Write a case presebtation on ctev orthopedics
Reading File
Finding Sources
Finding Sources
Searching the Web
CTEV clubfoot case presentation orthopedics clinical features management Ponseti
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data from authoritative textbooks and clinical images. Here is the full case presentation:
Case Presentation: Congenital Talipes Equinovarus (CTEV) - Club Foot
PATIENT DETAILS
| Name | Baby Arjun S. (pseudonym) |
| Age | 3 days old |
| Sex | Male |
| Referred by | Neonatology ward |
| Chief Complaint | Abnormal position of both feet noted at birth |
PRESENTING COMPLAINT
Parents noticed that both feet of the newborn were turned inward and downward immediately after delivery. The deformity was present at birth and was also noted on antenatal ultrasound at 22 weeks of gestation.
HISTORY OF PRESENT ILLNESS
Baby Arjun was born at 38 weeks of gestation via normal vaginal delivery to a 26-year-old primigravida mother. Antenatal period was uneventful except for detection of bilateral foot deformity on the anomaly scan at 22 weeks. There was no history of oligohydramnios, polyhydramnios, or trauma during pregnancy. The mother denied use of selective serotonin reuptake inhibitors or other teratogenic medications. There was no family history of similar deformity.
Antenatal ultrasound report: "Bilateral foot deformities noted - clubfoot morphology; no associated neural tube defect or cardiac anomaly."
PAST HISTORY
- No significant past medical or surgical history
- Immunizations: BCG and Hepatitis B given at birth
FAMILY & SOCIAL HISTORY
- First child; no consanguinity
- Father is a non-smoker; maternal smoking history - denied
- No family history of clubfoot, skeletal dysplasia, or neuromuscular disorders
EXAMINATION
General Examination
- Neonate, alert, pink, well perfused
- Weight: 3.1 kg; length: 50 cm
- No dysmorphic features
- No cutaneous stigmata of spinal dysraphism (no sacral tuft, dimple, or hairy patch)
Systemic Examination
- Cardiovascular, respiratory, and abdominal examinations: normal
- Neurological: normal tone, reflexes, and spontaneous movements of all four limbs
Local Examination - Both Feet
Position: Both feet are held in a fixed, three-dimensional deformity.
Inspection:
- Hindfoot: Equinus (plantarflexion) and varus (inversion) - heel appears small and empty; calcaneal tuberosity proximally displaced toward fibular malleolus
- Midfoot: Cavus (elevated medial longitudinal arch); deep medial and single posterior crease
- Forefoot: Adduction (intoeing) and apparent supination; curved lateral border of foot
- Small calf noted bilaterally; feet are approximately half a size smaller than normal neonatal feet
- No skin ulceration
Palpation:
- Fixed deformity; not passively correctable to neutral position
- Heel feels "empty" - calcaneus is pulled upward by shortened tendo-Achilles
- Lateral head of talus palpable and fixed (not mobile)
- No local warmth, erythema, or bony tenderness
Movement:
- Active: spontaneous toe movements present
- Passive dorsiflexion: not possible beyond 20 degrees plantarflexion
- Passive eversion: restricted
- The foot cannot be brought to touch the anterior tibia (normally possible in a healthy neonate)
Mnemonic for components of deformity - CAVE:
| Component | Finding |
|---|---|
| C - Cavus | Elevated medial arch |
| A - Adductus | Forefoot adduction |
| V - Varus | Hindfoot varus |
| E - Equinus | Plantarflexed ankle |
CLINICAL IMAGE
Classic clubfoot deformity in a newborn - posterior view showing inversion, plantarflexion, and internal rotation of calcaneus with forefoot adduction:

DIAGNOSIS
Bilateral Congenital Talipes Equinovarus (CTEV) - Idiopathic
DIFFERENTIAL DIAGNOSES
| Condition | Distinguishing Feature |
|---|---|
| Positional/Postural clubfoot | Fully passively correctable to neutral; resolves by 3 months with physiotherapy |
| Metatarsus adductus | Forefoot adduction only; hindfoot normal; "banana-shaped" foot |
| Talipes calcaneovalgus | Dorsiflexed and everted foot; opposite deformity |
| Congenital vertical talus (CVT) | "Rocker-bottom" foot; dorsal dislocation of navicular |
| Neuromuscular CTEV | Associated spina bifida, arthrogryposis, myelomeningocele - must be excluded |
CLASSIFICATION / SEVERITY SCORING
Pirani Scoring System
Six parameters assessed, each scored 0, 0.5, or 1 (maximum = 6):
Midfoot signs (0-3):
- Curved lateral border
- Medial crease
- Lateral head of talus coverage
Hindfoot signs (0-3):
4. Posterior crease
5. Rigid equinus
6. Empty heel
Pirani Classification diagram showing scoring criteria:
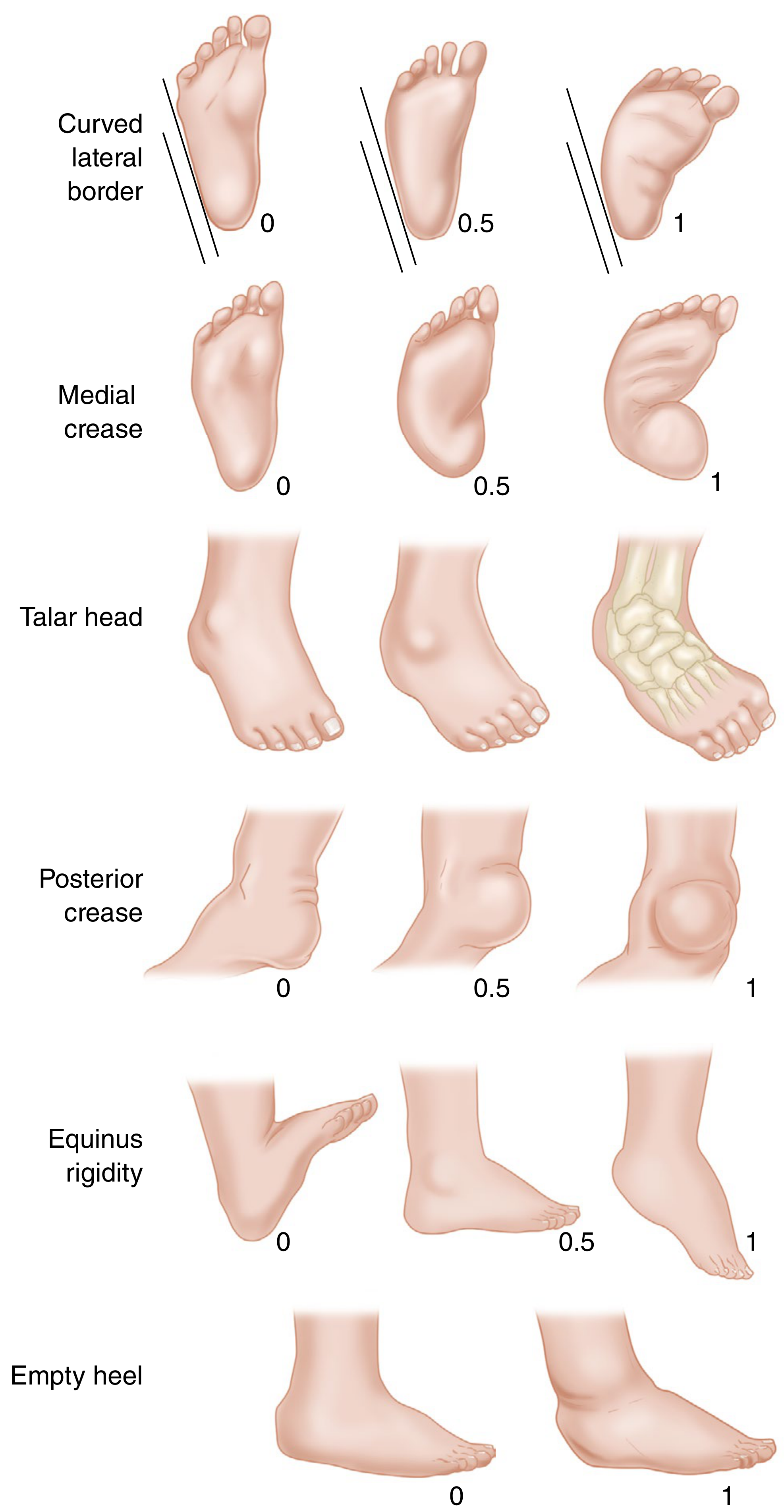
Score for this patient: Right foot 5/6, Left foot 5/6 (severe)
Dimeglio Classification (Alternative)
- Grade I: Soft, soft (<20°) - benign
- Grade II: Soft-stiff (20-45°) - moderate
- Grade III: Stiff-soft (>45°) - severe
- Grade IV: Stiff, stiff - very severe (teratologic)
This patient: Grade III (stiff-soft) bilaterally
INVESTIGATIONS
Radiological Evaluation
Standard radiographs in a non-ambulatory infant include:
- Simulated weight-bearing AP radiograph of both feet
- Stress dorsiflexion lateral radiograph of both feet
Key radiological angles:
| Angle | Normal | CTEV |
|---|---|---|
| AP Talocalcaneal (Kite's) angle | 20-40° | <20° (parallel talus and calcaneus) |
| Lateral Talocalcaneal angle | 25-50° | <35° |
| AP Talo-first metatarsal angle | 0-20° | Negative (adductus) |
| Tibio-calcaneal angle (lateral) | 10-40° | <10° (equinus) |
Findings in CTEV: On AP view, the talus and calcaneus appear parallel (convergent) rather than divergent. On lateral view, the talocalcaneal angle is reduced.
In a neonate with typical presentation like this one, X-rays are not routinely required before starting treatment. Ultrasound is an alternative radiation-free imaging modality.
Additional Workup (when indicated)
- MRI spine: If signs of spinal dysraphism (done in this case - normal)
- Chromosomal karyotype: If dysmorphic features suggest syndromic cause
- Echocardiogram: If associated cardiac anomaly suspected
PATHOLOGY & PATHOGENESIS
The four basic components (CAVE) arise from a complex three-dimensional deformity of the tarsal bones. Key anatomical changes (from Campbell's Operative Orthopaedics, 15th Ed.):
- The talonavicular joint is subluxed - navicular displaced medially on the talar head
- The calcaneus rotates under the talus - calcaneal tuberosity approaches the fibular malleolus
- Soft-tissue contractures affect the calcaneofibular ligament, posterior tibial tendon sheath, gastrocsoleus, and plantar ligaments - these are shortened, thickened, and contain contractile myofibroblasts
- The vascular supply via dorsalis pedis may be diminished
- If untreated, adaptive bony changes develop; joints may fuse or develop degenerative arthritis in adulthood
Etiology theories:
- Primary germplasm defect in the talus causing continued plantarflexion
- Primary neuromuscular soft-tissue abnormality causing secondary bony changes
- Vascular anomaly (hypertrophic anterior tibial artery noted in some cases)
- Abnormal type I:II muscle fiber ratio documented in clubfeet
MANAGEMENT
Goals of Treatment
- Achieve a plantigrade, functional, pain-free foot
- Maintain correction long-term
- Avoid the consequences of untreated CTEV: callosities, skin breakdown, difficulty walking, cosmetic and psychological impact
1. Non-Operative Treatment (First-Line)
Ponseti Method (Gold Standard)
The Ponseti method corrects foot deformity in >95% of idiopathic cases without formal surgical release. Treatment begins within the first few weeks of life. (Bailey & Love's Surgery, 28th Ed.)
Sequence of casts applied (one per week):
| Cast | Correction Targeted |
|---|---|
| Cast 1 | Supinate forefoot - correct cavus (elevate first ray first) |
| Casts 2-4 | Abduct forefoot around talar head fulcrum with counter-pressure on lateral talar head; correct varus |
| Final casts | Full abduction; then correct equinus |
Key principle: The head of the talus is the fulcrum around which the rest of the foot rotates. The forefoot is never pronated - this would worsen the cavus.
Achilles tenotomy:
- Required in approximately 80-90% of cases to correct the residual equinus
- Performed percutaneously as an outpatient procedure under local anesthesia
- Cast applied for 3 weeks post-tenotomy to allow healing
Denis Browne splint (foot abduction brace):
- Applied after full correction
- Worn full-time (23 hrs/day) for 3 months, then at night and nap time for 3-4 years
- Non-compliance is the primary cause of relapse - parents must be extensively counseled
- Recurrence rate: 10-30%; most recurrences can be treated with repeat casting
2. Operative Treatment
Indicated for:
- Failure of conservative management
- Relapsed/resistant cases
- Neuromuscular CTEV (e.g., spina bifida, arthrogryposis)
- Older children with neglected CTEV
Procedures:
- Anterior tibial tendon transfer (ATTT): For dynamic supination/relapse with muscle imbalance; tendon transferred from medial cuneiform to lateral cuneiform or cuboid
- Posteromedial release (Turco procedure / Carroll procedure): Now rarely needed; addresses soft-tissue contractures of posterior, medial, and subtalar joints; risk of overcorrection (flatfoot) and stiffness
- Ilizarov external fixator / gradual distraction: For neglected, rigid, or older cases
- Triple arthrodesis: For severe, rigid, painful adult residual deformity
TREATMENT PLAN FOR THIS PATIENT
- Initiate Ponseti casting within first week of life - bilateral above-knee plaster casts, changed weekly for 5-7 sessions
- Weekly follow-up for cast changes; monitor for skin complications under cast
- Percutaneous Achilles tenotomy at approximately 5-6 weeks (anticipated) under LA
- Denis Browne abduction brace post-correction - full-time for 3 months, then nocturnal for 3-4 years
- Parent counseling on brace compliance - the most important factor in preventing relapse
- MRI spine - already completed; normal result
- Long-term follow-up into adolescence to monitor for recurrence, limb length discrepancy, and tibial torsion
PROGNOSIS
- Idiopathic CTEV treated with Ponseti method: Excellent; >95% correction without major surgery
- Small calf and foot remain smaller than the contralateral side in unilateral cases - does not affect function
- Mild tibial shortening may become apparent with growth
- Untreated CTEV is "cosmetically, functionally, and psychologically unacceptable" - every effort must be made to correct the deformity (Campbell's Operative Orthopaedics)
- Neuromuscular CTEV has a worse prognosis with higher recurrence
DISCUSSION POINTS
Q: How does CTEV differ from positional clubfoot?
In true CTEV the deformity is fixed and not passively correctable. Positional (postural) clubfoot results from intrauterine moulding and is fully correctable to neutral. The postural type must normalize by 3 months; if not, it is reclassified as structural.
Q: Why is the heel "empty" in CTEV?
The calcaneus is pulled proximally by the shortened tendo-Achilles, bringing the calcaneal tuberosity up toward the fibular malleolus. The heel pad is small and the calcaneus is not palpable in the expected position.
Q: What is the role of genetics?
Most cases are idiopathic with multifactorial inheritance. Bilateral CTEV carries a higher risk of syndromic association. A family history of CTEV increases risk significantly. Known risk factors include paternal and maternal smoking, maternal obesity, and amniocentesis.
Q: When should surgery be offered?
Surgery is now reserved for failed or relapsed cases and neuromuscular causes. The historical posteromedial release (Turco/Carroll procedure) has largely been replaced by the Ponseti method due to superior long-term outcomes and fewer complications.
REFERENCES
- Campbell's Operative Orthopaedics, 15th Ed. 2026 - Chapter 31: Anomalies of the Foot (CTEV section)
- Bailey & Love's Short Practice of Surgery, 28th Ed. - Chapter 44: Congenital talipes equinovarus
- Miller's Review of Orthopaedics, 9th Ed. - Clubfoot (Congenital Talipes Equinovarus), p. 238
- Schwartz's Principles of Surgery, 11th Ed. - Congenital Talipes Equinovarus
This case presentation was prepared for orthopedic clinical teaching. The Ponseti method remains the gold standard for management of idiopathic CTEV with a success rate exceeding 90%. Long-term brace compliance is the single most important determinant of outcome.
This is a shared conversation. Sign in to Orris to start your own chat.