Teach me about nerve supply of scalp and how to give nerve blocks for hair transplant
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
Teach me about nerve supply of scalp and how to give nerve blocks for hair transplant
Reading File
Finding Sources
Finding Sources
Searching the Web
nerve blocks scalp hair transplant technique supraorbital supratrochlear occipital
Finding Sources
Finding Sources
Reading Web Page
https://clinista.com/scalp-block-and-proper-anesthesia-appli…
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Searching PubMed
scalp nerve block hair transplant anesthesia technique
I now have all the information needed to write a thorough, well-illustrated answer. Here it is:
Nerve Supply of the Scalp and Nerve Blocks for Hair Transplant
Part 1 - Anatomy of Scalp Innervation
The scalp receives sensory innervation from two sources: the trigeminal nerve (CN V) anterolaterally and the cervical plexus posteriorly. Classically, 7 nerves on each side supply the scalp.
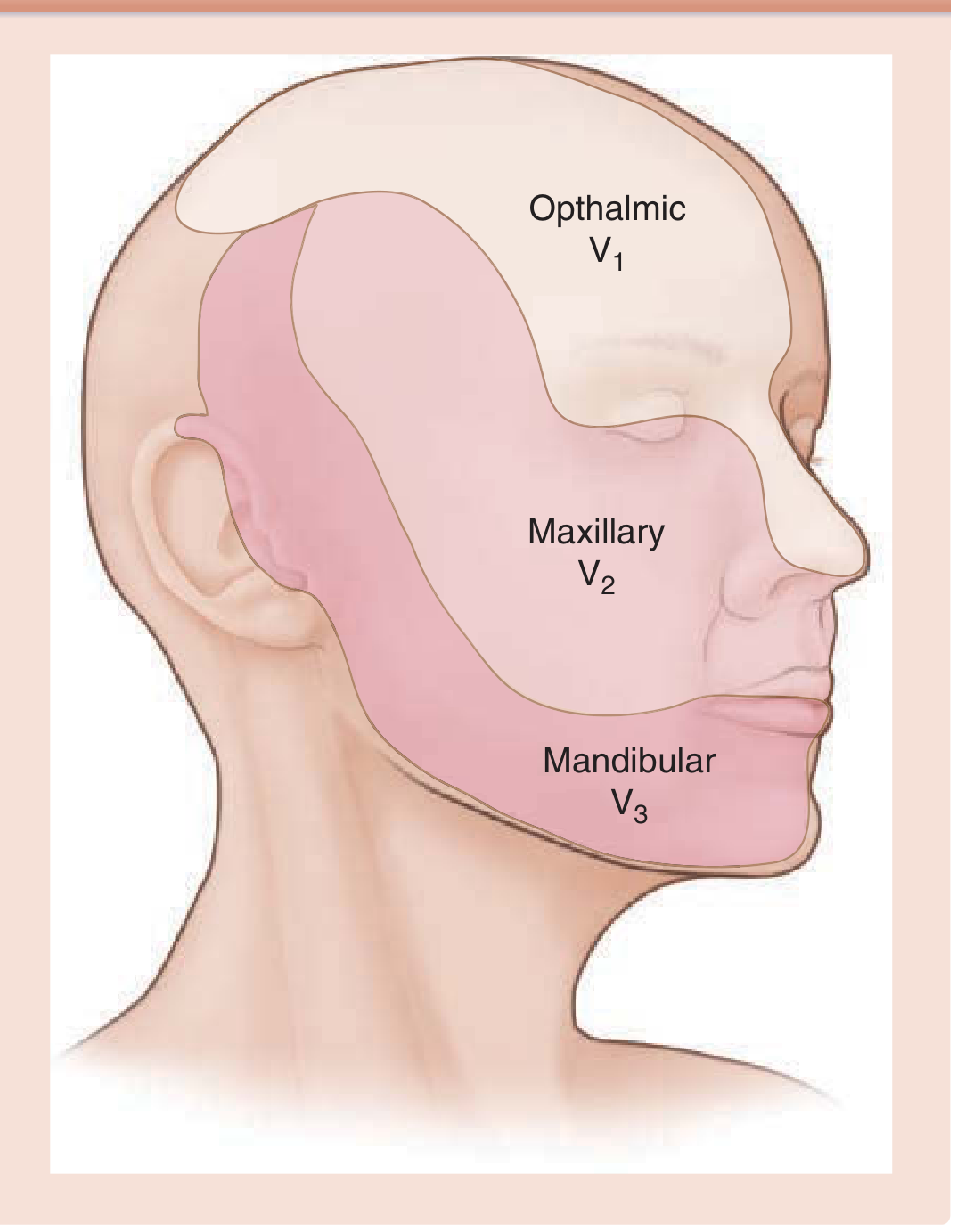
Here is the trigeminal distribution map:
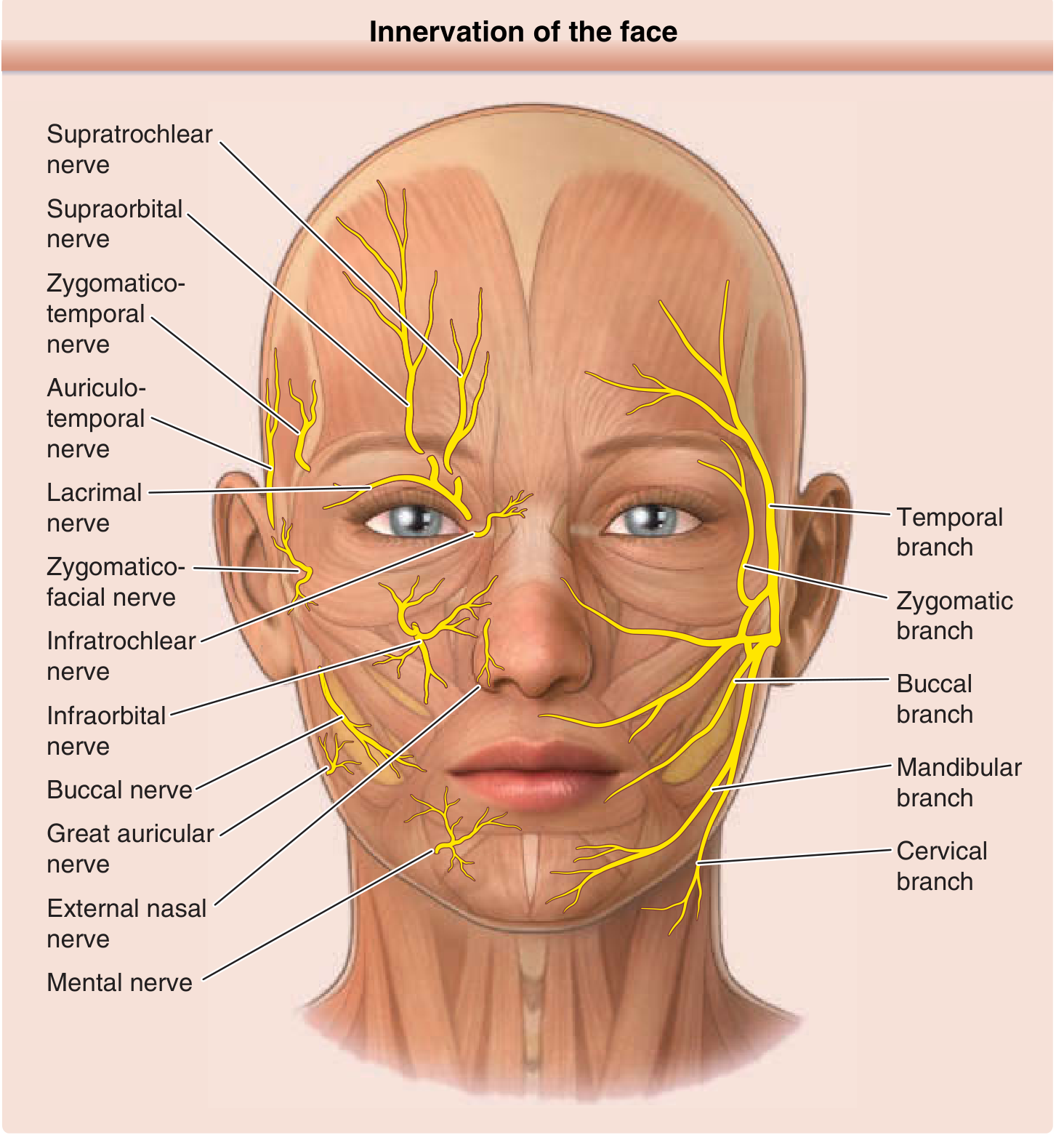
And the detailed nerve anatomy of the face and scalp:
The 7 Scalp Nerves (by region)
| Nerve | Origin | Region Supplied |
|---|---|---|
| Supraorbital | V1 (Ophthalmic) via frontal nerve | Forehead, anterior and vertex scalp to lambdoid suture |
| Supratrochlear | V1 (Ophthalmic) via frontal nerve | Medial forehead and anterior scalp |
| Zygomaticotemporal | V2 (Maxillary) via zygomatic nerve | Anterior temporal region, small strip of forehead |
| Auriculotemporal | V3 (Mandibular) | Posterior temple, temporoparietal scalp, anterior auricle |
| Greater occipital | Dorsal ramus of C2 | Posterior scalp to vertex |
| Lesser occipital | Ventral rami of C2, C3 | Scalp lateral to ear, posterior auricle |
| Great auricular | Ventral rami of C2, C3 | Mastoid area, inferior posterior scalp, auricle |
(Sources: Fitzpatrick's Dermatology; Roberts & Hedges' Clinical Procedures; Miller's Anesthesia)
Regional Breakdown
Anterior Scalp (V1 territory)
The frontal nerve (largest branch of V1) travels through the superior orbital fissure and divides into:
- Supraorbital nerve - exits via the supraorbital notch/foramen (located along the midpupillary line at the orbital rim). Divides into a superficial branch (forehead skin through frontalis) and a deep branch (scalp to lambdoid suture, ~2-3 cm lateral to midline).
- Supratrochlear nerve - exits via the supratrochlear notch, ~1 fingerbreadth medial to the supraorbital nerve. Supplies the medial forehead and anterior scalp near midline.
Temporal Scalp (V2 + V3 territory)
- Zygomaticotemporal nerve (V2) - pierces the temporalis fascia to supply the anterior temporal hairline. It ramifies as it exits, so both subcutaneous and subfascial injections are needed for a reliable block.
- Auriculotemporal nerve (V3) - runs with the superficial temporal artery, just anterior to the tragus. Supplies the large posterior temporal area and most of the hairline above the ear.
Posterior Scalp (Cervical plexus)
- Greater occipital nerve (C2 dorsal ramus) - the workhorse of posterior scalp anesthesia. Becomes superficial at the inferior border of obliquus capitis inferior, runs medial to the occipital artery, and ascends to the vertex.
- Lesser occipital nerve (C2 ventral ramus) - runs along the posterior border of the sternocleidomastoid, supplies the scalp behind the ear.
- Great auricular nerve (C2/C3 ventral rami) - largest ascending branch of the cervical plexus, supplies the mastoid area, posterior auricle, and adjacent scalp.
All these nerves travel in the subcutaneous layer, above the epicranial aponeurosis (galea aponeurotica). This is the critical anatomical point - injections must reach the subcutaneous plane.
Part 2 - Nerve Blocks for Hair Transplant
Hair transplant (FUE or FUT) requires anesthesia of both the donor area (posterior/occipital scalp) and the recipient area (frontal/vertex/temporal scalp). A complete scalp block using all 7 nerves is the standard approach.
Equipment
- 25-gauge needle, 5-10 mL syringes
- Local anesthetic: lidocaine 1-2% with epinephrine 1:100,000 to 1:200,000 (epinephrine reduces bleeding and prolongs duration)
- Alternatively: bupivacaine 0.25-0.5% for longer procedures; ropivacaine 0.3-0.5% is also used
- Total volume needed: approximately 20-30 mL for a complete ring block
The Ring Block Concept
A circumferential subcutaneous infiltration of local anesthetic is drawn along an imaginary line from the occipital protuberance anteriorly along the upper border of the ear to the eyebrows, connecting all 7 nerve territories. This "ring" blocks all nerves as they ascend from below.
Nerve-by-Nerve Block Technique
1. Supraorbital Nerve Block
- Landmark: Palpate the supraorbital notch/foramen at the orbital rim, in the midpupillary line (~2.5 cm from midline)
- Technique: Insert a 25-gauge needle just above the eyebrow at the orbital rim. Inject 2-3 mL of LA subcutaneously.
- Coverage: Forehead and anterior scalp to the vertex
2. Supratrochlear Nerve Block
- Landmark: ~1 fingerbreadth (1 cm) medial to the supraorbital notch, above the medial eyebrow
- Technique: From the same insertion point used for the supraorbital block, redirect the needle medially through the same skin puncture. Inject 2-3 mL subcutaneously. This is essentially a medial extension of the supraorbital block.
- Coverage: Medial forehead, nasal root area of the scalp
These two blocks together anesthetize the entire anterior scalp from hairline to vertex.
3. Zygomaticotemporal Nerve Block
- Landmark: Lateral edge of the supraorbital margin, extending down toward the zygomatic arch
- Technique: Because the nerve pierces the temporalis fascia, inject 3-5 mL both subcutaneously AND deep to the temporalis fascia (bifascial injection). Begin at the lateral orbital margin and extend toward the zygomatic arch.
- Coverage: Anterior temporal hairline region
4. Auriculotemporal Nerve Block
- Landmark: 1-1.5 cm anterior to the superior border of the tragus, at the level of the root of the zygoma, where the superficial temporal artery is palpable
- Technique: Palpate and avoid the superficial temporal artery. Inject 2-3 mL subcutaneously anterior to the tragus. Aspirate before injecting.
- Coverage: Temporal scalp, temporoparietal area above the ear
- Caution: Close proximity to the superficial temporal artery - mandatory aspiration before injection
5. Greater Occipital Nerve Block
- Landmark: The nuchal line (imaginary line from external occipital protuberance to mastoid process). The greater occipital nerve lies just medial to the occipital artery, approximately 2.5-3 cm lateral to the external occipital protuberance (or halfway between the EOP and the mastoid process)
- Technique: Palpate the occipital artery as your primary landmark. Insert a 23-25 gauge needle and inject 3-5 mL subcutaneously after careful aspiration (the occipital artery runs alongside the nerve)
- Coverage: Entire posterior scalp up to the vertex
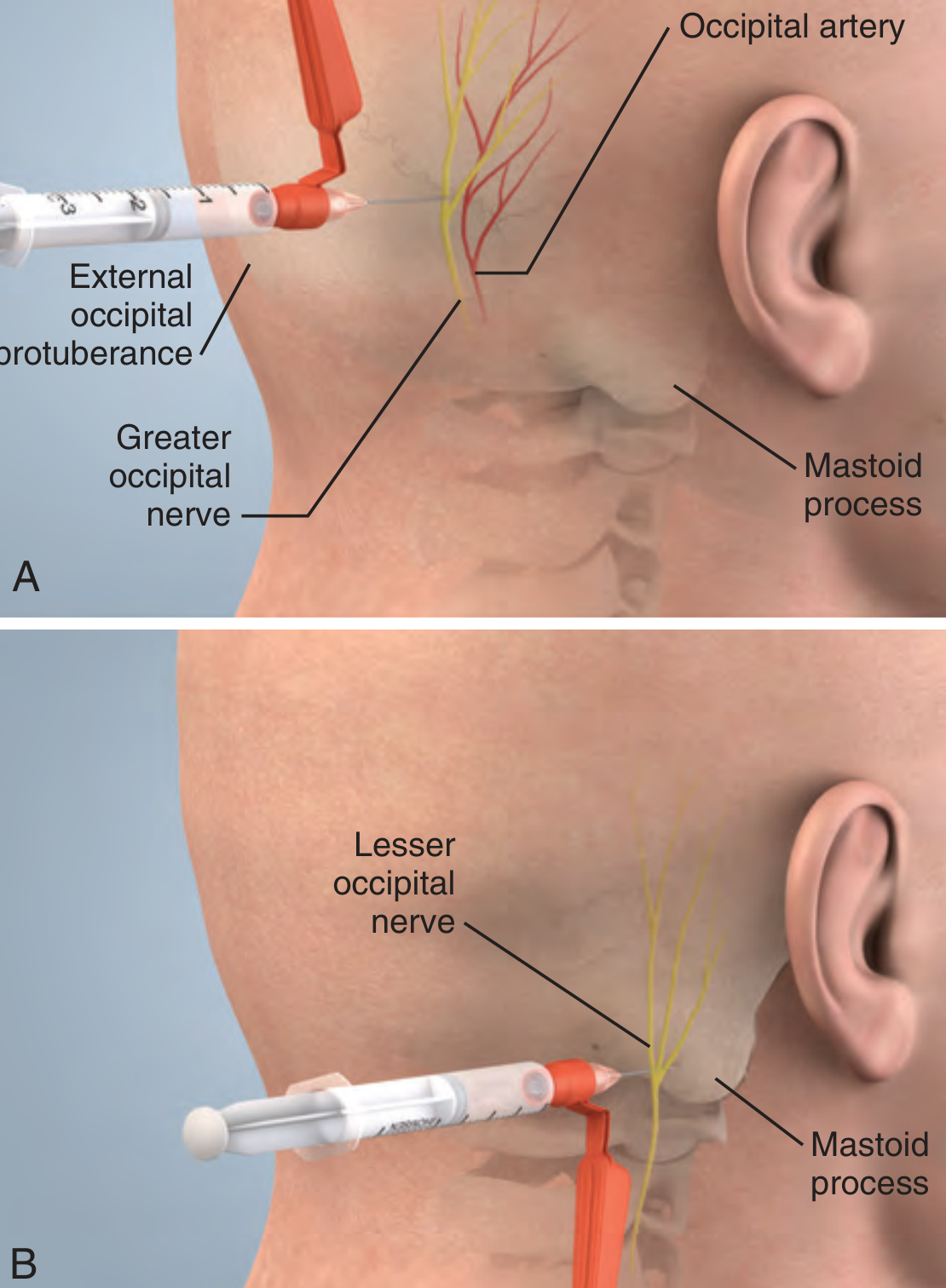
6. Lesser Occipital Nerve Block
- Landmark: 2.5-3.5 cm lateral and 1-2 cm caudal to the greater occipital nerve injection point, along the posterior border of the mastoid process
- Technique: Fan-like injection of 2-3 mL subcutaneously in this area
- Coverage: Scalp lateral to the ear, posterior to the auricle
7. Great Auricular Nerve Block (if needed)
- Landmark: Along the posterior border of the sternocleidomastoid muscle, at the level of the mastoid tip
- Technique: Subcutaneous infiltration of 2-3 mL
- Coverage: Mastoid area and inferior posterior auricle - this nerve rarely encroaches on the main hair transplant field and is sometimes omitted
Summary of Injection Points
ANTERIOR: Supratrochlear [medial] ← → Supraorbital [lateral]
↓ (both above eyebrow)
TEMPORAL: Zygomaticotemporal (at lateral orbital rim)
Auriculotemporal (1 cm anterior to tragus)
POSTERIOR: Greater occipital (3 cm lateral to EOP, medial to occipital artery)
Lesser occipital (2.5-3 cm further lateral from GON point)
Great auricular (along posterior SCM)
Practical Tips for Hair Transplant
| Point | Detail |
|---|---|
| Epinephrine is mandatory | 1:100,000 to 1:200,000 - reduces bleeding from the highly vascular scalp and prolongs anesthesia duration |
| Subcutaneous injection | All nerves run above the galea - injecting too deep misses them and causes unnecessary bleeding |
| Aspiration before every injection | The scalp is highly vascular; intravascular injection (especially at occipital artery and superficial temporal artery) causes systemic toxicity |
| Ring block is efficient | A continuous subcutaneous infiltration along the ring line is faster than blocking each nerve individually and plugs any anatomical variants |
| Local anesthetic dose limits | For lidocaine with epi: max 7 mg/kg. Total volume for complete scalp block ~20-30 mL of 1% lidocaine with epi. Monitor during the first 10-15 minutes post-injection. |
| Wait time | Allow 10-15 minutes for full onset before beginning the procedure |
| Tumescent supplementation | Most hair transplant surgeons supplement nerve blocks with tumescent local anesthesia (dilute lidocaine + saline + epi) directly into the donor and recipient zones for added hemostasis and hydrodissection |
Contraindications to Scalp Block
- Known allergy to local anesthetics (absolute)
- Absent bone flap (craniectomy defect) - risk of intrathecal spread, especially at occipital injection site (absolute)
- Active local site infection (relative)
- Bleeding disorder/anticoagulation (relative)
Why Nerve Blocks Beat Pure Local Infiltration for Hair Transplant
A ring block or nerve block approach uses far less total anesthetic volume than diffuse local infiltration over the entire scalp, reduces tissue distortion (important for graft placement accuracy), provides more uniform anesthesia, and minimizes systemic LA toxicity risk. The subcutaneous injection also creates a clean tissue plane that aids graft insertion.
Sources: Fitzpatrick's Dermatology Vol.1-2 (p.3731-32) | Roberts & Hedges' Clinical Procedures in Emergency Medicine (p.667-668) | Miller's Anesthesia 10e (p.11044-45) | WFSA Scalp Block: Techniques and Applications (Anaesthesia Tutorial of the Week 480) | Clinista: Scalp Block and Anesthesia in Hair Transplantation
This is a shared conversation. Sign in to Orris to start your own chat.