Why is creatinine used as a kidney function marker
Reading File
Searching the Web
creatinine kidney function marker physiology GFR
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have rich textbook content from multiple authoritative sources. Let me now compose a thorough answer.
Why Creatinine is Used as a Kidney Function Marker
What is Creatinine?
Creatinine is a small endogenous molecule (molecular weight 113 Da) produced in muscle as a byproduct of normal energy metabolism. Phosphocreatine - a high-energy phosphate reservoir in muscle cells - along with creatine is nonenzymatically converted at an almost steady rate (roughly 2% of total creatine per day) to creatinine. A secondary dietary source is creatine contained in ingested meat.
- Brenner and Rector's The Kidney, p. 3835
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 223
Why It Works as a GFR Marker - The Core Properties
Creatinine is the most widely used marker of glomerular filtration rate (GFR) for several interconnected reasons:
-
Fairly constant production rate - Because it derives from muscle mass (which is relatively stable day-to-day in a given person), its rate of entry into plasma is reasonably steady, which is a prerequisite for any useful filtration marker.
-
Not bound to plasma proteins - Creatinine circulates freely (unbound), so it passes through the glomerular filtration barrier without restriction.
-
Freely filtered at the glomerulus - Because it is small and unbound, virtually all plasma creatinine reaching the glomerulus is filtered into Bowman's capsule.
-
Not reabsorbed by the renal tubules - Once filtered, creatinine is not reclaimed by the tubule, so its urinary excretion faithfully reflects how much was filtered.
-
Inverse relationship with GFR - Serum creatinine does not directly measure GFR, but it varies inversely with GFR. When GFR falls (fewer nephrons filtering), creatinine accumulates in blood. When GFR is normal, creatinine is cleared efficiently and serum levels stay low.
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 223
- Brenner and Rector's The Kidney, p. 3837
The Practical Value
Because creatinine is endogenous, cheap to measure, and requires only a blood draw, it is far more convenient than the gold-standard GFR measurement (inulin clearance or iohexol, which require intravenous infusion and timed collection). Serum creatinine is also incorporated into validated estimating equations - particularly the CKD-EPI equation - that use creatinine plus age, sex, and race to calculate estimated GFR (eGFR) with reasonable accuracy across most patient populations.
- Comprehensive Clinical Nephrology, p. 2143
Limitations (Why it is "Imperfect")
Creatinine is useful but not perfect. Textbooks from multiple specialties flag the same set of limitations:
| Limitation | Effect |
|---|---|
| Tubular secretion | Proximal tubules actively secrete creatinine via organic cation transporters. This makes creatinine clearance overestimate true GFR by 10-40%, and worsens as GFR falls (secretion can contribute up to 50% of urinary creatinine in advanced renal failure). |
| Variable muscle mass | Elderly, malnourished, or cachectic patients produce less creatinine - so their serum creatinine can appear "normal" even with markedly reduced GFR. Women have lower creatinine at the same GFR than men for the same reason. |
| Dietary meat intake | A large meal of cooked meat can transiently raise serum creatinine by releasing preformed creatinine. |
| Rhabdomyolysis | Massive release of creatine/phosphocreatine from injured muscle converts to creatinine, causing a disproportionate rise unrelated to filtration. |
| Drugs | Trimethoprim, cimetidine, pyrimethamine, and dapsone block tubular secretion of creatinine, raising serum levels without any true change in GFR. |
| Extrarenal clearance | Gut bacteria degrade creatinine (creatininase activity), and this increases in chronic kidney failure, blunting the expected rise in serum creatinine. |
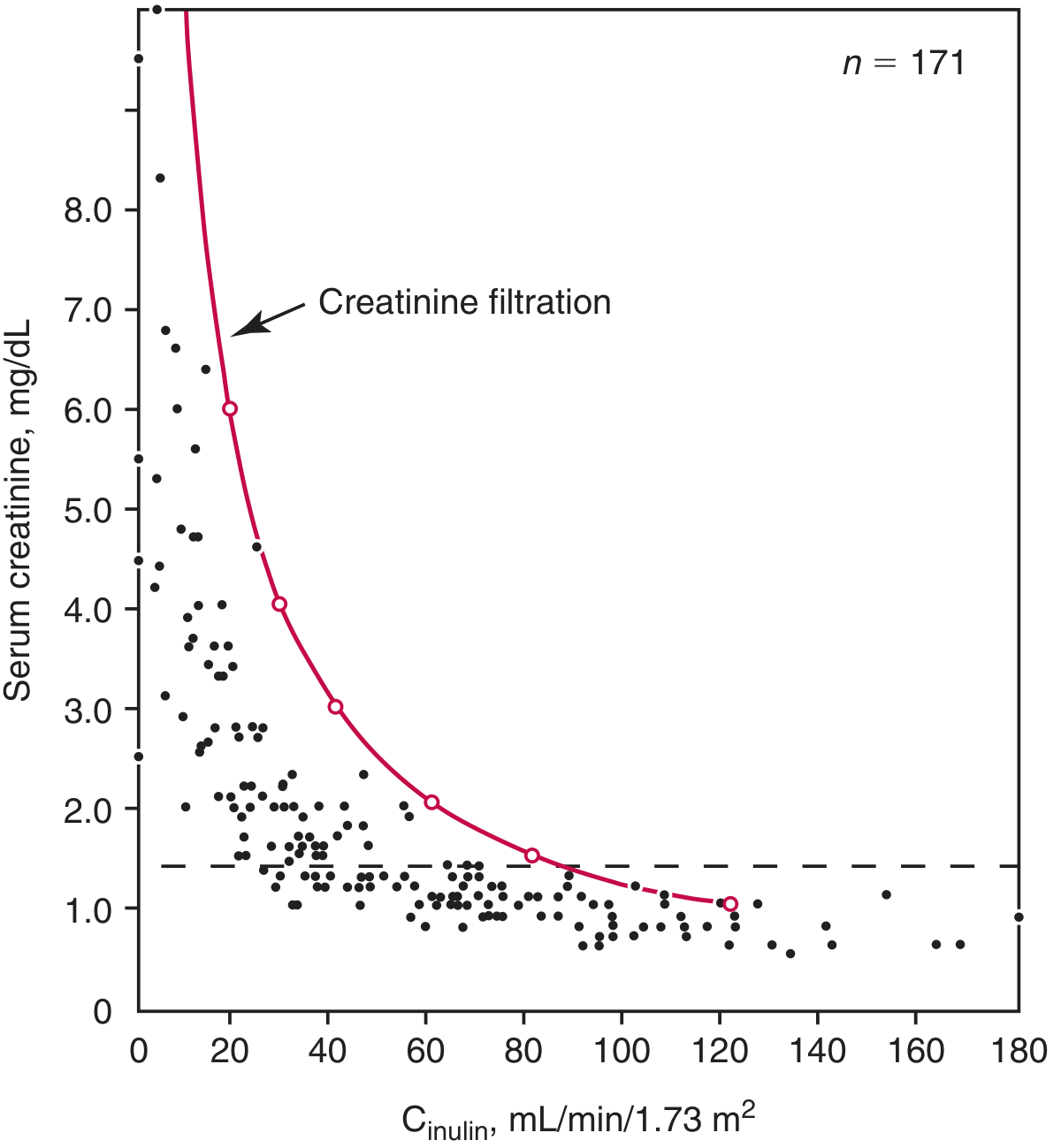
| Insensitivity at mild GFR reduction | Because of the hyperbolic inverse relationship between creatinine and GFR, significant kidney function can be lost before serum creatinine rises out of the "normal" range. A normal serum creatinine does NOT rule out CKD. |
- Brenner and Rector's The Kidney, pp. 3835-3848
- Tietz Textbook of Laboratory Medicine, p. 1098
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 223
The figure below (from Tietz) illustrates this hyperbolic relationship - note how at lower GFR values, small further drops in GFR cause large creatinine rises, while at higher GFR values, substantial GFR loss causes barely detectable creatinine changes:
Why Not Use Something Better?
Cystatin C - a protease inhibitor produced at a constant rate by all nucleated cells - is less influenced by muscle mass and is superior to creatinine as a GFR marker in several settings (elderly, muscle-wasting diseases, sickle cell nephropathy). The combined CKD-EPI equation using both creatinine and cystatin C is recognized as the most accurate eGFR estimate. However, cystatin C testing is more expensive and less universally available.
Inulin (the true gold standard) requires IV infusion, timed urine collection, and is impractical for routine clinical use.
Summary
Creatinine remains the dominant clinical kidney function marker because it is endogenous, freely filtered, not reabsorbed, cheap to measure, and its serum level reliably rises as GFR falls. Its limitations (tubular secretion, muscle-mass dependence, dietary variation) are well-characterized, and clinicians use eGFR equations and serial trends rather than isolated values to interpret results accurately.
Differentiate between creatine and creatinine
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching the Web
creatine vs creatinine structure function biochemistry difference
Finding Sources
I now have everything needed. Let me compile a comprehensive, well-structured comparison.
Creatine vs. Creatinine
These two molecules are closely related - creatinine is literally made FROM creatine - but they differ fundamentally in structure, function, location, and clinical significance.
At a Glance
| Feature | Creatine | Creatinine |
|---|---|---|
| Nature | Active metabolite | Waste product |
| Structure | Linear molecule; MW ~131 Da | Heterocyclic ring; MW ~113 Da |
| Synthesis | Biosynthesized (liver, kidney, pancreas) | Formed non-enzymatically from creatine/phosphocreatine in muscle |
| Reaction type | Reversible phosphorylation | Irreversible dehydration + loss of phosphate |
| Function | Energy storage/transfer (ATP regeneration) | No active function |
| Location | Primarily skeletal muscle (stored as phosphocreatine) | Plasma and urine |
| Protein binding | None | None |
| Renal handling | Reabsorbed by tubules | Freely filtered; small amount tubularly secreted |
| Clinical use | Supplement; creatine kinase (CK) as cardiac/muscle marker | GFR estimation, kidney function monitoring |
| Dietary source | Red meat, fish; oral supplementation | Derived from creatine in meat |
1. Structure
Creatine (methylguanidoacetic acid) is a linear guanidine compound - an open-chain molecule containing a guanidinium group and an acetic acid tail.
Creatinine is formed from creatine/phosphocreatine by spontaneous, irreversible, nonenzymatic dehydration and loss of phosphate - this cyclization creates a heterocyclic ring structure (an imidazolone ring). This is why the reaction is one-way: once the ring forms, it cannot reopen under physiological conditions.
- Harper's Illustrated Biochemistry, 32nd Ed, p. 323
2. Biosynthesis of Creatine
Creatine is synthesized in a two-step process across different organs:
- Step 1 (Kidney/Pancreas): Arginine + Glycine → Guanidoacetate (via arginine:glycine amidinotransferase, AGAT)
- Step 2 (Liver): Guanidoacetate + S-Adenosylmethionine (SAM) → Creatine (via guanidinoacetate methyltransferase, GAMT)
All three amino acids - glycine, arginine, and methionine (as SAM) - contribute atoms to creatine's structure.
- Harper's Illustrated Biochemistry, 32nd Ed, p. 323
Creatine is then transported in blood to skeletal muscle, heart, and brain, where it is phosphorylated by creatine kinase (CK) to form phosphocreatine (PCr).
3. Function of Creatine: The ATP Buffer
The key physiological role of creatine is energy storage via the phosphocreatine shuttle:
Creatine + ATP ⇌ Phosphocreatine + ADP (catalyzed by creatine kinase)
- At rest: Excess ATP phosphorylates creatine → builds up a phosphocreatine reservoir
- During intense exercise: Phosphocreatine rapidly donates its phosphate group back to ADP → regenerates ATP instantly, sustaining muscle contraction in the first ~10 seconds before glycolysis takes over
This makes creatine a critical short-term energy buffer in cells with high and fluctuating energy demands (skeletal muscle, heart, neurons).
- Ganong's Review of Medical Physiology, 26th Ed, p. 120
- Medical Physiology (Boron & Boulpaep), p. 3893
4. Formation of Creatinine: The Waste Product
Both free creatine and phosphocreatine undergo spontaneous (non-enzymatic, irreversible) cyclization in muscle:
Phosphocreatine → Creatinine + Phosphate (irreversible, nonenzymatic dehydration)
Creatine → Creatinine + H₂O (same spontaneous reaction)
The rate is approximately 2% of total creatine pool per day, which at normal muscle mass in a 70-kg man produces roughly 1.5 g/day (men) or 1.2 g/day (women) of creatinine.
Because this conversion rate is proportional to muscle mass, creatinine production (and hence 24-hour urinary creatinine excretion) is used to verify whether a complete 24-hour urine collection has been obtained.
- Harper's Illustrated Biochemistry, 32nd Ed, p. 323
- Brenner and Rector's The Kidney, p. 3835
5. Fate in the Body
| Creatine | Creatinine | |
|---|---|---|
| In muscle | Stored as phosphocreatine; used for ATP regeneration | Diffuses into plasma |
| In plasma | Transported to tissues; reabsorbed by tubules if filtered | Freely filtered at glomerulus |
| In kidneys | Tubules reabsorb creatine (it is conserved) | Not reabsorbed; small amount secreted by proximal tubule |
| End fate | Recycled (phosphorylated back to PCr) or slowly converted to creatinine | Excreted in urine |
This difference in renal handling is important: creatine is a valuable metabolic substrate and the kidney conserves it; creatinine is a terminal waste product and the kidney excretes it.
6. Clinical Significance
Creatine:
- Creatine kinase (CK/CPK) - the enzyme that phosphorylates creatine - is a key clinical marker. Elevated serum CK indicates muscle or cardiac cell damage (myocardial infarction, rhabdomyolysis, myositis).
- Oral creatine supplementation (popular among athletes) increases muscle phosphocreatine stores and can mildly raise serum creatinine - this is important to recognize so it is not misinterpreted as kidney disease.
- Rare genetic defects in creatine biosynthesis (AGAT or GAMT deficiency) cause intellectual disability and seizures - highlighting creatine's importance in the brain.
Creatinine:
-
Serum creatinine is the most widely used surrogate of GFR and kidney function (as discussed in the previous answer).
-
24-hour urinary creatinine excretion is used to validate completeness of urine collections.
-
Serum creatinine can be falsely elevated by drugs (trimethoprim, cimetidine) that block tubular secretion, or by a large meat meal - neither reflects true GFR change.
-
Brenner and Rector's The Kidney, pp. 3835-3848
-
Smith and Tanagho's General Urology, p. 2410
Key Conceptual Summary
Creatine is a living, functional energy currency in muscle - it stores and donates phosphate to keep ATP levels up during bursts of activity. Creatinine is its spent, irreversible end product - the molecular "exhaust" of creatine metabolism, with no biochemical role, passively excreted by the kidneys and used by clinicians as a window into renal filtration.
This is a shared conversation. Sign in to Orris to start your own chat.