Dexametgasone supression test
Reading File
Finding Sources
Searching the Web
dexamethasone suppression test types interpretation clinical use
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a thorough answer. Let me compile it.
Dexamethasone Suppression Test (DST)
Background and Rationale
Dexamethasone is a synthetic fluorinated derivative of cortisol with approximately 50-150 times the glucocorticoid activity of cortisol. Its key diagnostic advantage is that immunoassays for cortisol do not cross-react with dexamethasone, so endogenous cortisol can be measured cleanly after its administration.
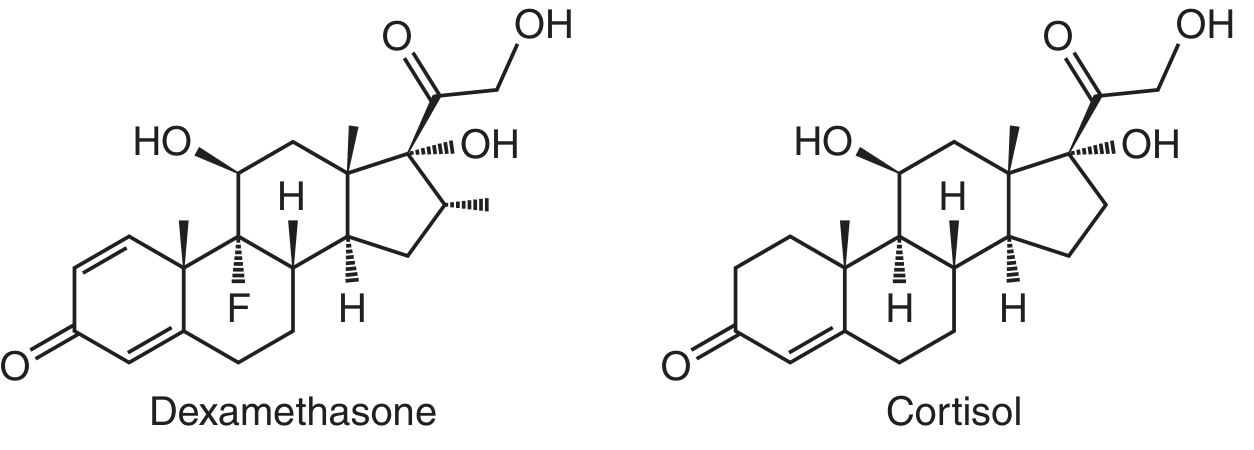
Note the fluorine (F) substituent in dexamethasone that distinguishes it from cortisol.
In a normal HPA axis, exogenous dexamethasone mimics cortisol's negative feedback, suppressing hypothalamic CRH and pituitary ACTH, which in turn reduces adrenal cortisol secretion. In Cushing syndrome, this feedback loop is disrupted - cortisol fails to suppress.
Types of DST
There are three main variants, addressing two clinical questions:
1. Low-Dose DST - "Does the patient have Cushing syndrome?"
A. Overnight (Rapid) Low-Dose DST
| Step | Detail |
|---|---|
| Dose | 1 mg dexamethasone orally at 11 PM (or 0.3 mg/m² in children) |
| Sampling | Plasma cortisol at 8 AM the next morning (8-9 hours later) |
| Normal response | Cortisol < 1.8 µg/dL (50 nmol/L) |
| Abnormal (Cushing) | Cortisol > 1.8 µg/dL |
- Sensitivity: ~95% for Cushing syndrome
- Specificity: ~80% at 1.8 µg/dL threshold; rises to >95% if threshold raised to 5 µg/dL (140 nmol/L)
B. Standard (2-Day) Low-Dose DST
| Step | Detail |
|---|---|
| Dose | 0.5 mg dexamethasone every 6 hours for 48 hours |
| Sampling | Continuous urinary free cortisol and serum cortisol |
| Normal response | Cortisol < 1.8 µg/dL |
2. High-Dose DST - "What is the cause of Cushing syndrome?"
Used after Cushing syndrome is confirmed, to differentiate pituitary (Cushing disease) from ectopic ACTH sources.
| Step | Detail |
|---|---|
| Dose | 2 mg dexamethasone orally every 6 hours for 48 hours (8 mg total/day) |
| OR (overnight) | 8 mg dexamethasone at 11 PM, cortisol at 8 AM |
| Positive suppression | ≥50% reduction in cortisol from baseline |
Interpretation Summary Table
| Condition | Low-Dose DST | High-Dose DST |
|---|---|---|
| Normal | Cortisol suppressed | Cortisol suppressed |
| Pituitary Cushing (Cushing disease) | No suppression | Usually suppressed (pituitary adenoma still responds to higher dose) |
| Ectopic ACTH | No suppression | No suppression (ectopic tumors are autonomous) |
| Adrenal tumor | No suppression | No suppression (ACTH-independent) |
(Table adapted from Scott-Brown's Otorhinolaryngology, Vol. 1)
Important caveat: The high-dose DST is not fully reliable - ~10-20% of ACTH-secreting pituitary adenomas do NOT suppress on high dose, while ~20-50% of ectopic ACTH-producing bronchial carcinoids DO show partial suppression. Additional imaging or inferior petrosal sinus sampling (IPSS) is generally required.
Why the DST is Ordered (Clinical Indications)
- Screening/confirming Cushing syndrome (low-dose)
- Differentiating pituitary vs. ectopic vs. adrenal causes of hypercortisolism (high-dose)
- Evaluating suspected incidentally found adrenal masses (adrenal incidentalomas) for autonomous cortisol secretion
False Positives (Failure to Suppress Without True Cushing)
A post-dexamethasone cortisol > 1.8 µg/dL can be seen in:
- Severe stress, acute/chronic illness, infection
- Obesity
- Severe depression (pseudo-Cushing syndrome)
- Alcohol abuse (alcoholic pseudo-Cushing)
- Oral contraceptives or estrogen therapy (increases cortisol-binding globulin)
- Pregnancy
- Drugs that accelerate dexamethasone metabolism: phenytoin, phenobarbital, rifampin, carbamazepine
- Failure to take the dexamethasone dose
- Renal insufficiency (invalidates the test)
Comparison with Other Cushing Screening Tests
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Overnight 1mg DST | ~95% | ~80% | Best screening test |
| 24-hr urinary free cortisol | ~95% | ~98% | Preferred if estrogens on board |
| Midnight salivary cortisol | ~93% | ~96% | Two samples recommended |
The Endocrine Society recommends using the overnight DST as the third screening option when 24-hr urinary cortisol and midnight salivary cortisol are inconclusive.
After the DST - Next Steps
If the low-dose DST is abnormal (confirms Cushing syndrome), the workup proceeds to determine the source:
- Plasma ACTH level - low/undetectable = adrenal source; elevated = ACTH-dependent
- High-dose DST or CRH stimulation test - differentiate pituitary from ectopic
- If pituitary source likely: MRI pituitary; if MRI negative, consider Bilateral Inferior Petrosal Sinus Sampling (BIPSS) - the gold standard for confirming pituitary vs. ectopic ACTH (petrosal:peripheral ratio >3 post-CRH = pituitary source)
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed. | Quick Compendium of Clinical Pathology, 5th Ed. | Scott-Brown's Otorhinolaryngology, Vol. 1 | Harrison's Principles of Internal Medicine, 22nd Ed.
Approach to Cushing syndrome flowchart
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Finding Sources
Generating Image
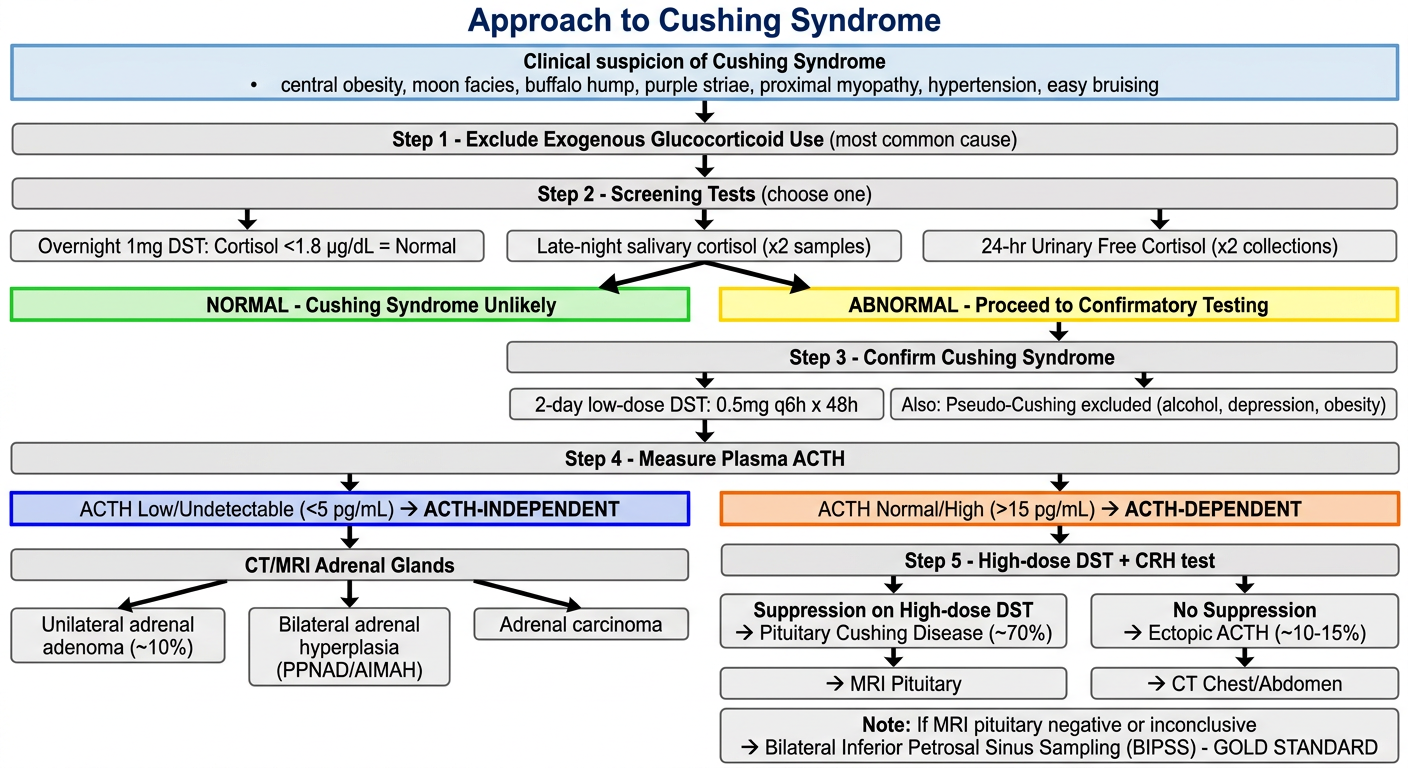
Approach to Cushing Syndrome - Step by Step
Here is the full textbook-based diagnostic algorithm alongside the flowchart:
Step 1 - Clinical Suspicion + Exclude Exogenous Cause
Suggestive features:
- Central obesity, moon facies, dorsocervical fat pad ("buffalo hump")
- Wide (>1 cm) violaceous/purple abdominal striae
- Proximal muscle weakness
- Easy bruising, facial plethora
- Hypertension, glucose intolerance
- Osteoporosis, hypogonadism
First step: Exclude exogenous/iatrogenic glucocorticoid use - this is the most common cause of Cushing syndrome (oral, topical, inhaled, intranasal, injected). A thorough medication and herbal remedy history is essential.
Step 2 - Screening (one of three tests)
| Test | Threshold | Notes |
|---|---|---|
| Overnight 1 mg DST | AM cortisol < 1.8 µg/dL = normal | ~95% sensitive; preferred for adrenal incidentaloma and renal failure |
| Late-night salivary cortisol | Two samples; lab-dependent cutoff | ~93% sensitive; reflects loss of circadian nadir |
| 24-hr urinary free cortisol (UFC) | Two collections; >3-4x ULN significant | Preferred in pregnancy, epilepsy, estrogen use |
Use the 2 mg 48-hr DST preferentially in conditions that activate the HPA axis: depression, morbid obesity, alcoholism, poorly controlled diabetes.
Step 3 - Confirm Cushing Syndrome
If any screening test is abnormal, confirm with:
- 2-day low-dose DST (0.5 mg q6h x 48h) - cortisol fails to suppress
- Exclude pseudo-Cushing states: major depression, chronic alcoholism, morbid obesity (these can give false positives on screening)
Step 4 - Measure Plasma ACTH (Key Branch Point)
This is the central decision step that separates all further workup:
Plasma ACTH
|
├── LOW / Undetectable (<5 pg/mL)
│ → ACTH-INDEPENDENT Cushing syndrome
│ → CT/MRI of adrenal glands
│
└── NORMAL / HIGH (>15 pg/mL)
→ ACTH-DEPENDENT Cushing syndrome
→ Proceed to Step 5
Step 5 - Localize ACTH Source (ACTH-Dependent Only)
| Finding | Likely Diagnosis | Frequency |
|---|---|---|
| High-dose DST suppression + MRI adenoma | Cushing disease (pituitary) | ~70% of endogenous |
| No suppression on high-dose DST | Ectopic ACTH syndrome | ~10-15% |
| Markedly elevated ACTH + rapid onset | Ectopic ACTH (often SCLC) | - |
Tumors causing ectopic ACTH: Small-cell lung carcinoma (~50%), bronchial carcinoid, thymic carcinoid, pancreatic carcinoid, medullary thyroid carcinoma.
Step 6 - Imaging
| Suspected Source | Imaging |
|---|---|
| Pituitary adenoma | MRI pituitary (gadolinium-enhanced) |
| Adrenal adenoma/carcinoma | CT abdomen (adrenal protocol) |
| Ectopic ACTH | CT chest/abdomen |
Caveat: ~50% of patients with Cushing disease have no abnormality on pituitary MRI. Also, ~10% of the general population have incidental pituitary findings that can mislead.
Step 7 - Bilateral Inferior Petrosal Sinus Sampling (BIPSS) - Gold Standard
Indicated when:
- ACTH-dependent Cushing confirmed but pituitary MRI is negative or equivocal
- Need to distinguish pituitary vs. ectopic ACTH with certainty
| Finding | Interpretation |
|---|---|
| IPS:peripheral ACTH ratio >2 (basal) OR >3 (post-CRH) | Cushing disease (pituitary source) |
| IPS:peripheral ratio low | Ectopic ACTH source |
| Asymmetric IPS ratio (left vs. right) | Helps lateralize adenoma within pituitary |
Sensitivity for Cushing disease after CRH stimulation: ~95%
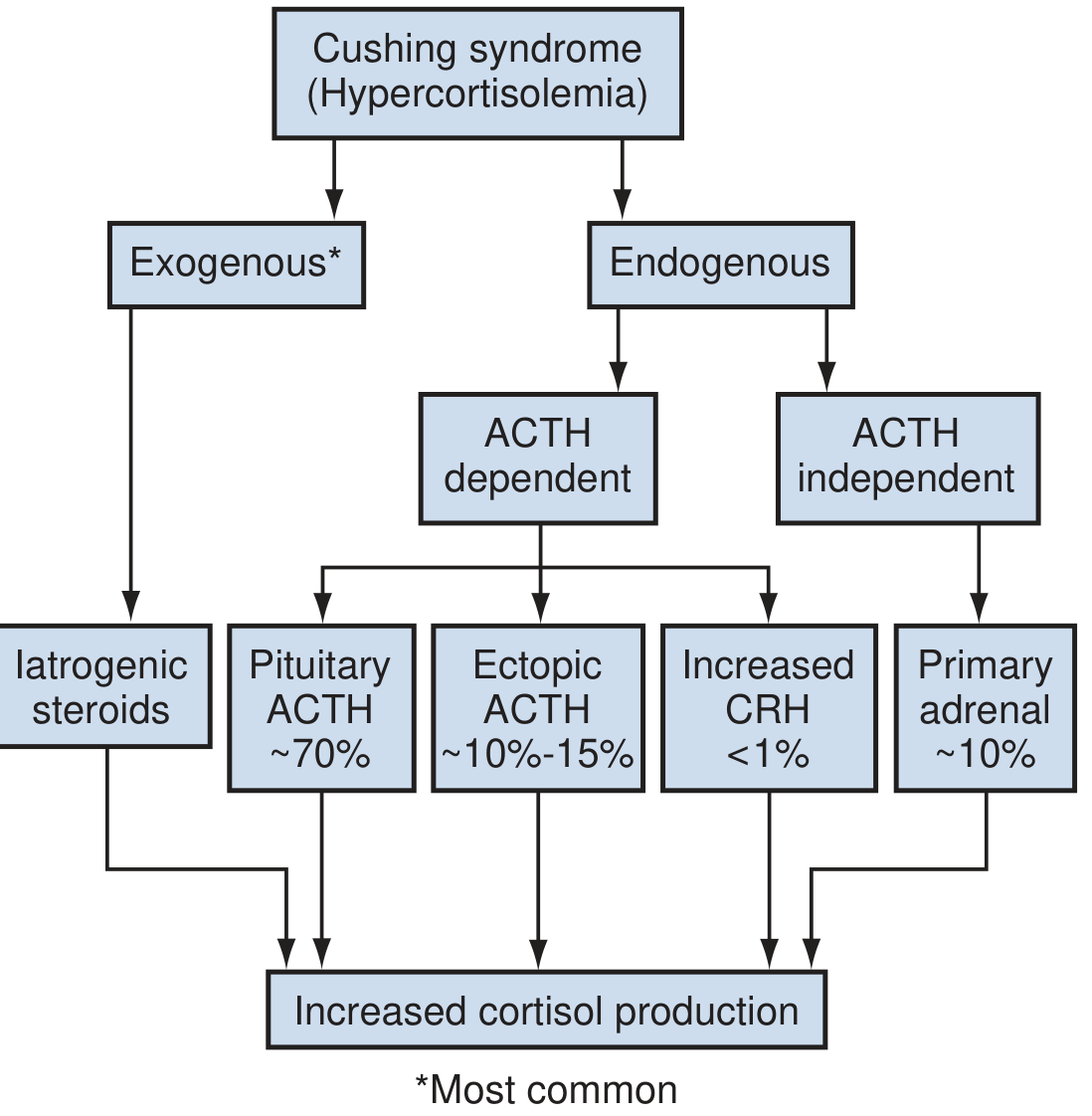
Etiology Classification (from Campbell-Walsh Urology)
Adrenal Incidentaloma - Specific Algorithm
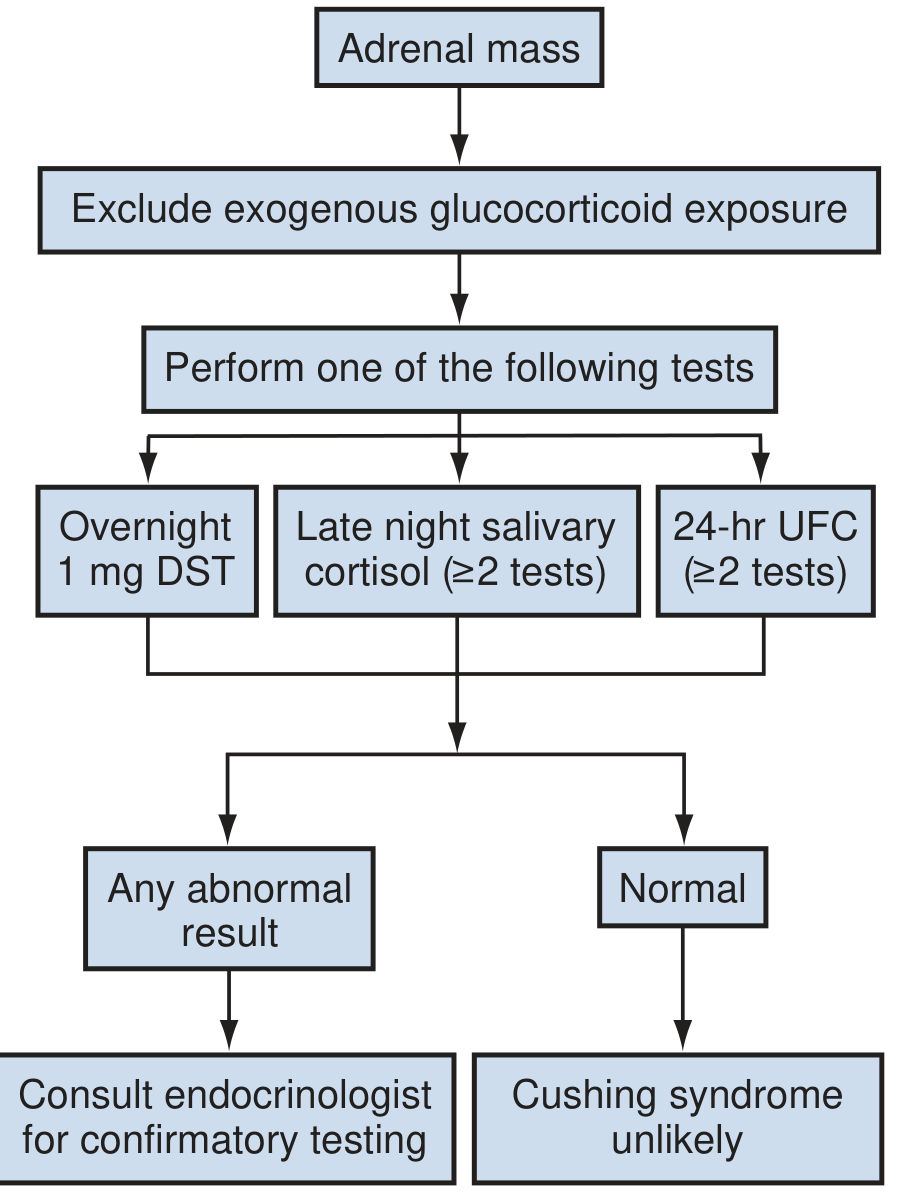
For any adrenal mass: exclude exogenous glucocorticoid use first, then perform one of the three screening tests (overnight DST / late-night salivary cortisol / 24-hr UFC). If any abnormal result - refer to endocrinology for confirmatory testing.
Sources: Campbell-Walsh-Wein Urology, 12th Ed. | Tietz Textbook of Laboratory Medicine, 7th Ed. | Berek & Novak's Gynecology | Quick Compendium of Clinical Pathology, 5th Ed. | Endocrine Society Clinical Practice Guideline (Nieman et al., 2008)
Addison’s disease
Reading File
Finding Sources
Finding Sources
Searching the Web
Addison's disease primary adrenal insufficiency pathophysiology diagnosis treatment 2024
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Addison's Disease (Primary Adrenal Insufficiency)
Definition
Addison's disease is primary adrenocortical insufficiency - failure of the adrenal cortex itself to produce adequate cortisol and aldosterone, with an intact HPA axis (i.e., ACTH is high, not low). Named after Thomas Addison, who described adrenal insufficiency in 1849.
It must be distinguished from:
- Secondary AI - pituitary failure → low ACTH → low cortisol (no mineralocorticoid deficiency, no hyperpigmentation)
- Tertiary AI - hypothalamic failure → low CRH → low ACTH (most often from exogenous steroid withdrawal)
HPA Axis and Types of Adrenal Insufficiency
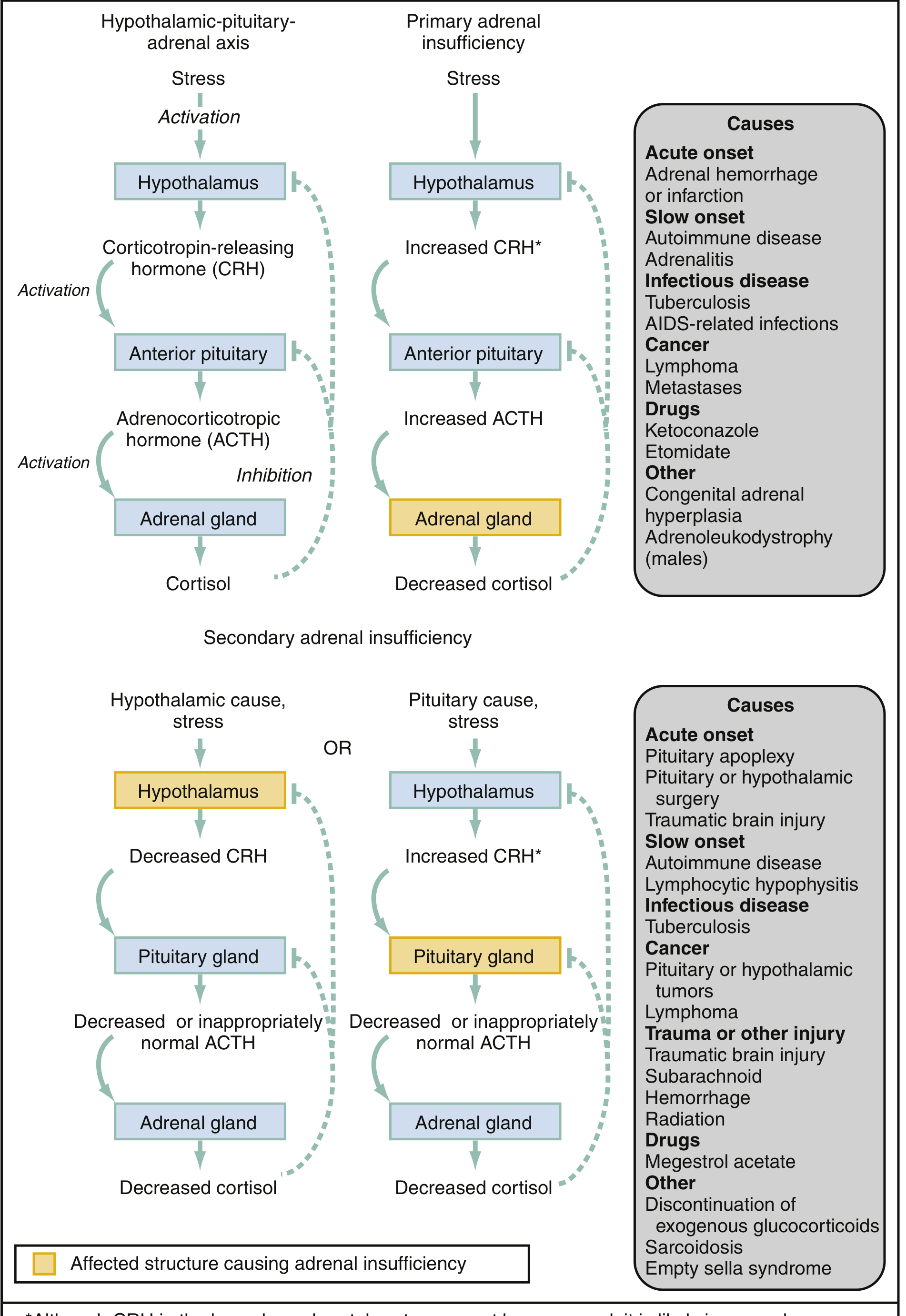
Fig. HPA axis in normal function vs. primary and secondary adrenal insufficiency, showing affected structures (highlighted) and causes. (Rosen's Emergency Medicine)
Epidemiology
- Prevalence: ~1 in 10,000 in developed countries (39-144 per million)
- Most common in ages 30-50 years; female predominance in autoimmune form
- ~90% of cases in developed countries: autoimmune
- Worldwide: tuberculosis remains the leading cause
Etiology
Autoimmune (Most Common in Developed World)
- Autoimmune adrenalitis with 21-hydroxylase antibodies (anti-adrenal antibodies)
- Often part of Autoimmune Polyglandular Syndrome (APS):
- APS type 2 (~70%): Addison + Type 1 DM + autoimmune thyroid disease (autosomal dominant, HLA-DRB1)
- APS type 1 (~10%): Addison + chronic mucocutaneous candidiasis + hypoparathyroidism (autosomal recessive, AIRE gene, chromosome 21q22.3)
- ~10% isolated Addison's (no associated APS)
Infectious
- TB (most common worldwide; adrenal involvement in ~6% of active TB)
- Disseminated fungal infections (histoplasmosis, cryptococcosis, coccidioidomycosis)
- HIV-related infections (CMV, MAI, toxoplasmosis)
Other Causes
| Category | Examples |
|---|---|
| Hemorrhage/infarction (acute) | Waterhouse-Friderichsen syndrome (meningococcemia), anticoagulant therapy, antiphospholipid syndrome, trauma |
| Infiltrative | Metastatic cancer (lung, breast, lymphoma), amyloidosis, hemochromatosis, sarcoid |
| Drugs | Ketoconazole, etomidate, rifampin, fluconazole (inhibit steroidogenesis) |
| Genetic (children) | Congenital adrenal hyperplasia (>80% of pediatric AI), adrenoleukodystrophy |
| Surgical | Bilateral adrenalectomy |
Symptoms appear only after >90% of adrenal tissue is destroyed - explaining the insidious onset.
Pathophysiology
| Deficiency | Consequences |
|---|---|
| Cortisol | Fatigue, weakness, hypoglycemia, anorexia, nausea/vomiting, weight loss, hypotension |
| Aldosterone | Sodium wasting → hyponatremia, hypovolemia, hypotension; potassium retention → hyperkalemia; metabolic acidosis |
| Adrenal androgens (DHEA) | Decreased pubic/axillary hair, decreased libido (especially in women) |
| High ACTH (compensatory) | Hyperpigmentation - ACTH contains the α-MSH fragment → stimulates melanocortin-1 receptor on melanocytes |
Key point: Hyperpigmentation is pathognomonic of primary AI (where ACTH is high). It does NOT occur in secondary AI.
Clinical Features
Chronic Presentation (Insidious Onset)
General (both primary & secondary):
- Fatigue, weakness (most common)
- Anorexia, weight loss
- Nausea, vomiting, diarrhea
- Myalgia, arthralgia
- Depression, apathy
- Mild fever
- Hypotension (BP ≤ 110/70 mmHg)
Primary AI specific:
- Hyperpigmentation - most striking sign
- Sun-exposed areas (face, neck, hands)
- Sites of pressure/friction (knees, elbows, knuckles, spine)
- Palmar creases, nipples, areolae, axillae, genitalia, perineum
- Oral/buccal mucosa (gums, inner cheeks)
- Recent scars
- Salt craving
- Orthostatic hypotension, syncope
- Vitiligo (associated autoimmune depigmentation)
- Hyperkalemia, hyperchloremic metabolic acidosis
- Hypoglycemia
Laboratory Findings
| Lab | Finding | Mechanism |
|---|---|---|
| Serum cortisol | Low | Primary adrenal failure |
| Plasma ACTH | High (>2x upper limit) | Lost negative feedback |
| Serum sodium | Low (hyponatremia) | Aldosterone deficiency + ADH excess |
| Serum potassium | High (hyperkalemia) | Aldosterone deficiency |
| Blood glucose | Low | Cortisol deficiency |
| BUN/Creatinine | Elevated | Prerenal (volume depletion) |
| Serum calcium | May be elevated | |
| Eosinophils | Elevated | Cortisol normally suppresses eosinophils |
| 21-hydroxylase antibodies | Positive | Autoimmune etiology |
| Renin | High | Aldosterone deficiency |
| Aldosterone | Low |
Diagnostic Algorithm
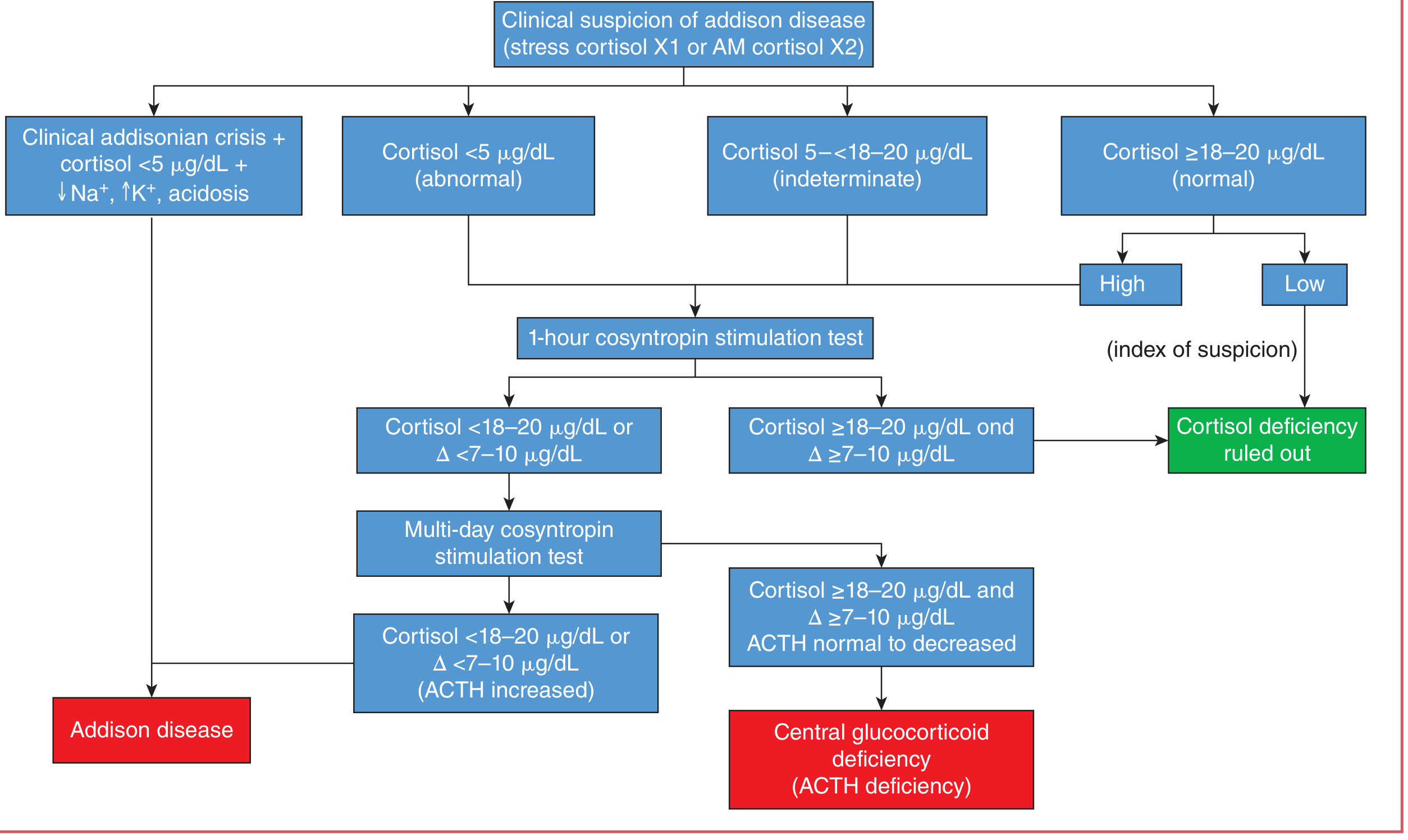
Tietz Textbook of Laboratory Medicine, 7th Ed.
Step-by-Step Diagnostic Approach:
-
Morning plasma cortisol (or stress cortisol x1 / AM cortisol x2):
- < 5 µg/dL → abnormal → proceed to cosyntropin test
- 5-18 µg/dL → indeterminate → proceed to cosyntropin test
- ≥ 18-20 µg/dL → normal (if low suspicion → ruled out)
-
1-hour cosyntropin (ACTH) stimulation test (standard test):
- Give 250 µg synthetic ACTH (cosyntropin) IV/IM
- Measure cortisol at 0, 30, and 60 min
- Normal response: Peak cortisol ≥ 18-20 µg/dL AND Δ ≥ 7-10 µg/dL → rules out cortisol deficiency
- Abnormal response: Cortisol < 18-20 µg/dL or Δ < 7-10 µg/dL → proceed to prolonged test
-
Multi-day cosyntropin stimulation (prolonged protocol):
- Differentiates primary (Addison) from secondary/central AI
- Cortisol fails to rise + ACTH high → Addison disease (primary)
- Cortisol eventually rises + ACTH normal/low → Central glucocorticoid deficiency (secondary/pituitary)
-
Clinical Addisonian crisis (no need to wait for labs):
- Cortisol < 5 µg/dL + ↓Na⁺ + ↑K⁺ + acidosis + shock → Treat immediately
If adrenal crisis is suspected, treat first - test later. Use dexamethasone (not hydrocortisone) if you still want to draw a cortisol level, as dexamethasone does not cross-react with cortisol assays.
Adrenal Crisis (Addisonian Crisis)
Life-threatening emergency. Precipitated by:
- Infection, surgery, trauma, physical/emotional stress
- Abrupt steroid withdrawal in a patient on chronic steroids
- First presentation in previously undiagnosed Addison's
Features: Refractory hypotension/shock, abdominal pain (can mimic acute abdomen), vomiting, confusion, fever
Treatment
Acute Adrenal Crisis
| Drug | Dose |
|---|---|
| Hydrocortisone (first line) | 100 mg IV bolus → then 200 mg/24 hrs (IV bolus q6h or continuous infusion) |
| Dexamethasone (alternative) | 4 mg IV bolus (does not interfere with cortisol assay) |
| IV fluids | Normal saline (aggressive fluid resuscitation) |
| Glucose | Dextrose if hypoglycemic |
Chronic Maintenance Therapy
| Drug | Dose | Purpose |
|---|---|---|
| Hydrocortisone | 15-25 mg/day in 2-3 divided doses (2/3 morning, 1/3 afternoon) | Glucocorticoid replacement |
| Fludrocortisone | 50-100 µg/day | Mineralocorticoid replacement |
| DHEA | 25-50 mg/day | May benefit women (libido, well-being) |
Sick Day Rules ("Stress Dosing")
- Minor illness/fever: Double the daily hydrocortisone dose
- Major illness/surgery/procedural stress: Hydrocortisone 100 mg IV
- Patients should wear a medical alert bracelet and carry an emergency injection kit
Primary vs. Secondary AI - Key Distinctions
| Feature | Primary (Addison's) | Secondary (pituitary) |
|---|---|---|
| ACTH | High | Low or inappropriately normal |
| Hyperpigmentation | Yes | No (pale skin) |
| Aldosterone | Low | Normal |
| Hyperkalemia | Yes | No |
| Hyponatremia | Yes | Yes (different mechanism) |
| Salt craving | Yes | No |
| Mineralocorticoid replacement needed | Yes | No |
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed. | Costanzo Physiology, 7th Ed. | Rosen's Emergency Medicine | Fitzpatrick's Dermatology | Henry's Clinical Diagnosis and Management by Laboratory Methods
Explain Syncathen test in more easy way
The Synacthen test (also called the cosyntropin/ACTH stimulation test) is one of the key tests we just discussed for Addison's disease. Let me explain it in a simple, intuitive way - no library search needed for this one.
The Synacthen Test - Simply Explained
What is Synacthen?
Synacthen is just a synthetic (lab-made) version of ACTH - the hormone your pituitary normally sends to your adrenal glands to tell them "make cortisol!"
Synacthen = Cosyntropin = Synthetic ACTH. Same thing, different names.
The Simple Concept - Think of it as a "Fire Drill"
Imagine your adrenal glands are a fire station, and ACTH is the alarm bell.
Normal situation:
Pituitary rings the alarm (ACTH) → Adrenal glands respond → Cortisol produced ✅
In Addison's disease:
Pituitary rings the alarm (ACTH) → Adrenal glands are DAMAGED → No cortisol ❌
The Synacthen test is essentially ringing the alarm bell artificially and watching if the fire station responds.
- If the adrenal glands respond well → they are healthy → no Addison's
- If they don't respond → they are damaged → Addison's confirmed
How the Test is Done - Step by Step
Step 1: Draw blood → measure baseline cortisol (8 AM fasting)
Step 2: Inject Synacthen 250 µg → IV or IM
(This is the "alarm bell")
Step 3: Wait 30–60 minutes
Step 4: Draw blood again → measure cortisol level
That's it. Simple 3-blood-draw test done in under an hour.
How to Read the Result
Think of it like a car engine test: you press the accelerator (Synacthen), and check if the engine revs up (cortisol rises).
| Result | Cortisol after Synacthen | Meaning |
|---|---|---|
| ✅ Normal | Rises to ≥ 18-20 µg/dL AND goes up by ≥ 7-10 µg/dL | Adrenal glands are healthy |
| ❌ Abnormal | Stays < 18-20 µg/dL or barely rises | Adrenal glands are not working |
But Wait - What If the Test is Abnormal? WHO is to Blame?
This is the clever part. An abnormal result just tells you the adrenals aren't making cortisol - but it doesn't tell you why. You now need to figure out:
Is it the ADRENAL GLAND'S fault? → Primary AI (Addison's disease)
OR
Is it the PITUITARY'S fault? → Secondary AI
Think of it this way:
- Addison's = The fire station itself is burnt down. Even if you ring the alarm (Synacthen), no trucks come out.
- Secondary AI = The fire station is fine, but it hasn't been used in so long (low ACTH from pituitary) that it has gone "rusty/lazy."
How to tell them apart after a failed test:
Short test (250 µg) = good for PRIMARY AI (Addison's)
The adrenal glands are so destroyed they can't respond at all.
Prolonged/multi-day test = needed for SECONDARY AI
Give low-dose Synacthen (1 µg) over several days - a lazy (atrophied) adrenal gland will eventually "wake up" if stimulated enough. A truly destroyed one (Addison's) never will.
| Addison's (Primary) | Secondary (Pituitary) | |
|---|---|---|
| Short Synacthen test | ❌ Fails | ❌ May also fail initially |
| Prolonged Synacthen test | ❌ Still fails | ✅ Eventually responds |
| ACTH level | 🔴 Very HIGH | 🔵 Low or normal |
Why Check ACTH Alongside?
After the Synacthen test fails, measure plasma ACTH:
ACTH very HIGH → Pituitary is screaming for help but adrenals can't respond
→ ADDISON'S DISEASE ✅
ACTH low/normal → Pituitary is not sending the signal properly
→ SECONDARY (pituitary) AI ✅
This single measurement separates the two conditions definitively.
The Whole Picture in One Diagram
INJECT SYNACTHEN (250 µg)
|
┌────────────┴────────────┐
↓ ↓
Cortisol RISES Cortisol STAYS LOW
(≥18-20 µg/dL) (<18-20 µg/dL)
↓ ↓
NORMAL ✅ ADRENAL INSUFFICIENCY
↓
Check ACTH level
┌──────────┴──────────┐
↓ ↓
ACTH HIGH ACTH LOW/Normal
↓ ↓
ADDISON'S SECONDARY AI
(adrenal (pituitary/
damage) steroid use)
When Should You NOT Do This Test?
- Active adrenal crisis → Don't wait for the test, treat immediately with hydrocortisone 100 mg IV
- If you're suspicious of crisis but still want to test → use dexamethasone instead of hydrocortisone for treatment, since dex doesn't interfere with the cortisol assay
One-Line Summary
The Synacthen test = Give fake ACTH, measure if adrenals respond. No response = adrenal insufficiency. Then check ACTH level to find out whose fault it is.
Approach to addisons disease like previous one
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Generating Image
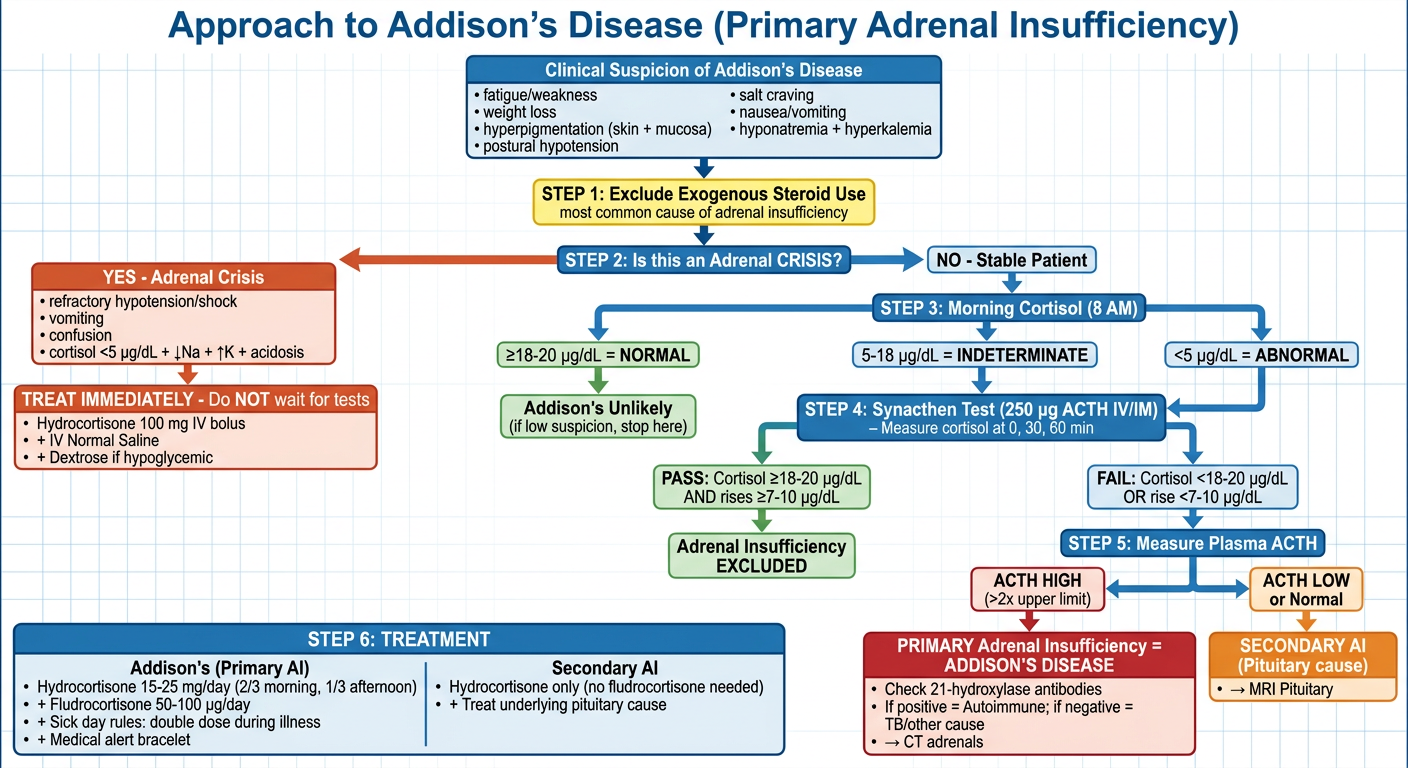
Here's the full written walkthrough to go alongside the flowchart:
Step-by-Step Approach to Addison's Disease
Step 1 - Clinical Suspicion
Think of Addison's when a patient has a combination of:
| Symptom/Sign | Why it happens |
|---|---|
| Fatigue, weakness | No cortisol = no energy metabolism |
| Hyperpigmentation (skin + mouth) | High ACTH stimulates melanocytes |
| Postural hypotension | No aldosterone = salt/water loss |
| Salt craving | Body trying to compensate sodium loss |
| Nausea, weight loss | Cortisol deficiency |
| Hyponatremia + Hyperkalemia | Hallmark electrolyte pattern |
Step 2 - Is it a Crisis?
First question always: Is this patient in shock?
-
YES (crisis): Cortisol < 5 µg/dL + ↓Na + ↑K + refractory hypotension → Treat first, test later
- Hydrocortisone 100 mg IV bolus
- Aggressive IV Normal Saline
- Dextrose if hypoglycaemic
- Identify & treat the precipitant (infection, surgery, missed doses)
-
NO (stable): Proceed with investigation
Step 3 - Morning Cortisol (8 AM)
| Value | Interpretation | Next step |
|---|---|---|
| ≥ 18-20 µg/dL | Normal | Addison's unlikely (stop if low suspicion) |
| 5-18 µg/dL | Indeterminate | Do Synacthen test |
| < 5 µg/dL | Abnormal | Do Synacthen test |
Step 4 - Synacthen (Cosyntropin) Test
Give 250 µg Synacthen IV or IM. Measure cortisol at 0, 30, 60 min.
- PASS (Cortisol ≥ 18-20 µg/dL AND rises by ≥ 7-10 µg/dL) → Adrenal insufficiency excluded ✅
- FAIL (Cortisol stays low, barely rises) → Adrenal insufficiency confirmed → Go to Step 5
Step 5 - Measure Plasma ACTH (The Key Branch Point)
ACTH very HIGH → Adrenal gland is damaged
→ PRIMARY AI = ADDISON'S DISEASE
ACTH LOW/Normal → Pituitary not sending the signal
→ SECONDARY AI (not Addison's)
Step 6 - Find the Cause of Addison's
Once primary AI confirmed:
- 21-hydroxylase antibodies positive → Autoimmune Addison's (most common in developed world)
- Antibodies negative → Look for other cause:
- CT adrenals: calcification = TB; bilateral enlargement = metastases/lymphoma; bilateral haemorrhage
- VLFCA levels (for adrenoleukodystrophy in young males)
- Screen for APS (thyroid, diabetes, parathyroid)
Step 7 - Treatment
| Addison's (Primary AI) | Secondary AI | |
|---|---|---|
| Glucocorticoid | Hydrocortisone 15-25 mg/day (2/3 AM, 1/3 afternoon) | Hydrocortisone (same dosing) |
| Mineralocorticoid | Fludrocortisone 50-100 µg/day ✅ | Not needed (aldosterone normal) |
| Sick day rules | Double dose during minor illness | Same |
| Crisis prevention | Medical alert bracelet + emergency injection kit | Same |
| DHEA | Consider in women (libido, well-being) | - |
The One Key Difference to Always Remember
| Feature | Addison's (Primary) | Secondary (Pituitary) |
|---|---|---|
| ACTH | 🔴 HIGH | 🔵 Low |
| Hyperpigmentation | YES | No |
| Aldosterone | LOW | Normal |
| Fludrocortisone needed | YES | No |
| Hyperkalemia | YES | No |
Sources: Tietz Textbook of Laboratory Medicine, 7th Ed. | Rosen's Emergency Medicine | Goldman-Cecil Medicine | Current Surgical Therapy, 14th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.