Selective neck dissection and extended neck dissection in detail according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from Cummings Otolaryngology to write a detailed, textbook-quality answer. Let me compile the full response.
Selective Neck Dissection and Extended Neck Dissection
Based primarily on Cummings Otolaryngology: Head and Neck Surgery (Chapter 118) and Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Background: Classification Framework
The American Head and Neck Society (AHNS) classifies all cervical lymphadenectomy procedures relative to the radical neck dissection (RND) as the standard baseline:
- Modified radical neck dissection (MRND) - RND with preservation of one or more nonlymphatic structures
- Selective neck dissection (SND) - preservation of one or more lymph node groups routinely removed in RND
- Extended neck dissection - removal of additional lymph node groups or nonlymphatic structures beyond the RND
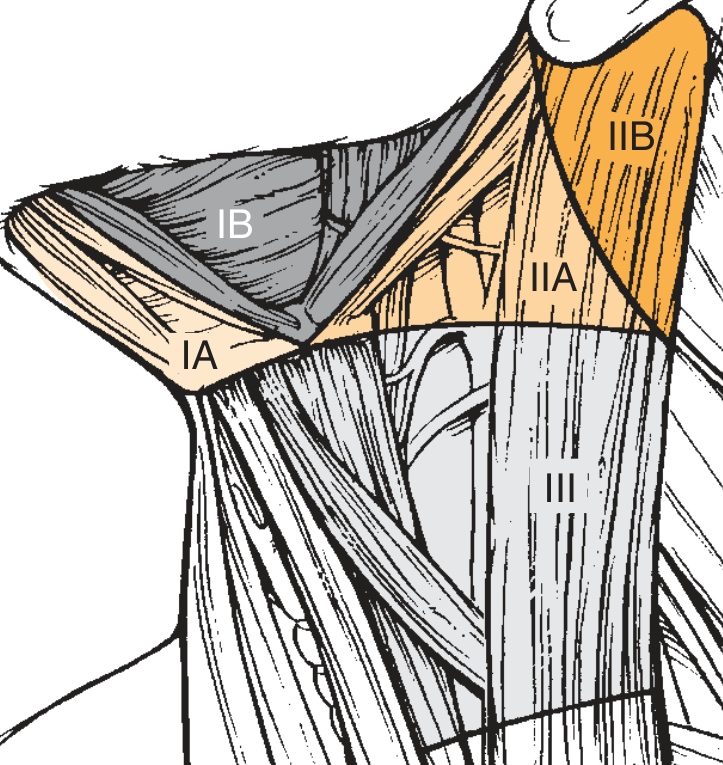
Lymph node levels are numbered I through VI (with sublevels IA, IB, IIA, IIB, VA, VB), and the notation uses Roman numerals to specify which levels are removed. A 2010 international consensus proposed using the symbol ND with prefixes L (left) or R (right) and listing removed levels and structures by standardized acronyms (SCM, IJV, CN XI, CN XII, ECA, ICA, etc.).
Selective Neck Dissection (SND)
Definition
SND is the en bloc removal of one or more specific lymph node groups at risk for harboring metastatic cancer, based on the known pattern of spread from the primary tumor site, while preserving all nonlymphatic structures (SCM, IJV, spinal accessory nerve). The levels removed are determined by the location of the primary lesion.
Rationale
- The concept dates to procedures used for lip cancer but was popularized broadly by surgeons at M.D. Anderson Cancer Center.
- It is grounded in the anatomic studies of Rouviere and Fisch & Sigel, which showed lymphatic drainage of mucosal head and neck surfaces follows relatively constant and predictable routes.
- Lindberg (1972) clinically validated this: jugulodigastric and midjugular nodes are most often involved in oral cavity carcinoma; submandibular triangle nodes are at risk for floor-of-mouth, anterior tongue, and buccal carcinomas.
- Shah subsequently showed oral cavity tumors metastasize mainly to levels I, II, III; pharyngeal, hypopharyngeal, and laryngeal tumors involve mainly levels II, III, IV.
- Key principle: when positive nodes were found in unexpected levels, disease was invariably also present in the highest-risk levels - supporting site-specific surgery.
- Studies have shown SND has equivalent therapeutic value to more extensive neck dissections for early nodal disease (N0/N1).
Types of Selective Neck Dissection
1. SND (I-III) - Supraomohyoid Neck Dissection
Indication: Oral cavity cancers (tongue, floor of mouth, buccal mucosa, alveolar ridge, lip)
Levels removed: IA, IB, IIA, IIB, III
Boundaries:
- Superior: lower border of mandible
- Inferior: junction of the superior belly of the omohyoid with the internal jugular vein (IJV)
- Anterior (medial): anterior belly of contralateral digastric
- Posterior (lateral): cutaneous branches of cervical plexus and posterior border of SCM
Rationale details:
- Primary echelons for oral cavity spread: submental, submandibular, upper and middle jugular groups
- For tongue cancer, level IV is also at risk - SND (I-IV) is recommended
- Floor of mouth/ventral tongue midline lesions: elective contralateral neck dissection is also indicated
- Risk of occult disease in oral cavity cancers is at least 20% even without clinical evidence
- For N1 disease confined to levels I-II, SND (I-IV) is appropriate with planned postoperative RT
Technique highlights:
- Incision: modified apron incision (ipsilateral) or bilateral apron incision for bilateral cases
- If lip-splitting is needed: bilateral boomerang incision
- If all 5 levels need dissection (advanced nodal disease with oral primary): boomerang incision is preferred
2. SND (II-IV) - Lateral Neck Dissection
Indication: Oropharyngeal, laryngeal, and hypopharyngeal cancers
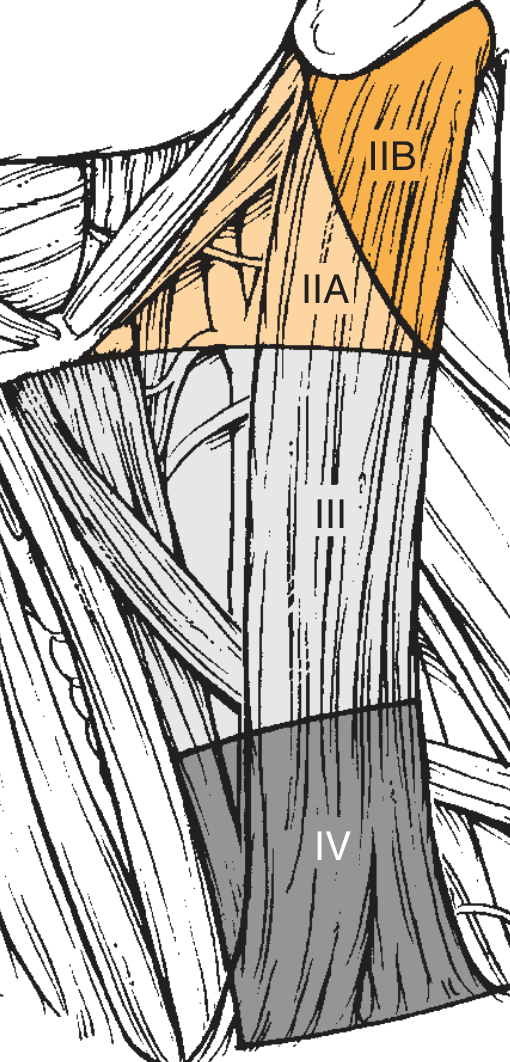
Levels removed: IIA, IIB, III, IV
Boundaries:
- Superior: skull base
- Inferior: clavicle
- Anterior (medial): lateral border of sternohyoid and stylohyoid muscles
- Posterior (lateral): cutaneous branches of cervical plexus and posterior border of SCM
Special considerations:
- For laryngeal and hypopharyngeal cancers: level IIB has lower risk in N0 disease, so some surgeons omit it - designated SND (IIA, III, IV)
- For oropharyngeal cancers: level IIB carries greater risk; should be included. Evidence suggests lateral retropharyngeal nodes are also at risk - in that case designated SND (II-IV, retropharyngeal nodes)
- For laryngeal/hypopharyngeal cancers extending below the glottis: level VI (central compartment) should be added - SND (II-IV, VI)
- Controversy: some studies suggest levels I-III are at risk in N0 oropharyngeal cancer, possibly due to misidentification of deep SG nodes as level IB
Technique highlights:
- Incision: hockey stick incision (can be extended bilaterally for bilateral SND)
- In the era of minimally invasive/robotic oropharyngeal surgery, there is a trend toward smaller incisions
3. SND (II-V) - Posterolateral Neck Dissection
Indication: Cutaneous malignancies (melanoma, squamous cell carcinoma) and soft tissue sarcomas of the posterior scalp and upper neck
Levels removed: II, III, IV, V (posterolateral), plus suboccipital and retroauricular (postauricular) lymph nodes
Boundaries:
- Superior: skull base anteriorly, nuchal ridge posteriorly
- Inferior: clavicle
- Anterior (medial): lateral border of sternohyoid and stylohyoid
- Posterior (lateral): anterior border of trapezius (inferior) and midline (superior)
Rationale: Lymphatic pathways from posterior scalp seed into posterior auricular, occipital, posterior triangle, and jugular groups. The dissection must encompass all of these, plus intervening subdermal fat and underlying fascia between lymph node groups and the primary.
Additional site-specific variations:
- Preauricular, anterior scalp, temporal malignancies: SND of parotid + facial nodes, levels IIA, IIB, III, VA, and external jugular nodes
- Anterior/lateral face malignancies: SND of parotid + facial nodes, levels IA, IB, II, III
Technique highlights:
- Incision: lazy-S pattern or hockey stick with horizontal extension along nuchal ridge
- Position: lateral decubitus (or prone for bilateral posterior scalp midline lesions)
- Skin flaps: subplatysmal plane anteriorly, subdermal plane posteriorly
- Posterior auricular and suboccipital nodes lie very superficially just below skin - dissection must go to fascia of upper neck muscles
- Upper trapezius attachment to skull base is divided to expose deep suboccipital nodes along the occipital artery
- SAN is routinely preserved unless directly invaded
4. SND (I-IV) and SND (II-IV, VI) - Additional Variants
- SND (I-IV): used for tongue cancers with level IV risk, or N1 disease confined to upper neck in oral cavity cancer
- SND (VI): central compartment dissection; used for thyroid cancer, laryngeal/hypopharyngeal cancers with subglottic extension; involves removal of paratracheal lymph nodes with en bloc thyroid resection, preserving recurrent laryngeal nerves
SND as a Staging and Therapeutic Tool
SND serves a dual role:
- Elective (staging) purpose: Removes at-risk node groups in clinically N0 patients; provides pathologic information - if multiple positive nodes or extracapsular spread (ECS) found, postoperative RT is indicated
- Therapeutic purpose: Can be used for N1 disease confined to the dissected levels, but N2/N3 disease usually requires MRND or comprehensive dissection
Postoperative RT indications after SND:
- Multiple lymph node metastases in specimen
- Extracapsular spread (ECS)
- N1 disease (Byers et al. showed lower regional recurrence with adjuvant RT in N1)
- With very rare exception of a solitary node without ECS, positive pathologic nodes warrant postoperative RT
Extended Neck Dissection
Definition
Any of the standard neck dissections (RND, MRND, or SND) that is extended to remove additional lymph node groups or vascular, neural, or muscular structures not routinely removed in a standard neck dissection.
Indications
Extended neck dissection is performed when:
- Nodal disease extent requires removal of additional lymph node groups not covered by standard dissection
- Direct tumor invasion of nonlymphatic structures makes en bloc resection necessary for oncologic clearance
Extension to Additional Lymph Node Groups
Retropharyngeal Lymph Nodes
- Indication: Primary tumors of the pharyngeal walls (posterior and lateral pharyngeal wall, tongue base, tonsil, soft palate, retromolar trigone involving the oropharyngeal walls)
- Incidence: Ballantyne reported a 44% incidence of retropharyngeal node involvement in carcinomas of the pharyngeal wall treated surgically
- Tumors of tongue base and tonsil may spread here when they involve the lateral/posterior oropharyngeal walls
- Designated as: SND (II-IV, retropharyngeal nodes) or extended MRND with retropharyngeal clearance
Level VII (Superior Mediastinal) Nodes
- Removal may be required for thyroid cancers or other tumors with paratracheal/mediastinal extension
Extension Involving Nonlymphatic Structures
1. Carotid Artery Resection
The most controversial aspect of extended neck dissection.
Arguments against:
- Dismal prognosis in patients with disease of sufficient extent to warrant carotid resection
- Moore and Baker reported 30% mortality and 45% cerebral complication rate with carotid ligation (includes elective + emergency)
- Only ~18% of patients who had tumor "peeled off" the carotid developed neck recurrence without distant metastases (Kennedy et al.) - suggesting only this minority benefits
Arguments for (selected patients):
- Improved methods of preoperative cerebral circulation assessment (contralateral carotid sufficiency testing)
- Better vascular reconstruction techniques: saphenous vein grafts preferred over prosthetic
- McCready et al. (16 patients): only 12% developed cerebrovascular complications; 45% free of disease at 1 year
- Encouraging results with intraoperative iodine seed sutures over remaining artery after gross tumor removal (Paryan, Goffinet, Fee): 77% neck tumor control, 15% disease-free at 1 year
Current recommendation:
- Patients with frank carotid wall involvement who demonstrate intolerance of carotid ligation on preoperative testing should undergo carotid resection and reconstruction
- Saphenous vein graft is preferred; if skin over carotid is heavily irradiated or resected, a myocutaneous flap must cover the graft
2. Hypoglossal Nerve (CN XII)
- Resected when the nerve is directly invaded by metastatic disease
- In the AHNS 2010 proposed notation: listed explicitly as CN XII in the dissection description
- Results in ipsilateral tongue deviation, dysarthria, and dysphagia
3. Other Structures
- Levator scapulae muscle - may be resected when disease extends to the posterior triangle floor
- Deep cervical muscles - when invaded by nodal disease or soft tissue spread
- Skin - when overlying skin is directly involved by tumor; requires reconstruction with myocutaneous flap
- Parotid gland - when parotid nodes are involved in cutaneous malignancies
- External carotid artery (ECA) and its branches - occasionally resected for vascular control or tumor adherence
AHNS Nomenclature Comparison (Table 118.4 from Cummings)
| Proposed ND Notation (2010) | AHNS 2008 Classification |
|---|---|
| I-V, SCM, IJV, CN XI | Radical neck dissection |
| I-V, SCM, IJV, CN XI, CN XII | Extended radical neck dissection (with hypoglossal nerve) |
| I-V, SCM, IJV - CN XI preserved | MRND (spinal accessory nerve preserved) |
| II-IV | Selective neck dissection (II-IV) |
| II-IV, VI | Selective neck dissection (II-IV, VI) |
| II-IV, SCM | Not applicable (nonstandard) |
| I-III | Selective neck dissection (I-III) |
Summary Table: SND Types by Primary Site
| SND Type | Levels Removed | Primary Site Indication |
|---|---|---|
| Supraomohyoid (SND I-III) | IA, IB, IIA, IIB, III | Oral cavity (floor of mouth, tongue, buccal, alveolar) |
| SND (I-IV) | IA-IB, II-IV | Oral tongue, N1 oral cavity disease |
| Lateral (SND II-IV) | IIA, IIB, III, IV | Oropharynx, larynx, hypopharynx |
| SND (II-IV, VI) | IIA, IIB, III, IV, VI | Subglottic/hypopharyngeal with central spread |
| Posterolateral (SND II-V) | II, III, IV, V + suboccipital/retroauricular | Posterior scalp, cutaneous malignancies, sarcomas |
| SND (VI) | Central compartment only | Thyroid cancer, glottic/subglottic larynx |
Key Points
- SND removes only the lymph node groups at highest statistical risk based on the primary site, while preserving all nonlymphatic structures.
- It has equivalent therapeutic efficacy to comprehensive neck dissection for early nodal disease (N0/N1).
- Postoperative RT is indicated for virtually all patients with pathologically positive nodes in SND specimens, except possibly a single node without ECS.
- Extended neck dissection is needed when tumor involves structures beyond the standard dissection boundaries, or when additional nodal groups (retropharyngeal, superior mediastinal) are at risk.
- Carotid artery resection in extended dissection carries significant morbidity and should be reserved for selected patients with frank wall invasion and adequate cerebrovascular reserve.
- The AHNS 2010 international notation (ND + side + levels + structures) provides precise, universally communicable descriptions of any cervical lymphadenectomy.
Sources: Cummings Otolaryngology Head and Neck Surgery, Ch. 118 (Ronen, Samant, Robbins), pp. 2292-2308; Scott-Brown's Otorhinolaryngology Head and Neck Surgery, Vol. 3.
This is a shared conversation. Sign in to Orris to start your own chat.