Using Miller's anaesthesiology book and morgan anesthesia book teach me tests to check different breathing circuits
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed from both textbooks. Let me compile a comprehensive, well-organized teaching response.
Tests to Check Breathing Circuits in Anaesthesia
Sources: Miller's Anesthesia 10e (MA) & Morgan and Mikhail's Clinical Anesthesiology 7e (MM)
Why This Matters
Misuse or malfunction of anaesthesia gas delivery equipment can cause major morbidity or mortality. The breathing circuit and low-pressure machine system are the most vulnerable areas for leaks. A routine, structured checkout before each use increases operator familiarity and confirms proper functioning. — MM, p. 146
Understanding the Two Separate Systems to Test
Before performing any tests, you must distinguish between two distinct areas:
| System | What It Includes | Test Type |
|---|---|---|
| Low-pressure system | Flow control valves → vaporizers → common gas outlet | Negative-pressure (suction bulb) test |
| Breathing circuit | From fresh gas inlet → inspiratory limb → patient Y-piece → expiratory limb → absorber → APL valve | Positive-pressure leak test |
Critical concept (Miller's, p. 2408): If the machine has an outlet check valve, positive pressure applied to the breathing circuit will NOT pass upstream into the low-pressure system. Therefore you cannot use a circuit pressure test to check for machine leaks — you need the negative-pressure suction bulb test instead.
Test 1 — Low-Pressure System Leak Test (Negative-Pressure / "Universal" Test)
When: Daily and whenever a vaporizer is changed
Responsible: Provider or technician
Indication for this test: Leaks in the low-pressure section (flow control valves through vaporizers to common gas outlet) can cause hypoxaemia or patient awareness under anaesthesia.
Procedure (MM, Table 4–3, Step 5 / MA, Item 8):
- Verify the machine master switch and all flow control valves are off
- Disconnect the breathing circuit from the common gas outlet
- Attach the specially configured suction bulb to the common (fresh) gas outlet
- Squeeze the bulb repeatedly until fully collapsed (this creates subatmospheric pressure in the low-pressure circuit, which opens any check valve present)
- Verify the bulb stays fully collapsed for at least 10 seconds
- Open one vaporizer at a time and repeat the squeeze-and-hold — this is critical because most vaporizer leaks are not detected unless the vaporizer is on
- Remove the suction bulb and reconnect the fresh gas hose
Pass: Bulb remains collapsed → no leak
Fail: Bulb re-inflates → ambient air is being drawn in through a leak
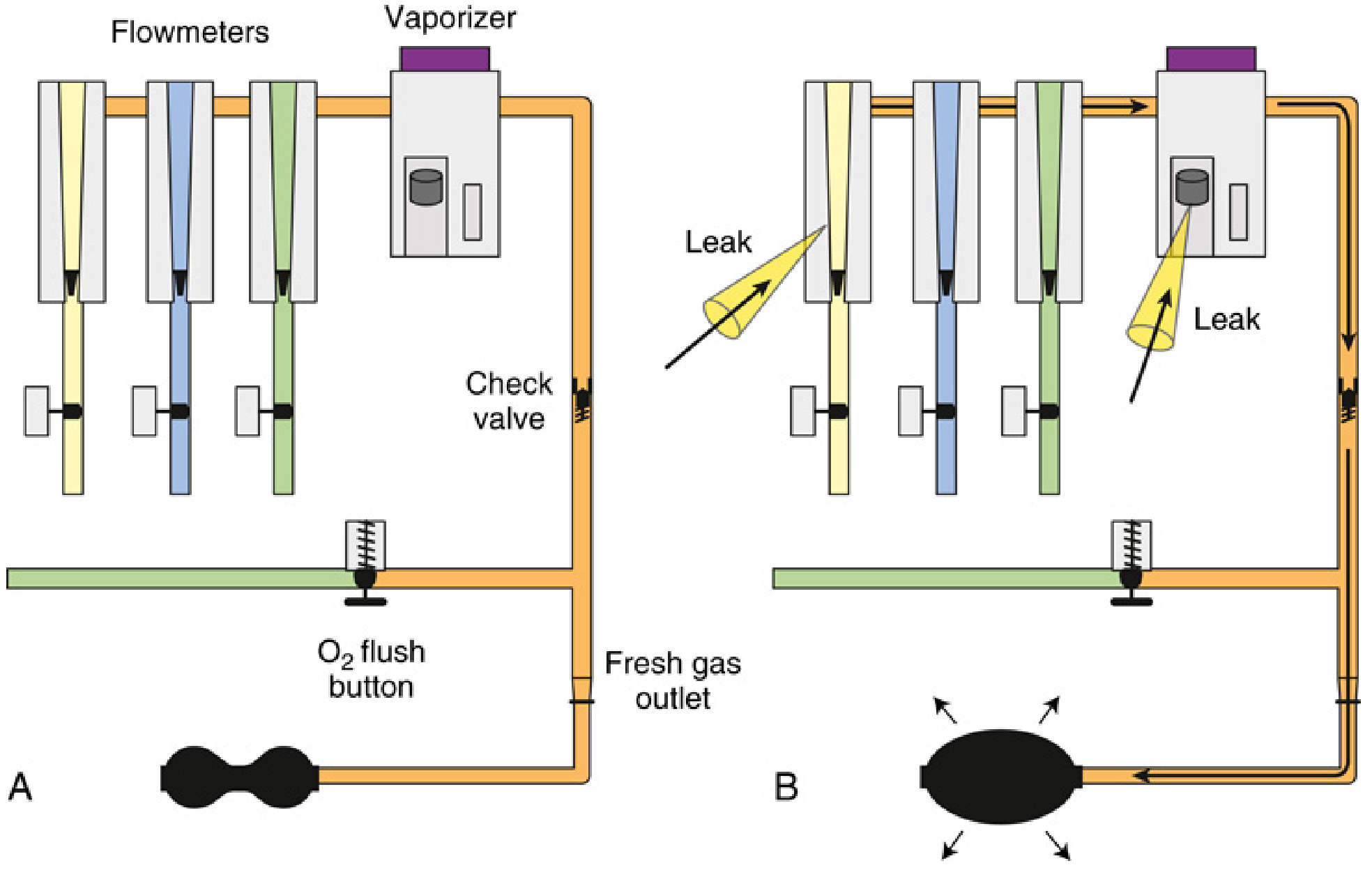
FIG. 20.54 from Miller's Anesthesia 10e — The negative-pressure "universal" low-pressure system leak test.
Why "universal"? This test works on machines both with and without a check valve, because it creates subatmospheric (negative) pressure, which naturally opens check valves. A positive-pressure test only works on machines without a check valve. — MA, p. 2409
Machines without accessible common gas outlet (many contemporary workstations): Negative-pressure manual testing cannot be performed. Instead, manual positive-pressure testing of vaporizers is done, or low-pressure testing is part of the automated checkout. — MA, p. 2409
Test 2 — Breathing Circuit (High-Pressure) Leak Test
When: Before each use
Responsible: Provider
Procedure (MM, Table 4–3, Step 11):
- Set all gas flows to zero (or minimum)
- Close the APL (pop-off) valve
- Occlude the Y-piece (the patient connection)
- Pressurize the breathing system to ~30 cm H₂O using the O₂ flush
- Ensure pressure remains fixed for at least 10 seconds
- Open the APL valve — verify that pressure decreases promptly
Pass: Pressure holds stable → circuit is intact
Fail: Pressure declines → leak within the breathing circuit
MM (p. 150): "A gradual decline in circuit pressure indicates a leak within the breathing circuit."
Where are leaks most commonly found? (MM, p. 150)
- Most common single site: Base plate of the CO₂ absorber
- Most common disconnection: Between the right-angle connector and the tracheal tube
- Other sites: open APL valve, cracked O₂ analyser adaptor, loose tubing, improperly adjusted scavenging unit, or leaks around the ETT cuff in an intubated patient
Test 3 — Oxygen Monitor Calibration Check
When: Before each use
Responsible: Provider
Procedure (MM, Table 4–3, Step 9):
- Remove the O₂ sensor and expose to room air → verify it reads 21%
- Verify the low-O₂ alarm is enabled and functioning
- Reinstall the sensor in the circuit
- Flush the breathing system with O₂ → verify the monitor reads >90%
Test 4 — Scavenging System Check
When: Daily
Responsible: Provider or technician
Procedure (MM, Table 4–3, Step 8 / MA, Item 9):
- Ensure proper connections between scavenging system and both the APL valve and ventilator relief valve
- Adjust the waste-gas vacuum (active systems: set to evacuate 10–15 L/min)
- Fully open the APL valve and occlude the Y-piece
- With minimum O₂ flow, allow scavenger reservoir bag to collapse completely → verify absorber pressure gauge reads ~0
- Activate the O₂ flush, allow reservoir bag to distend fully → verify absorber pressure gauge reads <10 cm H₂O
For active closed scavenging systems, also test the negative-pressure relief valve: turn off all flow control valves, occlude the Y-piece, then verify that the breathing pressure gauge does not go significantly negative. — MA, p. 2411
Test 5 — Unidirectional Valve Function Test
When: Before each use
Responsible: Provider
Unidirectional (one-way) valves ensure gas flows in one direction through the circle system. Their failure leads to rebreathing of CO₂.
Procedure (MM, Table 4–3, Step 12):
- Place a second breathing bag on the Y-piece (simulates patient lungs)
- Set appropriate ventilator parameters for the next patient
- Switch to automatic ventilation (ventilator) mode
- Turn ventilator on; fill bellows and breathing bag with O₂ flush
- Set O₂ flow to minimum
- Verify during inspiration: bellows delivers appropriate tidal volume
- Verify during expiration: bellows fills completely
- Set fresh gas flow to ~5 L/min; verify bellows and simulated lungs fill and empty appropriately without sustained pressure at end-expiration
- Check for proper action of unidirectional valves (watch that inspiratory valve opens on inhalation, expiratory valve opens on exhalation — neither should move in reverse)
- Switch back to manual (Bag/APL) mode and manually ventilate — ensure appropriate feel of resistance and compliance
- Remove the second breathing bag
Test 6 — Flowmeter Test (Hypoxic Mixture Prevention)
When: Daily
Responsible: Provider or technician (MM, Table 4–3, Step 7)
- Adjust the flow of all gases through their full range — check for smooth float operation and undamaged flow tubes
- Attempt to create a hypoxic O₂/N₂O mixture → verify the machine produces correct changes in flow or triggers an alarm (proportioning safety system)
Miller's also lists this as an additional check that some institutions include: "Testing the proportioning system by attempting to create a hypoxic oxygen–nitrous oxide mixture." — MA, p. 2419
Test 7 — Quick Intraoperative Leak Test (Back-Pressure Test)
When: Intraoperatively, if a leak is suspected
Responsible: Provider
MM (p. 149) describes this bedside test:
"Pinching the tubing that connects the machine's fresh gas outlet to the circuit's fresh gas inlet creates a back pressure that obstructs the forward flow of fresh gas from the anesthesia machine. This is indicated by a drop in the height of the flowmeter floats. When released, the floats should briskly rebound and settle at their original height."
- If floats drop when pinched → system upstream is intact (leak is in the circuit, not the machine)
- If floats do not drop → substantial leak exists within the machine upstream of the outlet
Summary: The FDA/Morgan Checkout Sequence in Full (Table 4–3)
| Step | System | Action |
|---|---|---|
| 1 | Emergency | Verify backup ventilation available |
| 2–3 | High-pressure | Check O₂ cylinder ≥½ full; pipeline pressures ~50 psig |
| 4–5 | Low-pressure | Check vaporizer fill; perform suction bulb negative-pressure leak test |
| 6–7 | Electrical/flowmeters | Master switch on; test all flowmeters; test hypoxic mix prevention |
| 8 | Scavenging | Test APL & ventilator relief connections; scavenger reservoir deflate/inflate test |
| 9 | O₂ monitor | Calibrate at 21% room air; verify reads >90% after O₂ flush |
| 10 | Breathing circuit status | Verify circuit complete, CO₂ absorbent adequate |
| 11 | Breathing circuit | Positive-pressure leak test: 30 cm H₂O, hold ≥10 sec |
| 12 | Ventilation/valves | Second bag test; unidirectional valve function; manual ventilation feel |
| 13 | Monitors | Calibrate capnograph, SpO₂, respiratory volume, pressure alarms |
| 14 | Final status | Vaporizers off, APL open, selector to Bag mode, flows to zero |
— MM, p. 147–148 (FDA Table 4–3) and MA pre-anaesthesia checkout recommendations
MS MAIDS — Final Pre-Induction Mnemonic (Miller's, p. 2420)
| Letter | Check |
|---|---|
| Machine | Checkout complete; vaporizers filled, closed, set to "O"; APL open; ventilator in manual mode |
| Suction | Adequate to clear the airway |
| Monitors | All standard monitors present and ready |
| Airway | Primary and backup airway equipment ready |
| Intravenous | IV lines, fluids, and equipment ready |
| Drugs | All medications available and labelled |
| Special | Any case-specific items ready |
Key Teaching Points
- Low-pressure leak test ≠ breathing circuit leak test — they test different zones with different techniques
- The negative-pressure (suction bulb) test is "universal" — it works regardless of whether a check valve is present; positive-pressure tests fail on machines with a check valve
- Each vaporizer must be tested individually during the low-pressure leak test
- Intraoperatively, a falling bellows is a sign of a leak exceeding fresh gas inflow — estimate leak size by increasing FGF until bellows height stabilises
- Automated machine self-tests do not replace all manual checks — no machine automatically checks everything; providers must understand exactly which items their machine's self-test covers — MA, p. 2309
This is a shared conversation. Sign in to Orris to start your own chat.