Leishmaniasis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"leishmaniasis"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Excellent content. I now have comprehensive information. Let me compile the full answer:
Leishmaniasis
Leishmaniasis is a chronic inflammatory disease caused by obligate intracellular protozoan parasites of the genus Leishmania, transmitted through the bite of infected female phlebotomine sandflies. It ranges in severity from a single self-healing skin lesion to a fatal systemic illness.
Etiology and Life Cycle
The parasite exists in two forms:
- Promastigote - extracellular, flagellated form in the sandfly gut. When the fly bites, promastigotes are injected into the host dermis along with vasodilatory sandfly saliva (e.g., maxadilan) which potentiates infection.
- Amastigote - intracellular, non-flagellated form within the phagolysosomal compartment of host macrophages. Amastigotes contain a unique organelle - the kinetoplast (a mass of mitochondrial DNA), making these parasites kinetoplastids.
Promastigotes are phagocytosed by macrophages; the phagolysosome's acidity (normally pH 4.5) would be lethal, but the parasites maintain the pH at 6.5 to survive. They then transform into amastigotes, which proliferate and spread to infect additional macrophages. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Main Species and Clinical Forms
| Leishmania spp. | Subgenus | Distribution | Primary Disease | Alternative Name |
|---|---|---|---|---|
| L. donovani | Leishmania | South Asia, East Africa | Visceral | Kala-azar |
| L. infantum (chagasi) | Leishmania | Europe, Mediterranean, S. America | Visceral | - |
| L. major | Leishmania | Asia, N. Africa, Middle East | Cutaneous | Biskra nail |
| L. tropica | Leishmania | Asia, Europe | Cutaneous | Aleppo boil |
| L. aethiopica | Leishmania | Ethiopia | Cutaneous/Diffuse | - |
| L. mexicana | Leishmania | Central America | Cutaneous | Chiclero ulcer |
| L. braziliensis | Viannia | South America | Cutaneous/Mucosal | ML-Espundia |
| L. amazonensis | Leishmania | S. & Central America | Cutaneous/Diffuse | - |
- Goldman-Cecil Medicine, Table 319-1
Clinical Forms
1. Visceral Leishmaniasis (Kala-azar)
The most serious form - fatal in >95% of cases if untreated. Caused mainly by L. donovani and L. infantum.
Clinical features:
- Irregular bouts of fever (often twice-daily "double quotidian" spikes)
- Massive hepatosplenomegaly (spleen can weigh up to 3 kg)
- Progressive weight loss, weakness
- Pancytopenia (bone marrow invasion)
- Lymphadenopathy
- Hyperpigmentation of skin in South Asians - the origin of "kala-azar" (black fever in Hindi)
- Hypoalbuminemia and edema
Microscopically, the spleen is packed with enlarged macrophages stuffed with amastigotes; normal splenic architecture is obliterated. The liver shows Kupffer cell infiltration and late fibrosis. There may also be an immune complex-mediated mesangioproliferative glomerulonephritis and, in advanced disease, amyloid deposition in the kidneys. - Robbins & Cotran
Post-kala-azar dermal leishmaniasis (PKDL): A rare sequela appearing 1-5 years after cure of VL (South Asian form) or concurrently (Sudanese/East African form). Characterized by dermal nodules or maculopapular rash.
Estimated global burden: 50,000-90,000 new cases/year; most in Brazil, East Africa, and South-East Asia. - Park's Textbook of Preventive & Social Medicine
2. Cutaneous Leishmaniasis (CL)
The most common form (600,000 to 1 million cases/year). Caused by L. major, L. tropica, L. mexicana, L. braziliensis, and others.
- Lesion begins as a papule surrounded by induration, which evolves into a shallow, slowly expanding ulcer on exposed skin
- Leaves permanent scars
- Generally self-limiting but may persist for months to years
- Predominantly in the Americas, Mediterranean, Middle East, Central Asia
3. Mucocutaneous Leishmaniasis (MCL / Espundia)
Mainly caused by L. braziliensis.
- Moist, ulcerating lesions in the nasopharyngeal region
- Leads to partial or total destruction of the mucous membranes of the nose, mouth, and throat - highly destructive and disfiguring
- May reactivate after long intervals of apparent cure
-
90% of cases in Bolivia, Brazil, Ethiopia, and Peru
4. Diffuse Cutaneous Leishmaniasis (DCL)
- Rare form; caused by L. aethiopica and L. amazonensis
- Begins as a single skin nodule that spreads until the entire body surface is covered with nodular lesions
- Microscopically: foamy macrophages stuffed with organisms
- Associated with severe immunologic anergy to leishmanial antigens (dominant Th2 response)
Histopathology
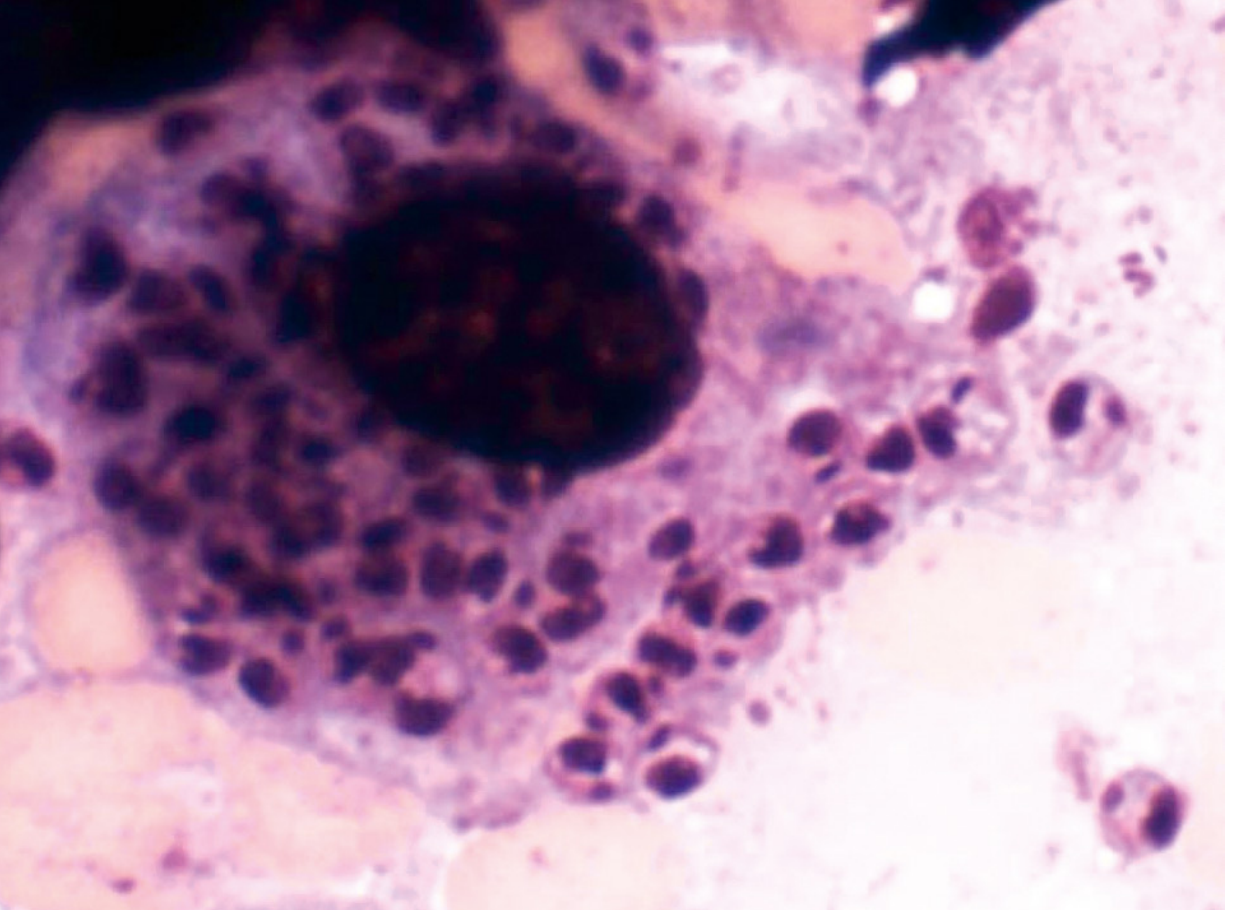
Fig: Giemsa stain of a tissue macrophage with L. donovani amastigotes (dark oval bodies with visible kinetoplast). - Robbins, Cotran & Kumar
Pathogenesis and Immune Response
The outcome of infection depends critically on the Th1 vs Th2 immune response:
| Response | Outcome |
|---|---|
| Th1 dominant (IFN-γ, IL-12, TNF-α) | Classical macrophage (M1) activation → intracellular killing via nitric oxide and ROS → parasite clearance |
| Th2 dominant (IL-4, IL-10, IL-13, TGF-β) | Alternative macrophage (M2) activation → parasite survival and spread |
Key virulence mechanisms of Leishmania:
-
Lipophosphoglycan (LPG) on promastigote surface resists complement
-
Gp63 (zinc-dependent proteinase) cleaves host enzymes
-
Maintains phagolysosome pH at 6.5 (instead of normal 4.5) to survive intracellularly
-
Produces endonucleases that digest neutrophil extracellular traps (NETs)
-
Uses microRNAs to disrupt host cellular signaling
-
Stimulates iron entry into phagolysosomes via ZIP family transporters
-
Robbins, Cotran & Kumar; Goldman-Cecil Medicine
Diagnosis
- Definitive: Demonstration of amastigotes on Giemsa-stained tissue smears/biopsy (spleen, bone marrow, lymph nodes for VL; skin/mucosa for CL)
- Culture: On NNN (Novy-MacNeal-Nicolle) medium
- PCR: Sensitive and specific; useful for species identification
- Serology: rK39 rapid antigen test (widely used for VL in South Asia)
- Montenegro skin test (leishmanin test): Delayed-type hypersensitivity test - negative in active VL; positive in healed or CL
Treatment
The choice of agent depends on species, geographic region (resistance patterns), and host factors.
Visceral Leishmaniasis
| Drug | Class | Route | Notes |
|---|---|---|---|
| Liposomal Amphotericin B | Polyene antifungal | IV | Drug of choice in most regions; single-dose regimens used in India |
| Amphotericin B deoxycholate | Polyene | IV | Effective but more toxic than liposomal form |
| Miltefosine | Alkylphosphocholine | Oral | First oral drug for VL; interferes with phospholipids and induces apoptosis; teratogenic - avoid in pregnancy; nausea/vomiting common |
| Sodium stibogluconate | Pentavalent antimonial | IV/IM | Prodrug reduced to active trivalent form; resistance emerging in India; cardiac arrhythmias, pancreatitis, elevated LFTs |
| Meglumine antimoniate | Pentavalent antimonial | IV/IM | Similar to stibogluconate |
| Pentamidine | Diamidine | IM | Alternative agent |
| Paromomycin | Aminoglycoside | IM | Alternative; often used in combination |
Cutaneous Leishmaniasis
- Many cases are self-limiting and may not require systemic treatment
- First-line systemic: Miltefosine 50 mg BID (if weight 30+ kg)
- Parenteral: sodium stibogluconate, meglumine antimoniate, amphotericin B
- Others: fluconazole, paromomycin
Mucocutaneous Leishmaniasis
-
Less responsive to treatment; relapses common
-
Options: liposomal amphotericin B, miltefosine, sodium stibogluconate, meglumine antimoniate, amphotericin B deoxycholate
-
Lippincott Illustrated Reviews Pharmacology; Goldman-Cecil Medicine; Katzung's Basic & Clinical Pharmacology
Epidemiology and Control
-
Endemic in tropical and subtropical regions of 98 countries
-
Worsening factors: asymptomatic carriers, PKDL, undernutrition, HIV co-infection (Leishmania-HIV co-infection greatly worsens prognosis)
-
Zoonotic reservoirs: rodents, canids (dogs/foxes) - most forms are zoonoses; Indian kala-azar is the major exception (anthroponotic)
-
Prevention: Insecticide-treated bed nets, sandfly control, reservoir host elimination, personal protection (repellents, protective clothing)
-
Epidemics occur with forced migration of non-immune populations into endemic areas (poverty-driven disease)
-
Park's Textbook of Preventive & Social Medicine; Robbins, Cotran & Kumar
Summary of key facts for exams:
- Vector: female phlebotomine sandfly
- Intracellular form in humans: amastigote (diagnostic form)
- Extracellular form in sandfly: promastigote
- Pathognomonic feature: kinetoplast (unique mitochondrial DNA organelle)
- Most fatal form: visceral (kala-azar) - fatal if untreated
- Most common form: cutaneous
- Only oral drug: miltefosine (teratogenic!)
- Drug of choice (VL): liposomal amphotericin B
- Th1 response = protection; Th2 response = susceptibility
This is a shared conversation. Sign in to Orris to start your own chat.