Management of ARDS in pancreatitis patient in Critical care
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Now I have comprehensive information to provide a thorough answer. Let me synthesize everything.
ARDS Management in Pancreatitis — Critical Care
Pathophysiology Link
Acute pancreatitis causes ARDS through non-pulmonary (indirect) lung injury. Pancreatic necrosis triggers systemic inflammatory cytokines that recruit neutrophils, damage alveolar epithelium and pulmonary capillary endothelium, leading to increased permeability pulmonary edema and diffuse alveolar damage — the histopathologic hallmark of ARDS. This represents secondary (extrapulmonary) ARDS, which is common in surgical ICU settings alongside sepsis, haemorrhage, and transfusion injury.
— Current Surgical Therapy 14e, p. 1621; Harrison's Principles of Internal Medicine 22e, p. 2338
Berlin Definition — Staging (Mandatory for Management Decisions)
| Severity | PaO₂/FiO₂ | Ventilatory Setting |
|---|---|---|
| Mild | 200–300 | PEEP or CPAP >5 cmH₂O |
| Moderate | 100–200 | PEEP ≥5 cmH₂O |
| Severe | <100 | PEEP ≥5 cmH₂O |
Diagnosis requires all of:
- Onset within 1 week of a recognised insult (e.g. pancreatitis)
- Bilateral opacities on CXR or CT not explained by effusions/collapse/nodules
- Respiratory failure not fully explained by cardiac failure or fluid overload
- PaO₂/FiO₂ ratio as above
— Current Surgical Therapy 14e, p. 1621
Pressure-Volume Relationship — Rationale for Lung-Protective Ventilation
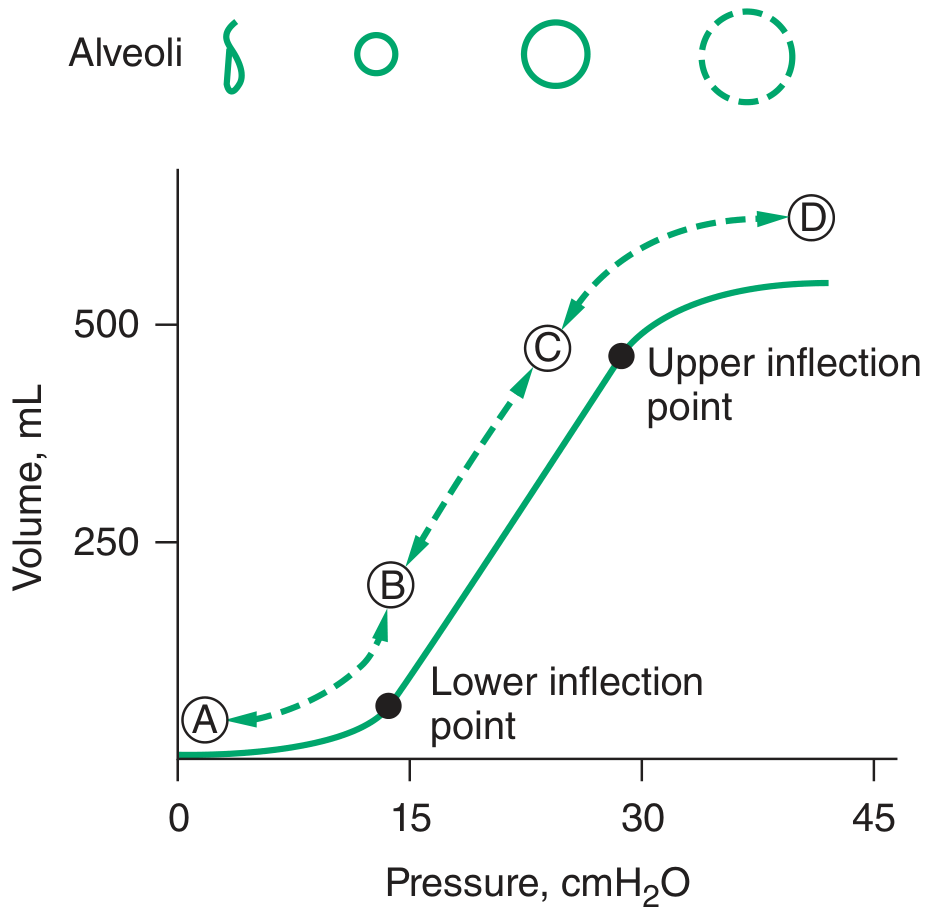
At the lower inflection point, collapsed alveoli begin to open. At the upper inflection point, alveoli become overdistended. PEEP should be set above the lower inflection point; tidal volumes should keep pressures below the upper inflection point.
— Harrison's Principles of Internal Medicine 22e, Fig. 311-5
Management Strategy
1. Oxygen Therapy (First Step)
- Target SpO₂ 90–96% — sufficient to meet metabolic demand while limiting oxygen toxicity
- High-flow nasal cannula (HFNC) preferred over NIV if patient has adequate neurological status, no hypercapnia, and no specific contraindications
- In pancreatitis patients: note abdominal distension may limit NIV tolerance
— Harrison's Principles of Internal Medicine 22e
2. Invasive Mechanical Ventilation — ARDSNet / Lung-Protective Ventilation
This is the cornerstone of ARDS management and has the strongest mortality evidence.
| Parameter | Target |
|---|---|
| Tidal volume (VT) | 4–8 mL/kg ideal body weight (6 mL/kg preferred) |
| Plateau pressure (Pplat) | ≤30 cmH₂O |
| PEEP | Titrated to maximise alveolar recruitment; avoid early high PEEP |
| PaO₂ goal | 55–80 mmHg |
| SpO₂ goal | 88–95% |
| Permissive hypercapnia | pH 7.30–7.45 acceptable; PaCO₂ >45 tolerated |
The landmark ARDSNet trial demonstrated mortality reduction from 39.8% → 31% with low tidal volume ventilation (6 vs 12 mL/kg IBW).
Ventilating with large tidal volumes causes "volutrauma" — repeated stretching and overdistention of injured, already-stiff alveoli worsens lung injury.
— Current Surgical Therapy 14e, p. 1621; Harrison's Principles of Internal Medicine 22e, p. 2338
3. Fluid Management — Conservative Strategy
A fluid-conservative strategy (targeting low CVP/PCWP) is associated with fewer ventilator days compared to a liberal fluid strategy in patients who have already been resuscitated from shock.
Specific challenge in pancreatitis: Early pancreatitis requires aggressive fluid resuscitation (often lactated Ringer's, 250–500 mL/hr). Once resuscitated and haemodynamically stable, transition to a conservative fluid strategy to limit ongoing pulmonary oedema. Avoid overresuscitation.
- Early resuscitation phase: correct hypovolaemia to maintain MAP ≥65 mmHg
- Post-resuscitation: target net-negative or neutral fluid balance
- CVP and PCWP monitoring can guide decisions
— Harrison's Principles of Internal Medicine 22e; Current Surgical Therapy 14e
4. Prone Positioning
- Indicated for severe ARDS (PaO₂/FiO₂ <150) refractory to initial ARDSNet strategies
- The PROSEVA trial demonstrated significantly reduced mortality in severe ARDS with ≥16 hours/day of prone positioning
- Mechanisms: redistribution of perfusion, improved V/Q matching, reduction of dorsal atelectasis
- In pancreatitis: abdominal distension and wounds/drains may complicate positioning — assess feasibility carefully
— Harrison's Principles of Internal Medicine 22e; Current Surgical Therapy 14e, p. 1621
5. Neuromuscular Blockade (NMB)
- Consider in moderate-severe ARDS (PaO₂/FiO₂ <150) when patient is dyssynchronous with the ventilator
- Cisatracurium (continuous infusion × 48h) studied in the ACURASYS trial — reduced 90-day mortality and barotrauma
- Prevents patient self-inflicted lung injury (P-SILI) from vigorous spontaneous efforts
- Monitor for ICU-acquired weakness — use only when indicated, for the shortest duration
— Harrison's Principles of Internal Medicine 22e
6. Rescue Therapies (Refractory Hypoxaemia)
When PaO₂/FiO₂ fails to improve despite the above:
| Rescue Measure | Notes |
|---|---|
| Pulmonary vasodilators | Inhaled nitric oxide (iNO) or inhaled prostacyclin — improve V/Q matching transiently; not shown to improve mortality but useful as bridges |
| Recruitment maneuvers | Stepwise PEEP escalation (PEEP 10→15→20→15→10 over 3 VT breaths each) — recruits collapsed alveoli; monitor haemodynamic effects |
| HFOV | High-frequency oscillatory ventilation — previously used; now generally avoided due to lack of benefit and possible harm in the OSCILLATE/OSCAR trials |
| VV-ECMO | Venovenous extracorporeal membrane oxygenation — definitive rescue when all else fails; allows ultra-low tidal volume "lung rest" (high PEEP, VT 4 mL/kg); best outcomes at specialised ECMO centres |
— Current Surgical Therapy 14e, p. 1621; Fishman's Pulmonary Diseases and Disorders
7. Pancreatitis-Specific Considerations
| Issue | Management |
|---|---|
| Abdominal compartment syndrome | Can co-occur, worsening respiratory mechanics; monitor intra-abdominal pressure; threshold >20 mmHg with organ failure warrants decompression |
| Pleural effusions | Common in pancreatitis (exudative, enzyme-rich); may worsen hypoxaemia; drain if haemodynamically or respiratorily significant |
| Sepsis | Secondary infected pancreatic necrosis is a major cause of deterioration and ARDS progression; early source control, targeted antibiotics |
| Nutrition | Enteral nutrition (nasojejunal preferred) should be commenced early; avoids gut mucosal atrophy and bacterial translocation contributing to systemic inflammation |
| Corticosteroids | Low-dose steroids (hydrocortisone 200 mg/day) indicated if concurrent septic shock; no proven benefit in ARDS alone without shock |
Outcomes
- Mild ARDS: ~35% mortality
- Severe ARDS: ~46% mortality
- Survivors face significant morbidity: physical deconditioning, cognitive impairment, and difficulty returning to work
— Current Surgical Therapy 14e, p. 1621
Summary Algorithm
Pancreatitis → ARDS suspected?
↓
Apply Berlin criteria → Grade severity
↓
All grades: HFNC/NIV if tolerated; O₂ target SpO₂ 90–96%
↓
Intubation needed? → ARDSNet ventilation
VT 6 mL/kg IBW | Pplat ≤30 cmH₂O | PEEP titration
Permissive hypercapnia | SpO₂ 88–95%
↓
Conservative fluid strategy (post-resuscitation)
↓
PaO₂/FiO₂ <150 (severe)?
→ Prone positioning ≥16 hrs/day
→ NMB (cisatracurium 48h)
→ Inhaled vasodilators
→ Recruitment maneuvers
↓
Refractory to all above?
→ VV-ECMO
This is a shared conversation. Sign in to Orris to start your own chat.