Hepatic encephalopathy
Reading File
Finding Sources
Searching PubMed
"hepatic encephalopathy"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive answer.
Hepatic Encephalopathy (HE)
Hepatic encephalopathy is a clinical state of altered cerebral function resulting from the diseased liver's failure to perform its normal metabolic functions. It encompasses a wide array of transient, reversible neurologic and psychiatric manifestations found predominantly in patients with chronic liver disease and portal hypertension, but also in acute liver failure (ALF).
Definition and Epidemiology
- HE develops in 50-70% of patients with cirrhosis
- Poor prognosis: 1-year survival 42%, 3-year survival 23% without liver transplantation
- Minimal HE - the mildest form - affects about half of all cirrhotic patients but is commonly overlooked
- Approximately 20,000 patients/year were hospitalized in the US between 2005-2009 for HE
Pathophysiology
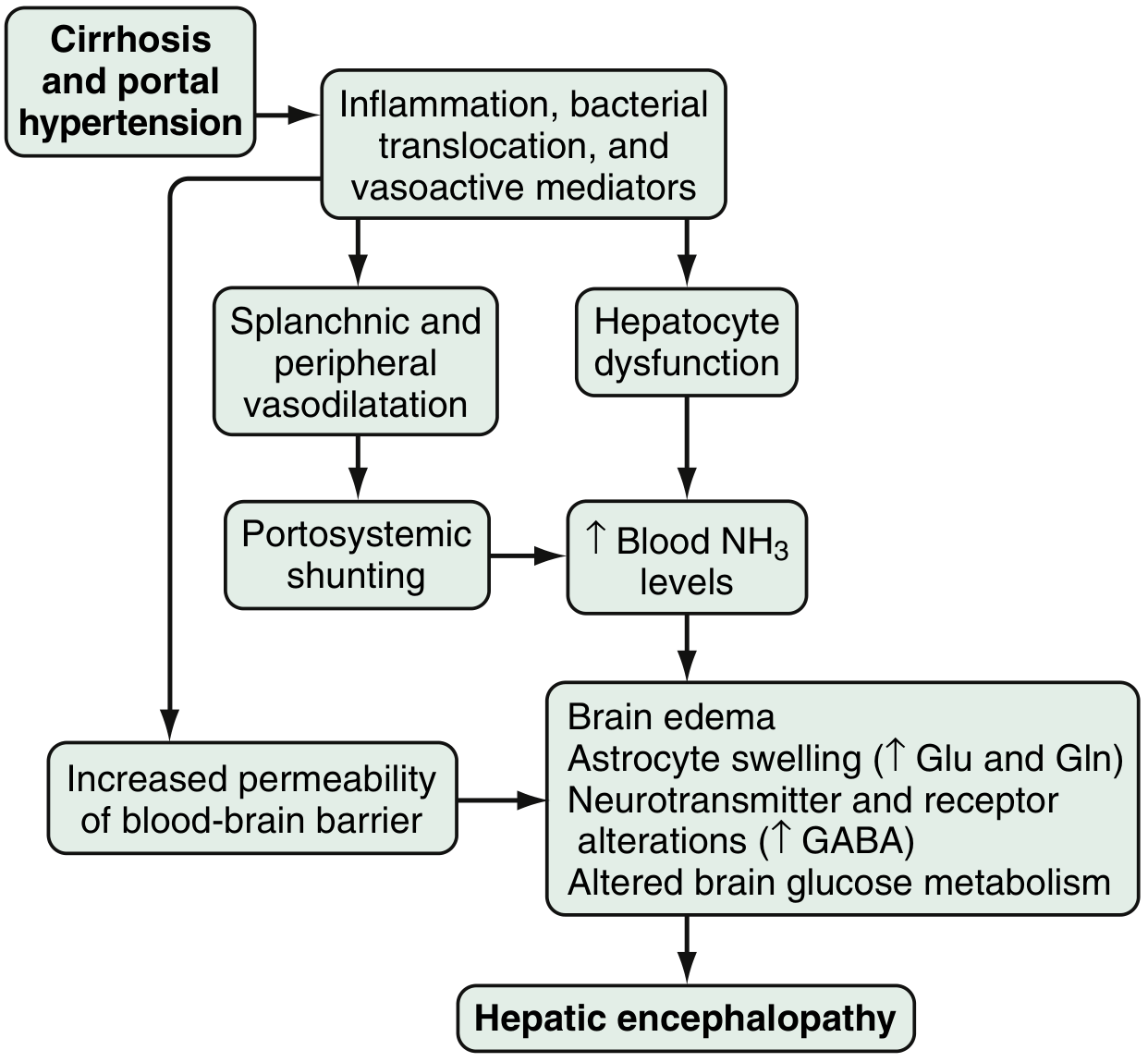
Proposed pathophysiology of HE - Sleisenger and Fordtran's GI and Liver Disease, Fig. 94.1
The precise mechanisms are multifactorial. Key contributors include:
1. Ammonia Toxicity (Primary mechanism)
- Source: Produced in the colon by bacterial metabolism of proteins and nitrogen products; enterocytes synthesize ammonia from glutamine
- Normally: Cleared by hepatocytes via conversion to urea
- In cirrhosis: Reduced hepatocyte function + portosystemic shunting = elevated circulating ammonia (present in up to 90% of HE patients)
- Brain effects: Ammonia crosses the blood-brain barrier, combines with alpha-ketoglutarate and glutamate to form glutamine, causing astrocyte swelling, cytotoxic brain edema, and disruption of GABA receptors
- Note: serum ammonia levels correlate inconsistently with severity of encephalopathy
2. GABA-Benzodiazepine System
- Increased sensitivity of astrocyte (peripheral-type) benzodiazepine receptors
- Enhanced activation via neurosteroids (allopregnanolone, tetrahydrodeoxycorticosterone) produced by astrocytes
- Results in CNS inhibition
3. Other Neurotoxins and Factors
- Mercaptans (products of methionine metabolism by gut bacteria) - cause fetor hepaticus
- Manganese toxicity causing dopaminergic dysfunction
- Serotonin (5-HT), nitric oxide, circulating opioid peptides
- Increased blood-brain barrier permeability
- Colonic mucosal microbiota alterations in cirrhotics with HE
- Genetic factors: allelic mutations in the glutaminase gene increase risk for overt HE
Classification
By Underlying Disease (Type)
| Type | Description |
|---|---|
| Type A | Associated with Acute Liver Failure (ALF) |
| Type B | Associated with portosystemic shunts, no hepatocellular disease |
| Type C | Associated with chronic/end-stage liver disease + portal hypertension (most common) |
By Severity: West Haven Criteria + SONIC Classification
| Grade (West Haven) | Intellectual Function | Neuromuscular Function | SONIC Category |
|---|---|---|---|
| 0 | Normal | Normal | Unimpaired |
| Minimal | Normal exam; subtle changes in work or driving | - | Covert HE |
| 1 | Trivial lack of awareness, euphoria/anxiety, shortened attention span | Impaired addition/subtraction | Covert HE |
| 2 | Disorientation to time, lethargy, personality change | Asterixis, slurred speech | Overt HE |
| 3 | Profound confusion, stupor, delirium | Asterixis, hyperreflexia, extensor plantar sign | Overt HE |
| 4 | Coma, unresponsive to painful stimuli | Decerebrate/decorticate posturing | Overt HE |
SONIC (spectrum of neurocognitive impairment in cirrhosis) simplifies grading: unimpaired / covert / overt - Sleisenger and Fordtran's, Table 94.1
Clinical Features
- Subtle (early): Forgetfulness, reversal of sleep-wake cycle, handwriting changes, difficulty driving
- Moderate: Confusion, personality changes, disorientation, dishinibited behavior
- Severe: Stupor, coma (grades 3-4)
Key Signs:
- Asterixis - low-amplitude alternating flexion/extension of the wrist when held in dorsiflexion; also elicited in the dorsiflexed foot or extended neck. Characteristic of grade 1-2 HE.
- Fetor hepaticus - musty breath odor from mercaptans; seen in severe cases
- Signs of underlying cirrhosis: spider angiomata, testicular atrophy, muscle wasting, superficial bruising, gynecomastia, ascites
Intracranial hypertension and cerebral edema are invariably present in grade 4, potentially causing brainstem herniation - the most common cause of death on postmortem. Seizures occur in 10-30% of pediatric patients.
Common Precipitating Factors
| Precipitant | Mechanism |
|---|---|
| GI bleeding | Increased nitrogen load in gut |
| Infection/sepsis | Systemic inflammation |
| Electrolyte disturbances (hypokalemia, alkalosis) | Increased ammonia production/absorption |
| Sedative/opioid medications | CNS depression |
| Dehydration / hypovolemia | Concentrated nitrogenous load |
| Constipation / ileus | Prolonged gut contact time |
| Acute/chronic kidney injury | Reduced urea excretion |
| Venous thrombosis | Increased shunting |
Differential Diagnosis
All causes of altered sensorium must be considered, particularly:
- Hypoglycemia
- Hyponatremia
- Drug/toxin ingestion
- Structural intracranial lesions (intracranial hemorrhage - especially given coagulopathy)
- Wernicke's encephalopathy (common in cirrhotics)
Focal neurological deficits increase likelihood of intracranial pathology.
Diagnostic Testing
- Serum ammonia: Generally elevated; does NOT correlate consistently with severity
- LFTs + albumin + INR/PT: Hepatic synthetic function is typically abnormal; normal results do NOT exclude HE
- Serum electrolytes, creatinine, glucose: Identify and correct precipitants
- Blood cultures, UA: Rule out infection
- Neuropsychological tests / EEG / Critical Flicker Frequency (CFF): For detecting minimal/covert HE
- EEG: Early slowing of alpha rhythm progressing to delta frequencies; triphasic waves in late stage (portend poor prognosis)
- Brain MRI: T1 hyperintensity of globus pallidus (manganese deposition); cerebral edema, atrophy; spectroscopy shows elevated glutamine
- CSF: Elevated glutamine concentrations
Management
1. Airway and Supportive Care (First Priority)
- Assess airway - prevent aspiration, support respiration as needed
- Most patients are hemodynamically stable but have increased risk of GI bleeding
- Avoid CNS depressants and sedatives
2. Identify and Treat Precipitating Cause
- Correct hypokalemia, alkalosis, hyponatremia, hypoglycemia, azotemia, dehydration
- Treat GI bleeding, infection, constipation
3. Lower Ammonia (Core Pharmacotherapy)
Lactulose (First-line)
- Nonabsorbable disaccharide
- Mechanism: osmotic cathartic effect + alters colonic pH to trap ammonia as ammonium (NH4+) in stool
- Dose: 30-60 g orally, or 200 g rectally daily - titrate to 2-3 loose stools/day
- In obtunded patients: administer via nasogastric tube or rectal enema
- Side effect: excessive diarrhea causing fluid and electrolyte imbalances
- PEG (polyethylene glycol) combination: A non-inferiority trial showed faster 24-hour improvement in HE severity scoring with lactulose + PEG 280 g/day vs lactulose alone
Rifaximin (Preferred antibiotic)
- Minimally absorbed oral antimicrobial agent concentrating in the GI tract
- Reduces ammonia-producing enteric bacteria
- Fewer systemic side effects than neomycin - preferred agent
- Often used in combination with lactulose for maintenance prevention of recurrence
Neomycin (Alternative antibiotic)
- Reserved for patients intolerant/contraindicated to rifaximin
- Dose: 250 mg PO q6-12h (max 4000 mg/day)
- Risks: ototoxicity and nephrotoxicity (limits use)
Other antibiotics: Vancomycin, metronidazole (less commonly used)
Branched Chain Amino Acids (BCAAs)
- Multiple trials show benefit without increased mortality or impact on nutrition or quality of life
- Should be strongly considered in patients with HE
L-Ornithine-L-Aspartate (LOLA)
- Less commonly used in the US; demonstrated benefit in lowering postprandial serum ammonia
- Useful after TIPS procedures (which can exacerbate HE)
4. Liver Transplantation
- Generally reverses HE
- Should be considered in eligible patients with end-stage liver disease
Pharmacological Cautions in HE Patients
Liver disease significantly alters drug pharmacokinetics:
- Hypoalbuminemia: Increased free drug concentrations for highly protein-bound drugs (phenytoin, morphine, beta-lactams, vancomycin, daptomycin) - dose adjustment needed
- Decreased hepatic metabolism: Drugs with large first-pass extraction have increased bioavailability and higher serum levels
- Decreased glutathione + impaired renal elimination: Predispose to drug toxicity and further liver injury
Prognosis
- Cumulative survival: 20-40% at 1 year and 15% at 3 years without liver transplantation
- Occurrence of HE is a poor prognostic indicator in cirrhosis
- Most deaths in severe HE result from brainstem herniation secondary to cerebral edema
- Minimal HE interferes with daily activities (impaired driving, work performance) and is underdiagnosed
Sources:
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Chapters 94 & 132)
- ROSEN's Emergency Medicine: Concepts and Clinical Practice (Chapter 76)
- Bradley and Daroff's Neurology in Clinical Practice (Chapters 84 & 13)
- Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Recent evidence note: A 2026 systematic review (PMID 41942881) on risk prediction models for HE in cirrhosis and a 2025 review on HE in non-cirrhotic portal hypertension (PMID 40081810) highlight ongoing refinement of risk stratification tools.
This is a shared conversation. Sign in to Orris to start your own chat.