Common fracture in upper limb
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Here is a structured overview of the common fractures of the upper limb, drawn from authoritative orthopaedic and surgical textbooks.
Common Fractures of the Upper Limb
1. Clavicle Fracture
Most common fracture in children; accounts for ~90% of obstetric fractures.
Mechanism:
- Birth injury: direct pressure from the symphysis pubis
- Older children/adults: fall on an outstretched hand (FOOSH), or direct trauma to the clavicle or acromion
Diagnosis:
- Standard AP X-ray; cephalic tilt views (35-40 degrees) are helpful
- CT for medial clavicle fractures or physeal separation evaluation
Classification: Middle-third fractures are most common (~80%)
Treatment:
- Newborns and most children/adolescents: non-operative (figure-of-8 sling or arm sling)
- Operative (plate fixation or IM nailing) for: open fractures, neurovascular compromise, displacement >2 cm, nonunion/malunion
Complications: Nonunion (1-3%), malunion, pneumothorax, neurovascular injury
- Miller's Review of Orthopaedics, 9th ed.
2. Fracture Neck of Humerus (Surgical Neck)
Very common in older adults (osteoporosis-related) and children (physeal injuries).
Mechanism:
- Fall on outstretched hand - upward thrust breaks the surgical neck and may shear off the greater tuberosity
- Direct blow to the shoulder -> anatomical neck fracture (rarer)
Types:
- Adduction type: inner halves of fractured ends are impacted
- Abduction type: outer halves are impacted, shaft remains abducted; greater tuberosity may be avulsed
Anatomy note: The axillary nerve and posterior circumflex humeral artery may be at risk, but injury is uncommon.
Treatment: Varies from conservative (collar and cuff, sling) to ORIF or hemiarthroplasty depending on displacement and patient factors.
- S Das Manual on Clinical Surgery, 13th ed.; Gray's Anatomy for Students
3. Colles' Fracture (Distal Radius)
The commonest wrist injury in adults.
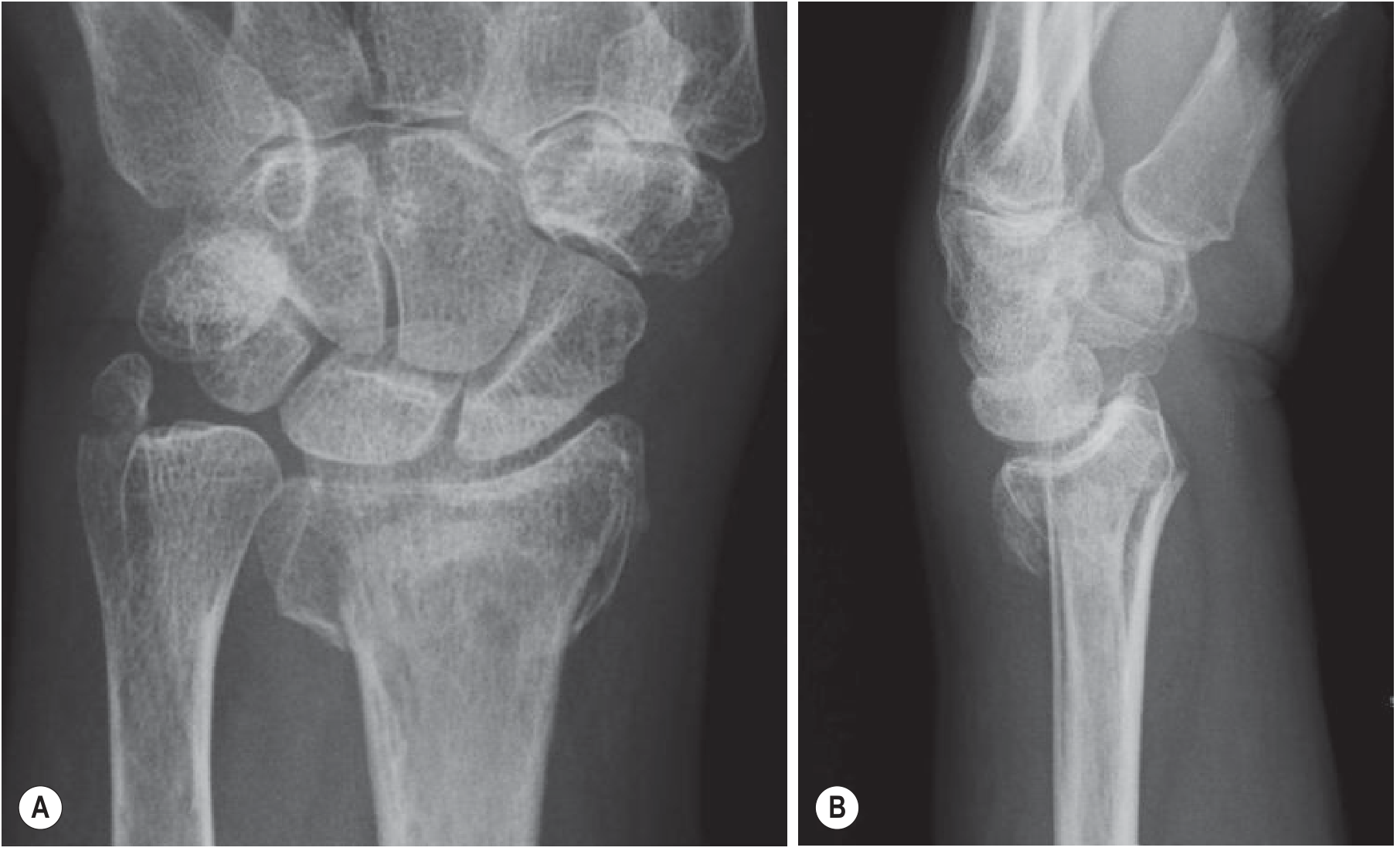
Definition: Fracture of the radius within 2 cm of the distal radial articular surface, with dorsal angulation/displacement of the distal fragment, often with an associated ulnar styloid fracture. (First described by Colles in 1814.)
Mechanism: Fall on outstretched hand (FOOSH) with wrist in dorsiflexion
Classic deformity: "Dinner fork" deformity (dorsal displacement)
Treatment:
- Undisplaced: below-elbow cast
- Displaced: closed reduction + cast; unstable fractures may need K-wires, external fixation, or ORIF
Related distal radius fractures:
| Fracture | Displacement | Mechanism |
|---|---|---|
| Colles' | Dorsal (most common) | Fall on dorsiflexed wrist |
| Smith's ("reversed Colles'") | Volar | Fall on volar-flexed wrist |
| Barton's | Rim fracture + radiocarpal subluxation | Shearing injury |
| Chauffeur's (Hutchinson) | Radial styloid, intra-articular | Axial load through scaphoid |
- Grainger & Allison's Diagnostic Radiology; Rockwood and Green's Fractures in Adults, 10th ed. 2025
4. Scaphoid Fracture
Accounts for ~60% of all carpal fractures. Most commonly missed fracture.
Mechanism: FOOSH in a young adult
Key anatomy: Blood supply enters distally and is retrograde - a displaced waist fracture interrupts supply to the proximal pole, risking avascular necrosis (AVN).
Diagnosis trap: May NOT be visible on initial X-rays. If the patient has anatomical snuff box tenderness after FOOSH, treat as scaphoid fracture until excluded.
Protocol for suspected scaphoid fracture (not visible on X-ray):
- Immobilise the wrist
- Re-examine at 10-14 days; repeat scaphoid views if tender
- If resources allow: bone scan, MRI, or CT for earlier diagnosis
Treatment:
- Undisplaced: below-elbow cast (thumb spica not mandatory)
- Displaced (>1 mm) or unstable: ORIF with headless compression screw
Complications: Non-union, AVN (proximal pole), malunion, carpal instability
- Bailey and Love's Short Practice of Surgery, 28th ed.; Tintinalli's Emergency Medicine
5. Supracondylar Fracture of the Humerus
The most common elbow fracture in children (typically age 5-10 years).
Mechanism: FOOSH with elbow in extension (extension type, >95%) - child presents holding swollen, flexed elbow with the opposite hand.
Treatment by displacement:
- Undisplaced: collar and cuff / backslab for 3 weeks, then mobilisation
- Displaced with intact periosteal hinge: closed reduction + above-elbow cast (3-4 weeks)
- Displaced with broken periosteal hinge: closed reduction + percutaneous K-wires + above-elbow cast
Complications (critical to recognise):
-
Volkmann's ischaemic contracture - from missed compartment syndrome; avoid deep elbow flexion if swollen
-
Vascular injury: The "white pulseless hand" = surgical emergency; requires urgent reduction + vascular exploration if pulse doesn't return
-
"Pink pulseless hand": Controversial; requires senior decision-making; if adequate perfusion, stabilise fracture then reassess vascularity
-
Nerve injury: Anterior interosseous nerve (AIN) most commonly affected (weakness of thumb and index flexion)
-
Bailey and Love's Short Practice of Surgery, 28th ed.
Summary Table
| Fracture | Typical Patient | Mechanism | Key Sign | Main Complication |
|---|---|---|---|---|
| Clavicle | Children, neonates | FOOSH / direct blow | Tenderness midclavicle | Pneumothorax, neurovascular injury |
| Surgical neck of humerus | Elderly (osteoporosis) | FOOSH / direct | Limited shoulder movement | Axillary nerve injury |
| Colles' | Middle-aged women | FOOSH (dorsiflexion) | Dinner fork deformity | Malunion, tendon rupture |
| Scaphoid | Young adults | FOOSH | Snuff box tenderness | AVN, non-union |
| Supracondylar | Children (5-10 yr) | FOOSH (elbow extension) | Swollen flexed elbow | Volkmann's contracture, vascular injury |
Key mnemonic: Most upper limb fractures share a common mechanism - FOOSH (Fall On OutStretched Hand) - but produce different fractures depending on the patient's age, bone quality, and exact position of the limb at impact.
This is a shared conversation. Sign in to Orris to start your own chat.