post partum hemorrhage
Reading File
Finding Sources
Searching PubMed
"postpartum hemorrhage"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
postpartum hemorrhage uterine atony management algorithm
Reading File
Reading File
Now I have comprehensive information. Let me compile the full answer.
Postpartum Hemorrhage (PPH)
Definition
PPH has two definitions in current use:
- Classical: Blood loss >500 mL after vaginal delivery or >1,000 mL after cesarean delivery within 24 hours of birth
- ACOG (current): Blood loss ≥1,000 mL after any mode of delivery, or any volume of blood loss accompanied by signs/symptoms of hypovolemia within 24 hours of birth
Primary (early) PPH: Within the first 24 hours of delivery
Secondary (late) PPH: 24 hours to 6 weeks postpartum
Physiologically, plasma volume increases ~40% and RBC volume ~25% by end of third trimester — so up to 30% total blood volume loss may occur before blood pressure drops. The first sign may be only a mild rise in pulse rate.
Causes — The "4 Ts"
| Cause | Details | Frequency |
|---|---|---|
| Tone (Uterine atony) | Most common cause; >70% of PPH | ~70–80% |
| Tissue | Retained placenta/fragments, placenta accreta spectrum | ~10% |
| Trauma | Cervical/vaginal/perineal lacerations, uterine rupture, uterine inversion | ~20% |
| Thrombin | Coagulopathy (inherited or acquired/DIC) | Uncommon |
Secondary PPH causes: Uterine subinvolution at the placental site, retained placental tissue, genital tract wounds, uterogenital infection.
Risk Factors
For uterine atony:
- Uterine overdistension (polyhydramnios, multiple gestation, macrosomia)
- Prolonged or rapid labor
- High parity (multiparity)
- Labor induction/augmentation with oxytocin or tocolytics
- Chorioamnionitis / intraamniotic infection
- Hypertensive disorders of pregnancy
For cesarean PPH:
- Preeclampsia, obesity, general anesthesia, prior PPH
For uterine rupture:
- Prior uterine surgery (most significant risk factor)
- Obstructed labor, abnormal fetal lie, grand multiparity
Etiologies Table (Barash Clinical Anesthesia)
| Category | Specific Causes |
|---|---|
| Uterine atony | Overdistension, infection, prolonged labor |
| Genital tract trauma | Episiotomy, perineal/vaginal/cervical lacerations |
| Retained products | Placenta fragments |
| Abnormal placentation | Placenta accreta / increta / percreta |
| Coagulation defects | Inherited (e.g., vWD) or acquired (DIC) |
| Uterine inversion | Often from mismanaged 3rd stage |
Management
Initial Resuscitation (All PPH)
- Monitor vitals frequently; establish large-bore IV access
- Fluid resuscitation — Lactated Ringer's initially
- Labs: CBC, type & crossmatch, fibrinogen, PT/PTT, platelet count
- Supplemental oxygen to maximize cellular delivery
- Prepare for blood transfusion
- Non-pneumatic antishock garments can reduce blood loss in resource-limited or transport settings
Stepwise Treatment by Cause
🔴 Uterine Atony (Most Common)
Step 1 — Uterotonic Agents:
| Drug | Dose | Key Precautions |
|---|---|---|
| Oxytocin (1st line) | 20–30 U in 1L IV fluid ≤100 mU/min; or bolus 1–3 IU IV + infusion | Avoid rapid bolus (hypotension); risk of fluid overload |
| Methylergonovine | 0.2 mg IM q2–4h | Contraindicated in hypertension (causes vasoconstriction, severe HTN) |
| 15-methyl PGF₂α (Carboprost/Hemabate) | 250 μg IM q15–90 min (max 8 doses) | Avoid in asthma or cardiovascular disease; monitor O₂ sat |
| Misoprostol | 800–1000 μg rectally or transvaginally | For refractory cases; useful where IV drugs unavailable |
Step 2 — Bimanual uterine massage/compression alongside pharmacotherapy
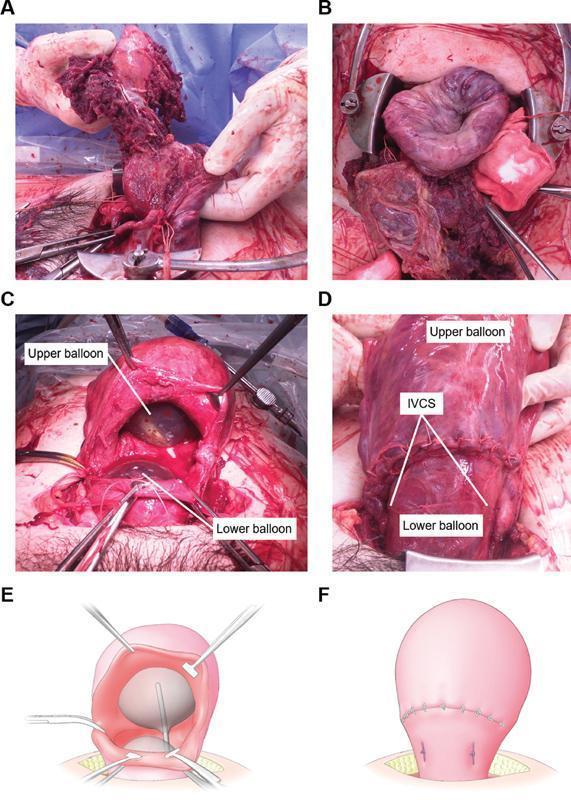
Step 3 — If uterus remains atonic after pharmacotherapy:
- Uterine tamponade: Bakri balloon or Foley catheter (especially for low placentation site bleeding)
- Uterine packing with sterile gauze
- Selective pelvic vessel embolization (where available)
Step 4 — Surgical (laparotomy):
- Identify occult intraabdominal sources
- Arterial ligation (uterine artery, internal iliac artery)
- B-Lynch compression sutures — vertical sutures that mechanically compress the uterine corpus
- Peripartum hysterectomy (last resort for refractory atony)
🔴 Retained Placenta / Accreta Spectrum
- Manual exploration and removal
- Placenta accreta: average blood loss 3–5 L; planned cesarean hysterectomy at 34–36 weeks under elective conditions is preferred
- Emergency embolectomy or hemostatic B-Lynch sutures if unplanned
🔴 Lacerations
- Repair under adequate light, exposure, and assistance
- Continuing hemorrhage with a firm fundus = look for hidden laceration
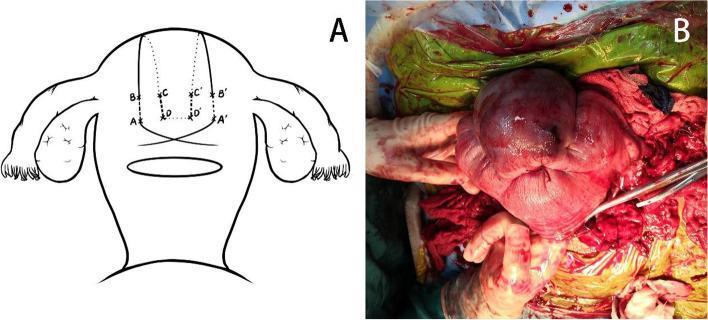
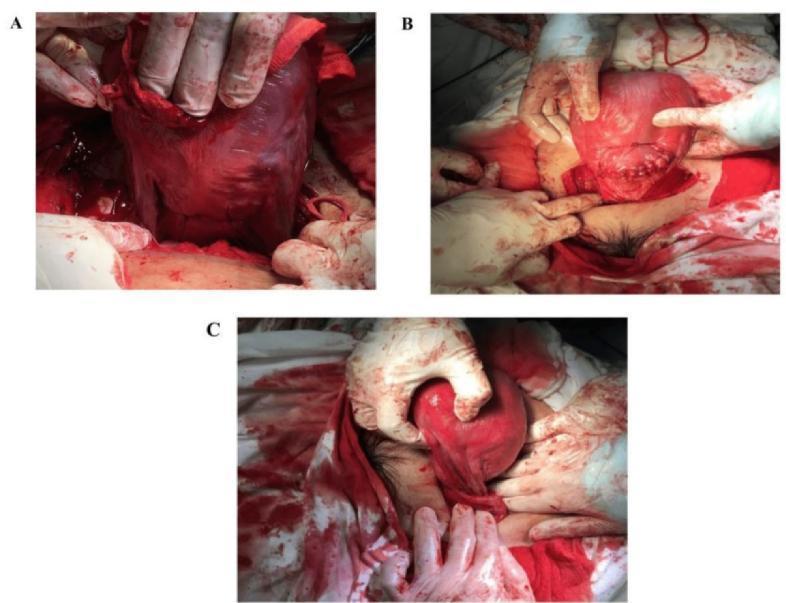
🔴 Uterine Inversion
- Immediate manual replacement: grasp uterus in palm, thumb anterior, push firmly back into abdominal cavity, hold for several minutes
- IV hydration briskly before and during
- Tocolytics (e.g., magnesium sulfate 0.25 mg IV) may assist repositioning
- Correction often requires general anesthesia
🔴 Uterine Rupture
- Immediate surgery; high maternal and fetal mortality risk
- Primary risk factor: prior cesarean section
Prevention (Active Management of 3rd Stage)
Active management reduces PPH incidence by two-thirds:
- Early oxytocin administration (10 U IM or dilute IV) after delivery of anterior shoulder or immediately after birth
- Early cord clamping and cutting
- Controlled cord traction
Surgical Images
Recent Evidence (2025 Cochrane Updates)
- Uterotonic agents (PMID 40237648): 2025 Cochrane network meta-analysis confirms combination uterotonics (e.g., oxytocin + carbetocin, or oxytocin + misoprostol) are superior to oxytocin alone for PPH prevention.
- Blood product transfusion (PMID 39911088): 2025 Cochrane review on optimal transfusion strategies in PPH management — current evidence base for ratio-based massive transfusion protocols remains limited in obstetric-specific populations.
Sources: Creasy & Resnik's Maternal-Fetal Medicine, Tintinalli's Emergency Medicine, Textbook of Family Medicine 9e, Barash Clinical Anesthesia 9e
This is a shared conversation. Sign in to Orris to start your own chat.