I have an 83 year old male patient complaining of polyuria since the last three days. I
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
polyuria elderly evaluation
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Finding Sources
I now have comprehensive, authoritative information. Here is a complete clinical guide for your patient:
Polyuria in an 83-Year-Old Male — Clinical Approach
Step 1: Define It First
Polyuria = urine output >3 L/day. This must be distinguished from urinary frequency (frequent voiding of small volumes), which is common in elderly men due to benign prostatic hyperplasia. A 24-hour urine collection clarifies this.
Harrison's 22E: "It is often difficult for patients to distinguish urinary frequency from true polyuria, and a quantification of volume by 24-h urine collection may be needed."
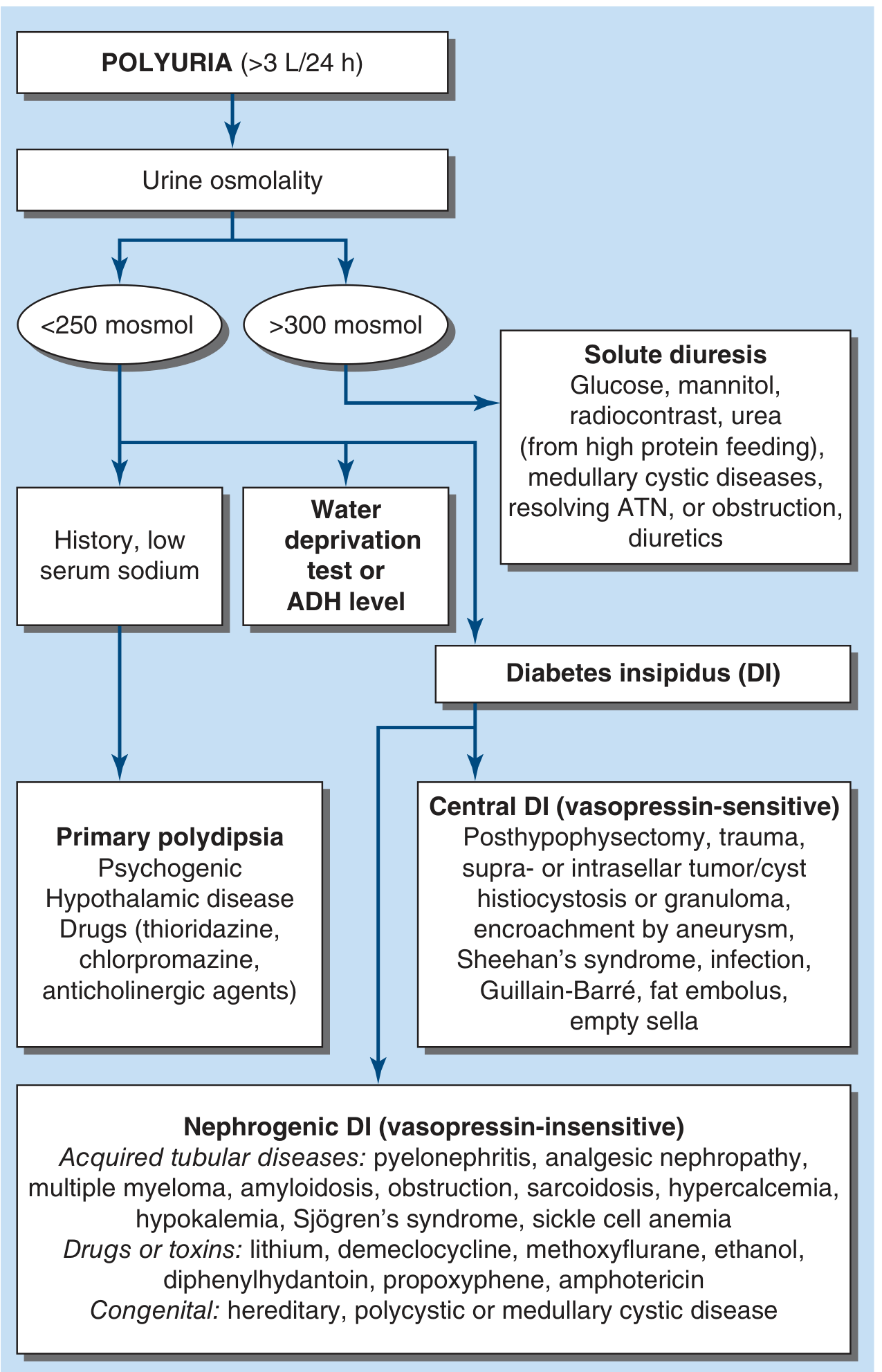
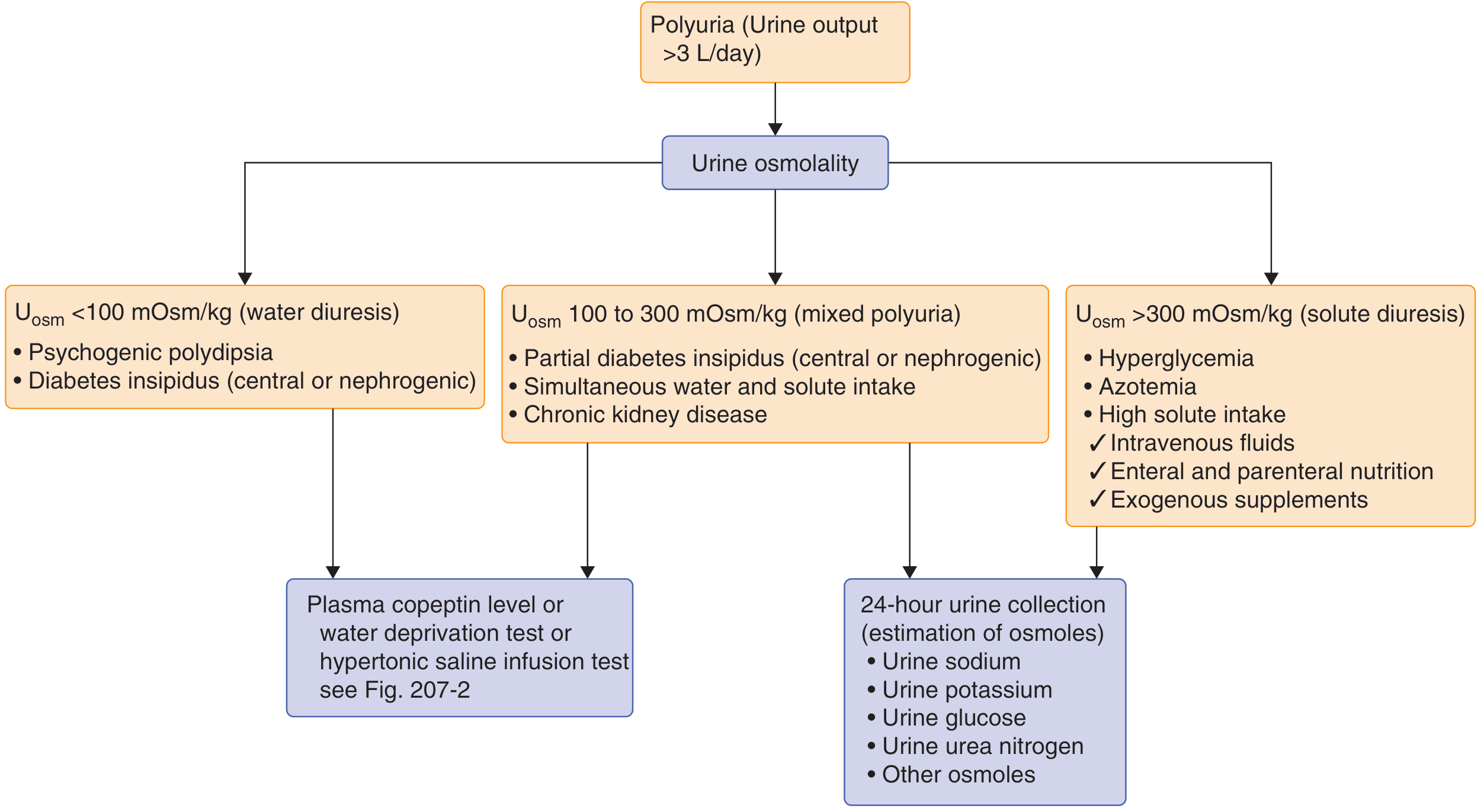
Step 2: The Two Pathophysiologic Categories
| Category | Urine Osmolality | Mechanism |
|---|---|---|
| Solute (osmotic) diuresis | >300 mOsm/kg | Poorly reabsorbable solute (glucose, urea, Na⁺) |
| Water diuresis | <100–250 mOsm/kg | Deficient or ineffective AVP (vasopressin) |
| Mixed | 100–300 mOsm/kg | Partial DI, CKD, simultaneous water + solute |
The pivotal first investigation is urine osmolality.
Step 3: Diagnostic Algorithm
Step 4: Differential Diagnosis
A. Solute (Osmotic) Diuresis — Urine Osm >300 mOsm/kg (Most common in elderly)
| Cause | Key Features in this Patient |
|---|---|
| Uncontrolled Diabetes Mellitus / Hyperglycemia ⭐ | Most common cause; glucosuria triggers osmotic diuresis; check BGL, HbA1c |
| Post-obstructive diuresis | Elderly male with BPH → acute urinary retention relieved → massive diuresis |
| Recovering AKI (resolving ATN) | Salt-wasting, obligatory polyuria during diuretic phase |
| High protein feeding / Urea load | Enteral nutrition, high protein diet → increased urea excretion |
| Mannitol / Radiocontrast | Recent procedural history? |
| Hypercalcemia | Malignancy, primary hyperparathyroidism (common in elderly) |
B. Water Diuresis — Urine Osm <250 mOsm/kg
| Cause | Key Features |
|---|---|
| Nephrogenic Diabetes Insipidus (NDI) | AVP-resistant; acquired tubular disease, drugs (lithium, demeclocycline), hypokalemia, hypercalcemia, CKD, myeloma |
| Central Diabetes Insipidus (CDI) | AVP-deficient; hypothalamic/pituitary pathology, head trauma, tumor, granuloma, inflammation |
| Primary Polydipsia | Compulsive water drinking; psychiatric disease or drugs (thioridazine, chlorpromazine, anticholinergics) |
Goldman-Cecil: "Nephrogenic DI can be caused by a mutation in the vasopressin V2 receptor or aquaporin-2 water channel. Drugs such as lithium commonly cause polyuria, which can be quite severe."
Step 5: Age-Specific Considerations at 83 Years
In this patient, prioritize these causes:
- Uncontrolled DM2 / new hyperglycemia — most prevalent
- Drugs: diuretics, lithium, demeclocycline — thorough medication review essential
- BPH with partial obstruction → post-obstructive diuresis
- Hypercalcemia from malignancy or hyperparathyroidism
- CKD with isosthenuria (urine Osm fixed ~300 mOsm/kg)
- Central DI from a new CNS lesion (metastasis, stroke) — always consider in acute onset
⚠️ Elderly caution: thirst perception is blunted in older adults. If AVP deficiency is present and the thirst mechanism is also impaired, severe hypernatremia and irreversible brain damage can rapidly supervene.
Step 6: Investigations
Initial (Essential)
| Test | Purpose |
|---|---|
| 24-hour urine volume | Confirm true polyuria (>3 L/day) |
| Urine osmolality (spot or 24h) | Pivotal branch point |
| Serum Na⁺, K⁺, Cl⁻, HCO₃⁻ | Electrolyte disturbance, hypernatremia, hypokalemia |
| Serum osmolality | Compare with urine Osm; calculate osmolar gap |
| Blood glucose / HbA1c | Rule out DM/hyperglycemia (most common) |
| Serum BUN / Creatinine / eGFR | Assess CKD, azotemia |
| Serum calcium | Rule out hypercalcemia |
| Urine dipstick + microscopy | Glycosuria, proteinuria, casts |
| Medication review | Lithium, diuretics, demeclocycline, contrast, mannitol |
Secondary (Based on Initial Results)
| Test | When to Order |
|---|---|
| Plasma copeptin (preferred) or water deprivation test | Urine Osm <250 mOsm/kg; distinguishes CDI vs NDI vs primary polydipsia |
| DDAVP (desmopressin) test (2 µg SC) | Suspected CDI — check urine Osm before and after; >50% rise = CDI |
| Serum PTH, PTHrP | Hypercalcemia found |
| MRI brain/pituitary | Suspected CDI |
| PSA, post-void residual ultrasound | Suspected obstructive uropathy/BPH |
| Serum protein electrophoresis / Bence-Jones | Suspected myeloma |
Harrison's 22E: "If sodium levels are above the normal reference range, the diagnosis of AVP deficiency or resistance is likely, and a test with desmopressin (2 µg) followed by a repeat measurement of urine osmolality will determine if hypotonic polyuria is due to AVP deficiency or AVP resistance."
Step 7: Management Principles
| Cause | Treatment |
|---|---|
| DM / Hyperglycemia | Glycemic control; insulin if HHS; hydration |
| Central DI | Desmopressin (DDAVP) intranasally or SC; treat underlying cause |
| Nephrogenic DI | Remove offending drug (lithium); thiazide diuretics + low-Na diet (paradoxical antidiuresis); NSAIDs (indomethacin) as adjunct |
| Primary polydipsia | Fluid restriction; treat underlying psychiatric disorder |
| Hypercalcemia | IV fluids, bisphosphonates, treat underlying cause |
| Post-obstructive diuresis | Careful IV fluid replacement (~50% of hourly output) to prevent hypovolemia |
Summary
Polyuria in 83M (3 days)
↓
First: Confirm with 24h urine volume
↓
Urine osmolality
├── >300 mOsm/kg → Solute diuresis → Check BG, Ca²⁺, medications, renal function
├── <250 mOsm/kg → Water diuresis → Copeptin/water deprivation test → CDI vs NDI vs polydipsia
└── 100–300 mOsm/kg → Mixed → CKD, partial DI
Most likely diagnosis in an 83-year-old male: osmotic diuresis from uncontrolled diabetes mellitus — but a full panel is mandatory before anchoring.
Sources: Harrison's Principles of Internal Medicine, 22E (2025); Goldman-Cecil Medicine; Brenner & Rector's The Kidney; Campbell-Walsh Urology
This is a shared conversation. Sign in to Orris to start your own chat.