development of placenta for MBBS ist prof exam
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the information needed for a complete, exam-ready answer. Let me compile a thorough, well-structured response.
Development of the Placenta
Source: The Developing Human: Clinically Oriented Embryology (Moore, Persaud & Torchia)
Overview
The placenta is a fetomaternal organ with two components:
- Fetal part - derived from the chorionic sac (villous chorion / chorion frondosum)
- Maternal part - derived from the decidua basalis (endometrium)
It functions as a transport system for nutrients, oxygen, and waste between mother and embryo/fetus. Its activities include: protection, nutrition, respiration, excretion, and hormone production.
The Decidua (Maternal Component)
The decidua is the endometrium of the pregnant uterus - specifically, its functional layer that separates after parturition.
Three regions, named by their relation to the implantation site:
| Region | Location | Role |
|---|---|---|
| Decidua basalis | Deep to the conceptus | Forms the maternal part of the placenta |
| Decidua capsularis | Overlying (superficial to) the conceptus | Disappears by ~22 weeks |
| Decidua parietalis | All remaining endometrium | Fuses with smooth chorion later |
The decidual reaction: Connective tissue cells enlarge, accumulate glycogen and lipid, forming decidual cells. This is driven by rising progesterone levels.
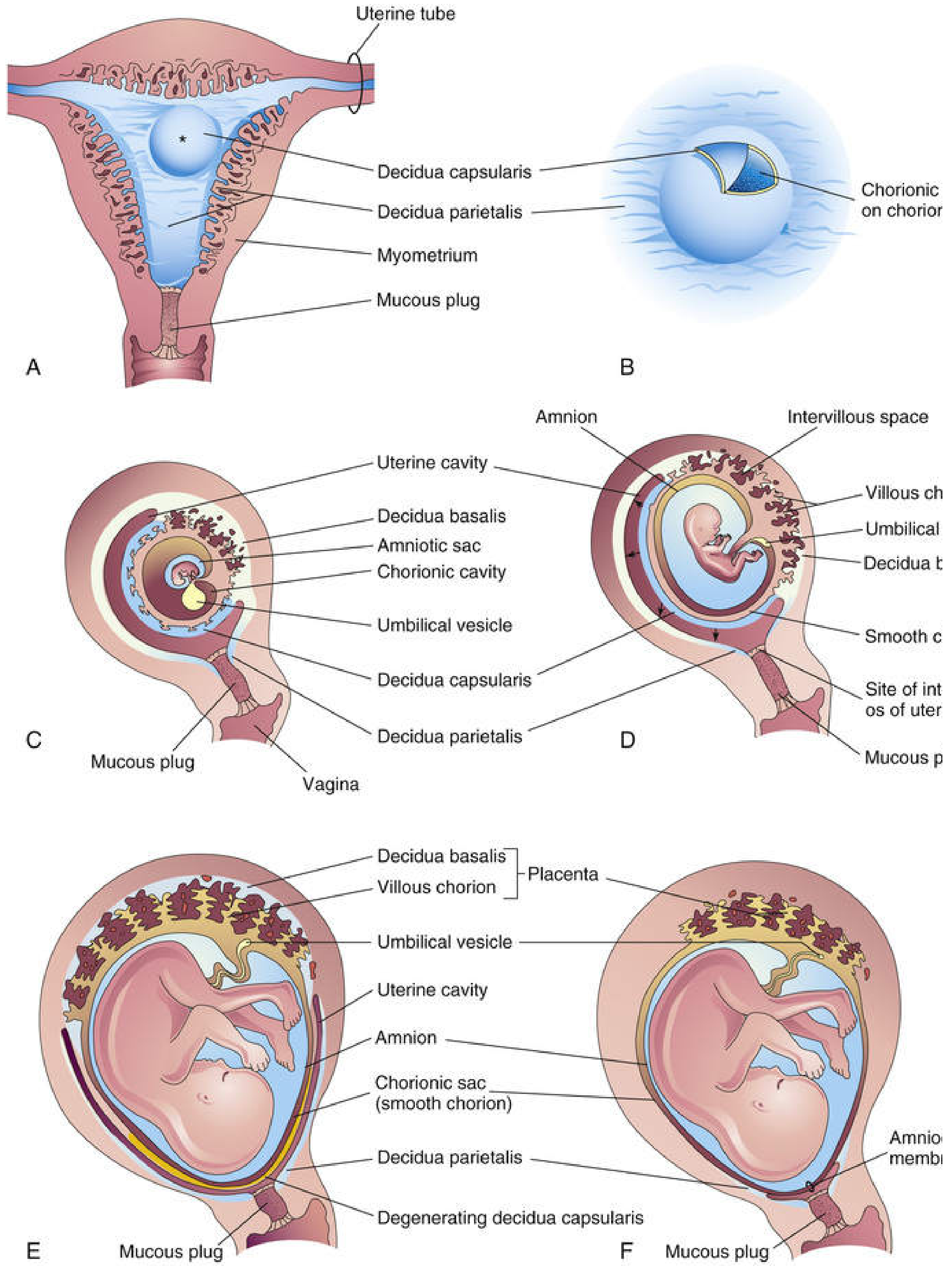
Development of the Chorionic Villi
Week 2: Lacunae form in the syncytiotrophoblast - these are the precursors of the intervillous space.
Week 3: Primary chorionic villi (syncytiotrophoblast + cytotrophoblast core) become secondary villi when mesenchyme invades the core; then tertiary villi when blood vessels develop in the mesenchyme. By the end of week 3, the vascular network is established and physiological exchange is possible.
Up to Week 8: Chorionic villi cover the entire chorionic sac.
After Week 8:
- Villi associated with decidua capsularis lose blood supply, compress, and degenerate → form the smooth, bare chorion laeve (smooth chorion)
- Villi associated with decidua basalis proliferate, branch profusely, and enlarge → form the chorion frondosum (villous chorion) - this is the fetal part of the placenta
This transformation is driven by homeobox genes (HLX, MSX2, DLX3) expressed in the trophoblast.
Structure of the Mature Placenta
Shape and Size
- Discoid shape (circular, due to the shape of the persistent villous area)
- At term: covers 15-30% of the decidua; weighs ~1/6 of the fetus
- Growth continues until fetus is ~18 weeks old
The Cytotrophoblastic Shell
The fetal part is attached to the maternal part by the cytotrophoblastic shell - an external layer of trophoblastic cells on the maternal surface. It anchors the chorionic sac to the decidua basalis. Endometrial arteries and veins pass through gaps in this shell.
Cotyledons and Placental Septa
As chorionic villi invade the decidua basalis, decidual tissue is eroded to enlarge the intervillous space. This erosion produces wedge-shaped projections of decidua called placental septa, which project toward the chorionic plate and divide the fetal part into irregular convex areas: the cotyledons.
- Each cotyledon = 2 or more stem villi + many branch villi
- By the end of the 4th month, the decidua basalis is almost entirely replaced by cotyledons (~15-30 cotyledons total)
- Septa do NOT reach the chorionic plate, so there is free communication between cotyledons
The branching of stem villi is regulated by kinase genes MAP2K1 and MAP2K2 and transcription factor Gcm1 (glial cells missing-1).
Placental Circulation
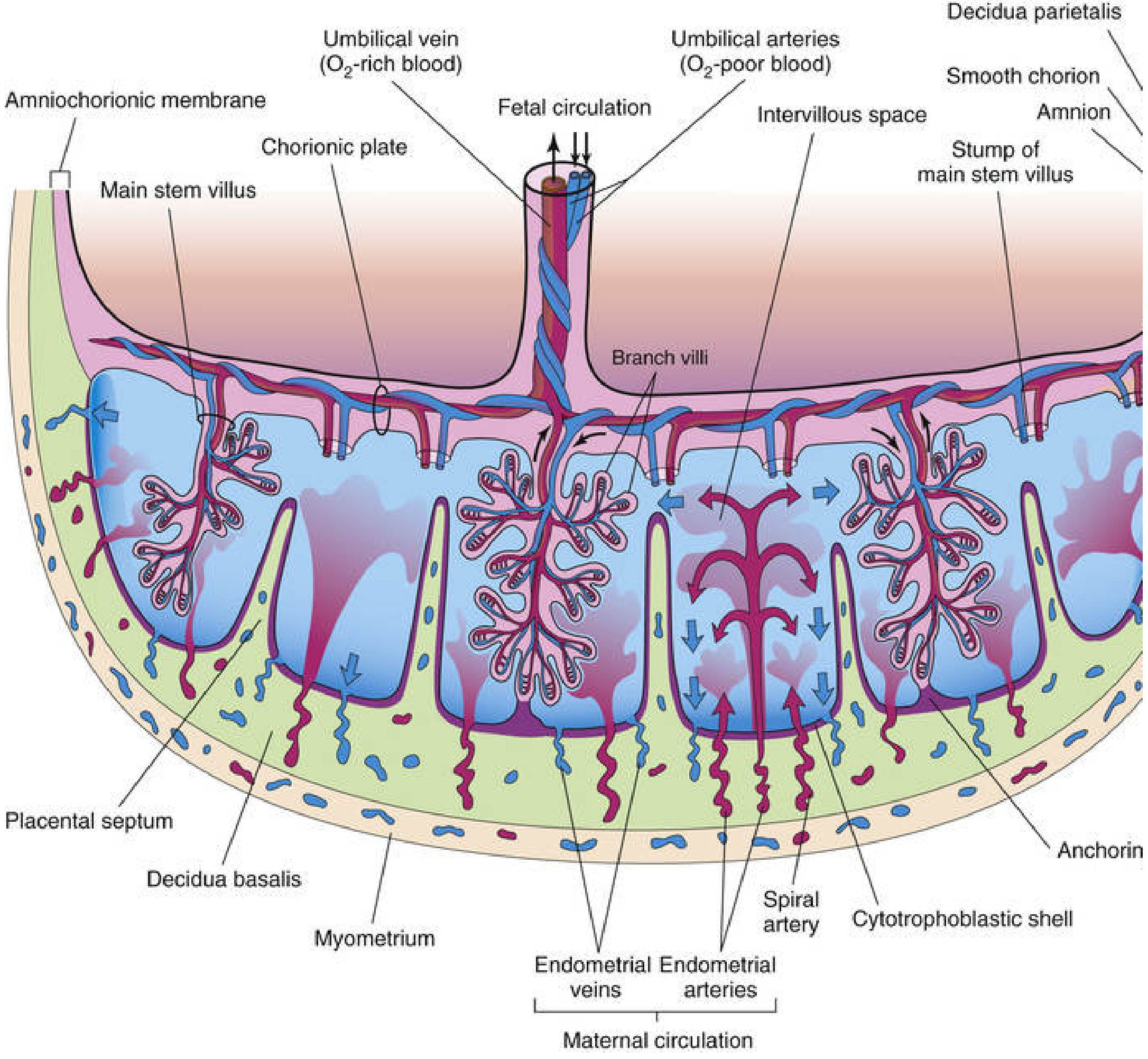
Fetal Placental Circulation
- Umbilical arteries (2) carry deoxygenated blood from fetus to placenta
- At the umbilical cord insertion, they branch into chorionic arteries on the chorionic plate
- These branch into the arteriocapillary-venous system within chorionic villi
- After gas/nutrient exchange, oxygenated blood returns via veins → converge to form the single umbilical vein
- The umbilical vein carries oxygen-rich blood back to the fetus
Maternal Placental Circulation
- 80-100 spiral endometrial arteries in the decidua basalis discharge blood into the intervillous space through gaps in the cytotrophoblastic shell
- Blood spurts toward the chorionic plate (the "roof"), then flows slowly over branch villi → exchange occurs
- Blood drains via endometrial veins back to maternal circulation
- The intervillous space at term contains ~150 mL of blood, replenished 3-4 times per minute
Key principle: Fetal and maternal blood do NOT normally mix. They are separated by the placental membrane.
Early trophoblastic plugging (weeks 1-11): Trophoblastic cells initially plug spiral arteries, allowing only plasma into the intervillous space (maintaining a low-O₂ environment needed for early development). Plugs break down at 11-14 weeks, allowing whole blood flow.
Placental Membrane (Placental Barrier)
The placental membrane is a composite of extrafetal tissues separating maternal and fetal blood.
Before ~20 weeks (4 layers):
- Syncytiotrophoblast (outermost)
- Cytotrophoblast (layer of cells)
- Connective tissue (mesenchyme of villus)
- Fetal capillary endothelium (innermost)
After ~20 weeks (2-3 layers remain):
- The cytotrophoblast cells thin out and nearly disappear
- The membrane becomes very thin, greatly increasing efficiency of exchange
- At term: essentially just syncytiotrophoblast + fetal endothelium
Note: The term "placental barrier" is a misnomer - it is selective, not absolute. Many substances (drugs, viruses, antibodies) can cross it.
Hofbauer cells - fetal macrophages present in chorionic villi throughout pregnancy; involved in placental development and defense.
Functions of the Placenta
1. Respiration
- O₂ and CO₂ cross by simple diffusion
- Fetal hypoxia results from reduced uterine blood flow (not diffusion limitation)
2. Nutrition / Transfer of Substances
| Substance | Mechanism |
|---|---|
| Water | Simple diffusion |
| Glucose | Facilitated diffusion (via GLUT-1 transporter) |
| Amino acids | Active transport |
| Free fatty acids | Simple diffusion |
| Large proteins (e.g., IgG) | Pinocytosis |
| O₂, CO₂, CO | Simple diffusion |
| Electrolytes (Na⁺, K⁺) | Active transport |
3. Excretion
- Fetal waste products (urea, uric acid, creatinine, bilirubin) pass to maternal blood
4. Metabolism
- Synthesizes glycogen, cholesterol, fatty acids in early pregnancy
- Serves as energy/nutrient source for the embryo
5. Endocrine Secretion (Hormones)
| Hormone | Function |
|---|---|
| hCG (human chorionic gonadotropin) | Maintains corpus luteum; basis of pregnancy test; peaks at ~8-10 weeks |
| hPL (human placental lactogen) | Promotes fetal growth; mammary gland development; anti-insulin effect |
| Progesterone | Maintains pregnancy; produced from 10-12 weeks onward (after corpus luteum declines) |
| Estrogens (mainly estriol) | Uterine growth; mammary gland development |
| Relaxin | Relaxes pubic symphysis and uterine myometrium |
6. Immunological Functions
- Transfers maternal IgG antibodies to fetus (passive immunity) - by pinocytosis
- Acts as an allograft (semi-foreign tissue) - the placenta expresses non-classical HLA molecules (HLA-G, HLA-E) that prevent maternal immune rejection
Clinically Important Points (Exam Focus)
| Condition | Mechanism |
|---|---|
| Placenta previa | Implantation over the internal os; causes painless antepartum hemorrhage |
| IUGR | Reduced uteroplacental circulation → fetal hypoxia and growth restriction |
| Preterm labor | Premature rupture of amniochorionic membrane (<37 weeks) |
| Hydatidiform mole | Abnormal trophoblastic proliferation; elevated hCG |
| Transplacental infections | TORCH organisms (Toxoplasma, Rubella, CMV, Herpes) cross the membrane |
| Rh incompatibility | Minute fetal RBCs enter maternal circulation at delivery → maternal sensitization |
| Drug transfer | Most drugs cross by diffusion - thalidomide, alcohol, cocaine are teratogens |
Summary Table: Key Timelines
| Time | Key Event |
|---|---|
| Week 2 | Lacunae form in syncytiotrophoblast |
| Week 3 | Tertiary villi with blood vessels; vascular exchange begins |
| Week 4 | Complex vascular network established |
| Week 8 | Smooth chorion (chorion laeve) begins forming; villous chorion (chorion frondosum) develops |
| Weeks 11-14 | Trophoblastic plugs break down; maternal blood flow into IVS |
| Week 16-18 | Rapid placental growth; decidua basalis replaced by cotyledons |
| Week 20 | Cytotrophoblast thins; placental membrane now 2-3 layers |
| Week 36-40 | Full-term placenta: discoid, ~500g, ~15-30 cotyledons |
- The Developing Human: Clinically Oriented Embryology, Chapter 7 (Moore, Persaud & Torchia)
Create a summary presentation on placenta for quick revision
Reading File
Reading File
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your presentation is ready! Here is your download link:
Placenta Revision
Presentation · PPTX
The deck has 12 slides covering everything you need for a 1st Prof exam revision:
| Slide | Content |
|---|---|
| 1 | Title slide |
| 2 | What is the Placenta? (overview, functions) |
| 3 | The Decidua — 3 regions + decidual reaction |
| 4 | Development of chorionic villi — visual timeline (Wk 2 → Term) |
| 5 | Mature placenta structure — cotyledons, septa, cytotrophoblastic shell + Moore's diagram |
| 6 | Placental circulation — fetal + maternal (dark theme, color-coded) |
| 7 | Placental membrane / "barrier" — 4 layers vs 2-3 layers + Hofbauer cells |
| 8 | Transport mechanisms — diffusion, active, pinocytosis + TORCH/drugs table |
| 9 | Placental hormones — hCG, hPL, Progesterone, Estrogens, Relaxin |
| 10 | Clinical correlates — Previa, IUGR, Preterm, Mole, Rh incompatibility, TORCH |
| 11 | Key timelines table (Wk 2 → Term) |
| 12 | Exam summary — all 8 key takeaways at a glance |
The design uses a navy/teal/rose palette with the actual Moore's Embryology diagram of the full-term placenta cross-section embedded on slide 5.
This is a shared conversation. Sign in to Orris to start your own chat.