Explain the development of urinary system and prostate gland along with all clinicals
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Now I have all the content needed for a comprehensive answer. Let me compile it.
Development of the Urinary System and Prostate Gland
Sources: The Developing Human - Clinically Oriented Embryology (Moore); Campbell-Walsh-Wein Urology
PART 1: DEVELOPMENT OF THE URINARY SYSTEM
Overview and Origin
The urinary system begins development before the genital system. Both systems arise from intermediate mesenchyme (mesoderm) of the dorsal body wall, and together form the urogenital system. The urinary system consists of:
- Kidneys (produce and excrete urine)
- Ureters (convey urine to the bladder)
- Urinary bladder (stores urine)
- Urethra (discharges urine)
DEVELOPMENT OF KIDNEYS AND URETERS
Three successive sets of kidney structures develop in humans, from cranial to caudal, each building on the remnants of the last.
1. Pronephroi (Week 4)
- Appear early in the 4th week as a few bilateral cell clusters and tubular structures in the cervical (neck) region
- The pronephric ducts run caudally and open into the cloaca (a common chamber receiving hindgut and allantois)
- These rudimentary structures are non-functional in humans
- The pronephroi soon degenerate, but most of their ducts persist and are adopted by the next kidney system
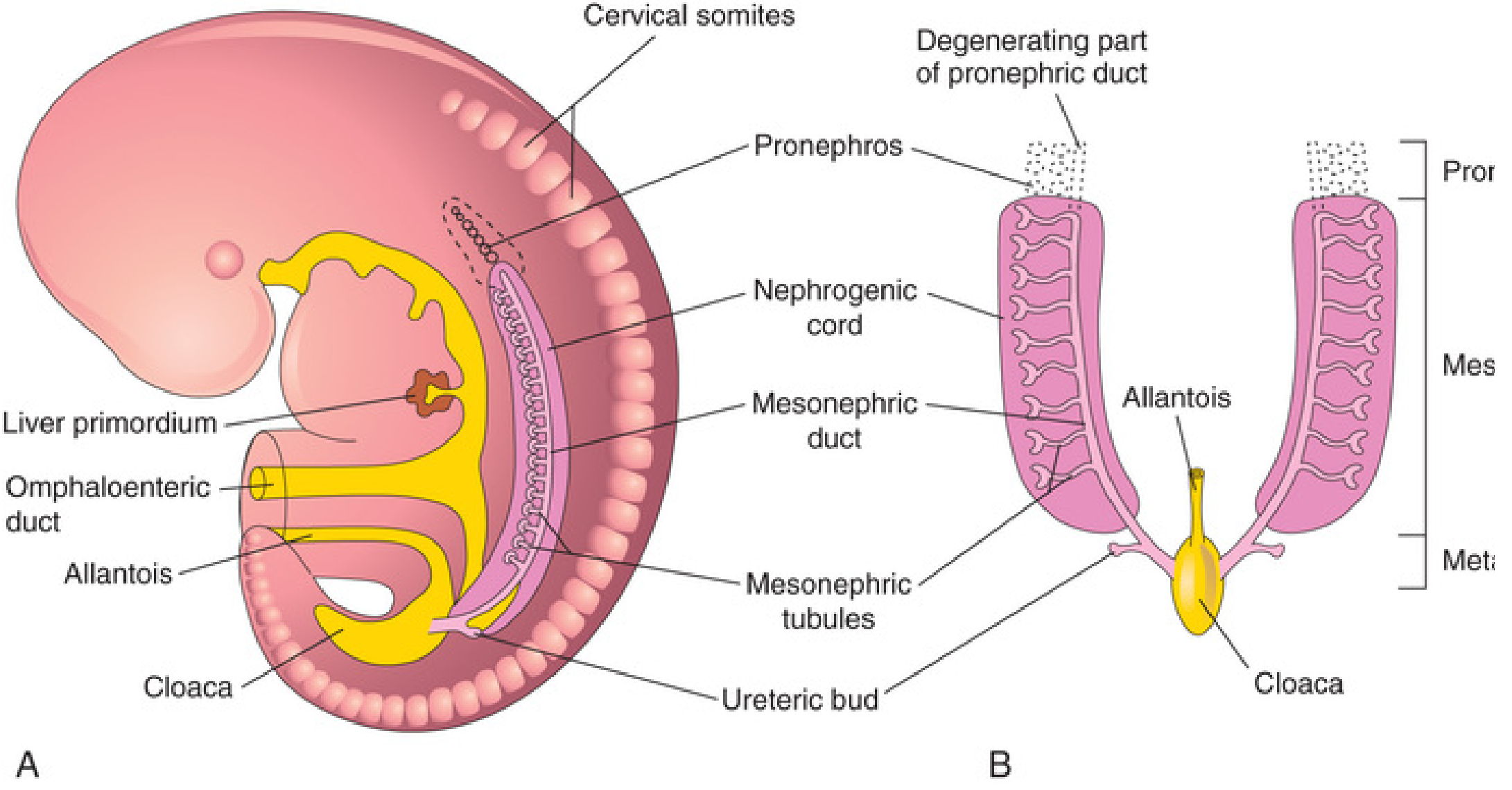
The three sets of kidney systems in a 5-week embryo. Note the pronephros cranially, the mesonephric tubules and duct in the middle zone, and the ureteric bud emerging caudally.
2. Mesonephroi (Late Week 4 - Week 12)
- Large, elongated excretory organs appearing late in week 4, caudal to pronephroi
- Function as interim kidneys for ~4 weeks until permanent kidneys develop
- Consist of 10-50 glomeruli per kidney and mesonephric tubules
- Tubules drain into mesonephric (Wolffian) ducts, which open into the cloaca
- Degenerate by end of week 12
- Important remnants in males:
- Mesonephric tubules become efferent ductules of the testes
- Mesonephric ducts form the epididymis, vas deferens, seminal vesicles, and ejaculatory ducts
3. Metanephroi - The Permanent Kidneys (Week 5 onward)
The permanent kidneys begin to develop in week 5 from two sources:
A. Ureteric Bud (Metanephric Diverticulum)
- Outgrowth from the mesonephric duct near its entry into the cloaca (week 5)
- Penetrates the metanephric blastema (metanephrogenic mesenchyme)
- Gives rise to: ureter, renal pelvis, calyces, collecting tubules
B. Metanephric Blastema (Metanephrogenic Mesenchyme)
- Derived from the caudal portion of the nephrogenic cord (intermediate mesoderm)
- Induced by the ureteric bud to form: nephrons (glomeruli, proximal tubules, loops of Henle, distal tubules)
Reciprocal Induction
The ureteric bud and metanephric mesenchyme engage in mutual inductive signaling:
- The ureteric bud induces the mesenchyme to differentiate into nephrons
- The mesenchyme induces the bud to branch and grow
- This reciprocal process continues until 32-36 weeks of gestation
Ascent of the Kidneys (Weeks 6-9)
- Initially, the metanephric kidneys lie in the pelvis
- They ascend to their lumbar position by weeks 6-9 due to:
- Body growth (caudal end elongates)
- Reduction in body curvature
- During ascent, the kidneys receive successive blood supplies from increasingly cranial aortic branches
- The hilum, initially facing ventrally, rotates 90 degrees medially
- The kidneys reach the suprarenal glands by week 9, fixing their final position
Changes in Blood Supply During Ascent
- Initially: renal arteries branch from common iliac arteries
- Then: blood supply from distal aorta
- Finally: permanent renal arteries from abdominal aorta (the most cranial branches)
- Caudal branches involute and disappear
Development of Urinary Bladder
- Derived from the upper part of the urogenital sinus (which forms when the urorectal septum divides the cloaca)
- The allantois (connecting to the umbilicus) becomes the urachus at its upper end - later obliterating into the median umbilical ligament
- As the bladder enlarges, distal mesonephric ducts are incorporated into its dorsal wall, contributing to the trigone
- The ureters open separately into the bladder and their orifices migrate superolaterally due to kidney ascent
- In males: mesonephric duct orifices move together to enter the prostatic urethra as ejaculatory ducts
- In infants and children, the bladder is in the abdomen even when empty; it enters the greater pelvis at ~6 years, and enters the true pelvis only after puberty
Development of Urethra
- Develops from the lower part of the urogenital sinus
- The entire epithelium of the male urethra (including the prostatic, membranous, and spongy parts) is of urogenital sinus origin
- The glandular urethra (glans penis) develops by canalization of an ectodermal ingrowth
CONGENITAL ANOMALIES OF THE URINARY SYSTEM
Renal Agenesis
| Type | Frequency | Features |
|---|---|---|
| Unilateral | ~1 in 1,000 neonates | Males > females; left kidney more common; surviving kidney undergoes compensatory hypertrophy; usually asymptomatic |
| Bilateral | ~1 in 3,000 neonates | Incompatible with life; causes oligohydramnios (Potter sequence) |
Potter Sequence (Bilateral Renal Agenesis):
- Absent kidneys → no fetal urine production → oligohydramnios
- Results in: pulmonary hypoplasia, Potter facies (flattened nose, recessed chin, low-set ears, skin folds under eyes), limb deformities (talipes equinovarus)
- Incompatible with postnatal life due to pulmonary hypoplasia
Cause: Failure of the ureteric bud to develop, OR failure of the metanephric blastema to respond to induction
Horseshoe Kidney
- Inferior poles fuse during ascent, usually across the inferior mesenteric artery (IMA) - which prevents further cranial migration
- The kidney lies lower than normal, with its hilum facing anteriorly
- Occurs in ~1 in 500 people; more common in males
- Most cases are asymptomatic; associated with increased risk of:
- Ureteropelvic junction (UPJ) obstruction and hydronephrosis
- Renal calculi
- Wilms tumor (nephroblastoma)
- Trisomy 18 (Edwards syndrome)
Pelvic Kidney (Ectopic Kidney)
- Kidney fails to ascend - remains in the pelvis
- May receive blood supply from iliac vessels or lower aorta
- Usually asymptomatic but predisposed to infection and hydronephrosis
- Occasionally discovered incidentally on imaging
Duplex Ureter / Double Collecting System
- Caused by early division of the ureteric bud before it contacts the metanephric blastema
- Results in two separate ureters (one or both sides)
- The ectopic ureter (from the upper moiety) inserts below the normal trigonal position, following the Weigert-Meyer rule:
- Upper moiety ureter: inserts inferomedially (ectopically) → tends to obstruct
- Lower moiety ureter: inserts superolaterally → tends to reflux
Accessory Renal Arteries
- Present in ~25% of adults (2-4 renal arteries)
- Arise from the aorta superior or inferior to the main renal artery
- An accessory artery crossing anterior to the ureter at the inferior pole can cause UPJ obstruction and hydronephrosis
- Accessory arteries are end arteries - ligation causes ischemic infarction of supplied tissue
- Approximately twice as common as accessory veins
Polycystic Kidney Disease
| Type | Inheritance | Mechanism | Presentation |
|---|---|---|---|
| Autosomal Recessive PKD (ARPKD) | AR - PKHD1 gene (fibrocystin) | Collecting duct dilation | Infants; bilateral enlarged kidneys; often lethal perinatally; associated with hepatic fibrosis |
| Autosomal Dominant PKD (ADPKD) | AD - PKD1 or PKD2 genes (polycystin) | All nephron segments | Young adults; flank pain, hematuria, hypertension, renal failure; associated with intracranial berry aneurysms and hepatic/pancreatic cysts |
Urachal Anomalies
The urachus (allantois remnant between bladder and umbilicus) normally obliterates to form the median umbilical ligament. Failure to obliterate leads to:
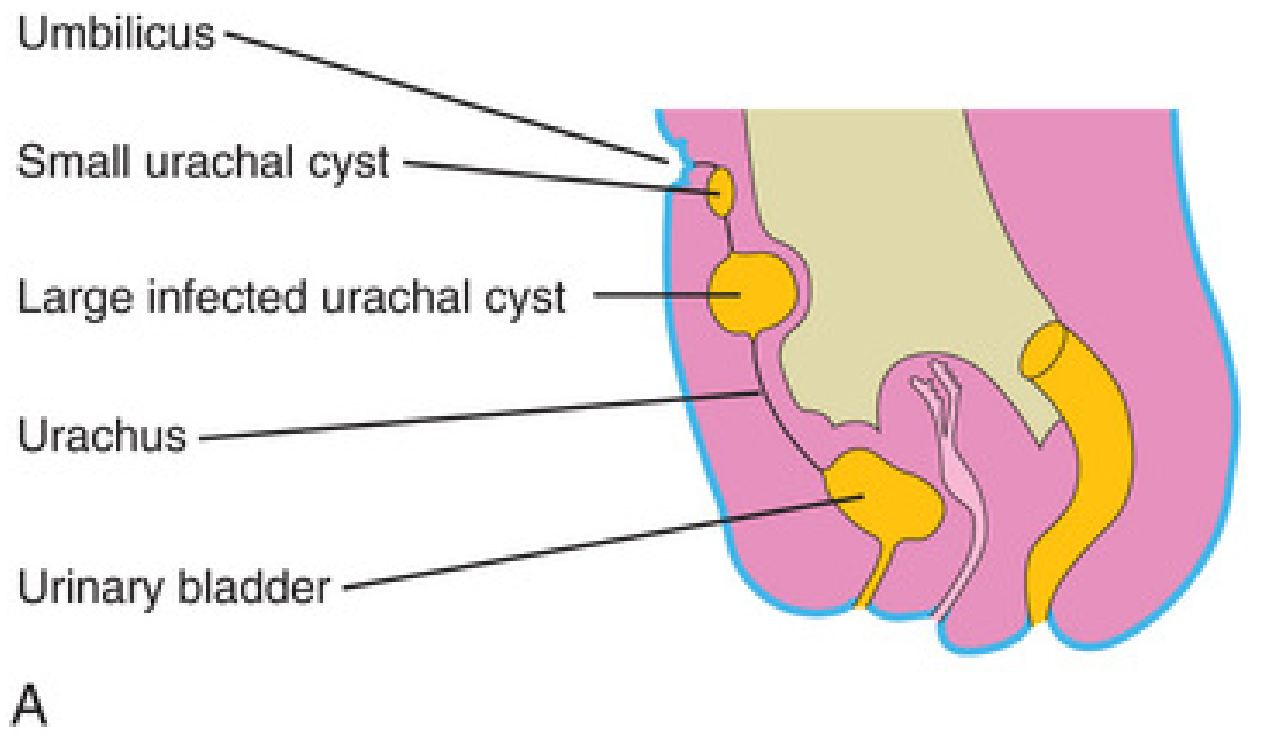
| Anomaly | Description | Clinical Feature |
|---|---|---|
| Urachal fistula (patent urachus) | Entire urachus remains open | Urine draining from umbilicus |
| Urachal sinus | Only superior end patent | Discharges at umbilicus |
| Urachal sinus (inferior) | Only inferior end patent | Opens into bladder |
| Urachal cyst | Middle portion remains (both ends closed) | Usually asymptomatic; presents when infected; midline infraumbilical mass |
Clinical note: Urachal remnants in adults carry a small but real risk of urachal carcinoma (adenocarcinoma), particularly if they become symptomatic in adulthood.
Vesicoureteral Reflux (VUR)
- The most common urinary tract anomaly in children
- Due to failure of the intramural ureter to develop an adequate submucosal tunnel
- Allows urine to reflux from bladder into ureters/kidneys during voiding
- Graded I-V (I = ureter only; V = massive dilation with intrarenal reflux)
- Predisposes to recurrent UTI and reflux nephropathy (scarring)
- May resolve spontaneously (lower grades); higher grades may need surgical correction
Bladder Exstrophy
- Failure of mesodermal migration to reinforce the anterior abdominal wall over the developing bladder
- Results in the posterior bladder wall being exposed on the abdominal surface
- Associated with epispadias in males
- Increased risk of bladder adenocarcinoma if untreated
- Requires surgical reconstruction
Renal Tubular Defects
- Congenital hydronephrosis - most commonly due to UPJ obstruction; detected prenatally on ultrasound
- Multicystic dysplastic kidney (MCDK) - non-hereditary; caused by atresia of the ureter early in development; kidney replaced by non-communicating cysts; usually unilateral; involutes over time
PART 2: DEVELOPMENT OF THE PROSTATE GLAND
Origin and Embryological Context
The prostate is a derivative of the primitive endoderm (gut tube). Development begins with regional differentiation of the cloaca:
- The urorectal septum divides the cloaca into a dorsal anorectal canal and ventral primitive urogenital sinus
- The urogenital sinus further differentiates into:
- Bladder (cranial portion)
- Pelvic urethra (middle portion - prostatic and membranous in males)
- Phallic urethra (caudal portion)
- The prostate develops from the pelvic portion of the urogenital sinus epithelium (UGE), specifically from FOXA1-positive endodermal cells
Androgenic Control of Prostate Development
- Fetal testes produce testosterone from Leydig cells under the stimulation of human chorionic gonadotropin (hCG), which peaks at weeks 8-12
- Within the urogenital sinus (UGS), testosterone is converted to dihydrotestosterone (DHT) by 5α-reductase
- DHT binds to androgen receptors (AR) in the urogenital sinus mesenchyme (UGM) - not the epithelium
- AR signaling in UGM is required for prostate induction via paracrine signaling to adjacent UGE (the "andromechanist" hypothesis)
- This was proven by recombination experiments: AR-null mesenchyme cannot induce prostate budding even in wild-type epithelium
Key point: Androgen exposure is necessary and sufficient to drive prostatic differentiation regardless of genetic sex, meaning female urogenital sinus epithelium grafted onto male mesenchyme will form prostate-like structures.
Stages of Prostate Development
Prostatic organogenesis passes through six overlapping stages:
| Stage | Timing | Event |
|---|---|---|
| 1 | Weeks 9-10 | Prostate lineage commitment - androgens act on UGM to prepare for budding |
| 2 | Weeks 9-10 | Solid epithelial buds emerge from UGE into surrounding mesenchyme at stereotyped locations; mesenchymal condensation precedes bud invasion |
| 3 | Week 11 onward | Bud elongation and branching in a specific spatial pattern establishing zonal subdivisions |
| 4 | Fetal period | Canalization of solid epithelial cords into ducts |
| 5 | Late fetal | Differentiation of luminal and basal epithelial cells |
| 6 | Late fetal/postnatal | Secretory cytodifferentiation |
Anatomical Development
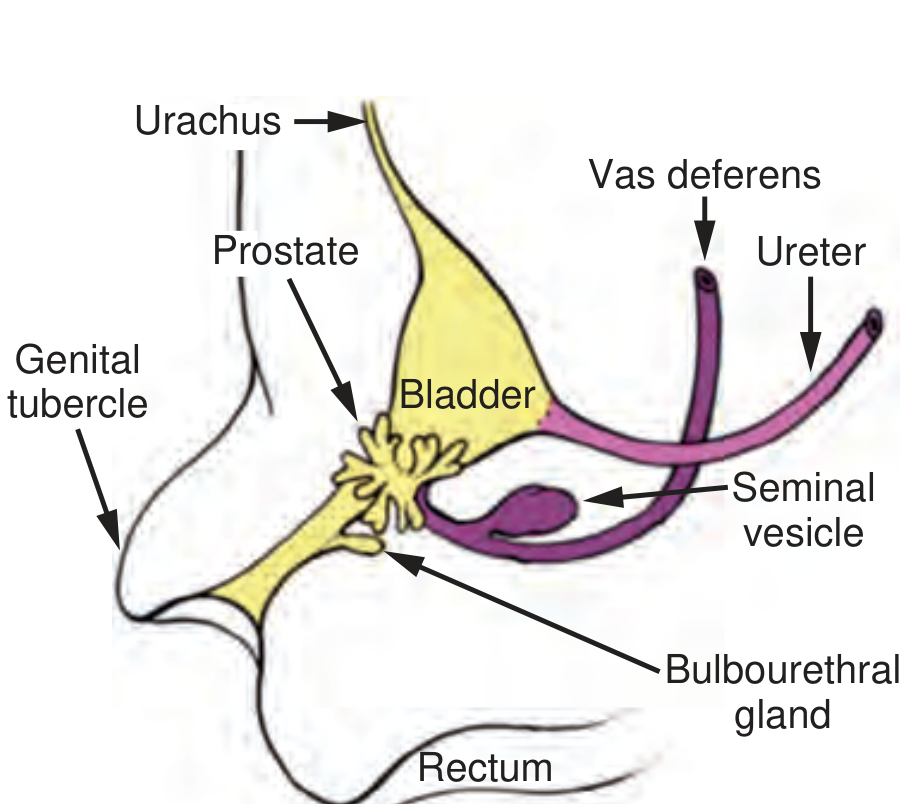
The developing male urogenital system. Structures in yellow (bladder, urachus, prostate, urethra, bulbourethral glands) are derived from endodermal urogenital sinus epithelium. The ureter, vas deferens, and seminal vesicle (purple) derive from mesodermal mesonephric (Wolffian) duct.
Verumontanum: A unique human feature - a craniocaudal hillock on the dorsal wall of the UGS. Most prostatic buds emerge from the gutters lateral to the verumontanum (weeks 9-10), establishing the spatial pattern of the mature prostate zones.
Zonal anatomy origin:
- Peripheral zone (70% of adult prostate, site of most cancers) - from lateral UGE buds
- Central zone (25%) - from periurethral UGE
- Transition zone (5%, site of BPH) - from periurethral region
Molecular Regulation of Prostate Development
Key signaling pathways in prostatic morphogenesis:
| Molecule | Role |
|---|---|
| DHT / AR | Primary androgen signal; acts through mesenchyme |
| FGF-7 (KGF), FGF-10 | Mesenchymal factors; stimulate epithelial growth |
| Wnt / β-catenin | Epithelial branching morphogenesis |
| Shh (Sonic hedgehog) | Regulates ductal branching pattern |
| BMP-4 | Inhibits lateral bud formation |
| FOXA1/2 | Endodermal transcription factors marking prostatic lineage |
| NKX3.1 | Early prostate-specific transcription factor; later a tumor suppressor |
Development of Seminal Vesicles
- Appear as a diverticulum of the Wolffian (mesonephric) duct at about weeks 10-12 of gestation
- The diverticulum elongates and folds back on itself to form a "hook-like duct" with extensive side ducts developing during months 4-5
- Autonomic innervation develops by week 13
- Malformations are extremely rare; seminal vesicle cysts can occur
CLINICAL CORRELATIONS OF PROSTATE DEVELOPMENT
1. Benign Prostatic Hyperplasia (BPH)
- Developmental significance: BPH represents a reactivation of prostatic developmental pathways - specifically re-awakening of the embryonic inductive interaction between stroma and epithelium (epithelial-mesenchymal interaction)
- Develops in the transition zone (same periurethral zone where prostatic buds first emerge)
- Androgen-dependent (testosterone/DHT) but also involves estrogen signaling
- Stroma-to-epithelium paracrine signaling mirrors fetal development
Clinicals:
- Lower urinary tract symptoms (LUTS): weak stream, hesitancy, frequency, nocturia, incomplete emptying
- Complications: acute urinary retention, hydronephrosis, bladder stones, recurrent UTI
- Treatment: alpha blockers (tamsulosin), 5α-reductase inhibitors (finasteride - blocks conversion of T to DHT), TURP
2. Prostate Cancer
- Most cancers arise in the peripheral zone
- PSA (prostate-specific antigen) is expressed throughout prostatic development and serves as a biomarker
- NKX3.1 - expressed early in prostate development as a lineage marker, later acts as a tumor suppressor; its loss is one of the earliest events in prostate carcinogenesis
- Reactivation of developmental programs (AR signaling, epithelial-mesenchymal transition) drives cancer progression
3. 5α-Reductase Deficiency
- Type 2 5α-reductase is expressed in the UGS during development
- Deficiency results in: normal Wolffian duct derivatives (testosterone-dependent), but markedly underdeveloped prostate, external genitalia feminization (pseudovaginal perineoscrotal hypospadias), and bifid scrotum
- Testes are present but undescended; AMH is normal so Müllerian structures are absent
- At puberty, rising testosterone drives virilization (voice deepening, muscle mass, phallus enlargement) - the classic "guevedoces" presentation
- Confirms the principle that DHT, not testosterone, is required for prostate and external genitalia formation
4. Androgen Insensitivity Syndrome (AIS)
- X-linked; AR gene mutations
- Complete AIS (CAIS): 46,XY; no functional AR; female external phenotype; absent uterus (AMH is normal); no prostate development; testes in inguinal canal or labia
- Partial AIS: variable phenotype depending on degree of AR dysfunction; rudimentary prostate may form
- AMH-mediated Müllerian regression is normal (not AR-dependent)
5. Hypospadias
- Failure of normal urethral plate canalization and/or urethral fold fusion
- In ~10% of severe cases, associated with DSD (differences of sex development)
- The prostatic urethra and prostate remain relatively unaffected; the penile/glandular urethra is the primary abnormality
- Associated with reduced androgen exposure or AR signaling defects in mild forms
6. Prostatitis Syndromes
- Embryological background relevant to understanding anatomy: the zonal structure of the prostate and its ductal drainage patterns determine which zones are most susceptible to inflammatory conditions
- Acute bacterial prostatitis - often involves the peripheral zone
- Chronic prostatitis/CPPS - may relate to abnormal ductal architecture from developmental variants
SUMMARY TABLE: Developmental Origins of Urogenital Structures
| Structure | Embryological Origin |
|---|---|
| Kidney (nephrons) | Metanephric blastema (intermediate mesoderm) |
| Ureter, renal pelvis, calyces | Ureteric bud (from mesonephric duct) |
| Bladder (mucosa) | Upper urogenital sinus (endoderm) |
| Bladder trigone | Mesonephric duct |
| Urethra (male, all parts) | Urogenital sinus epithelium (endoderm) |
| Prostate | Urogenital sinus epithelium (endoderm) - androgen-induced |
| Seminal vesicles | Mesonephric (Wolffian) duct |
| Epididymis, vas deferens | Mesonephric (Wolffian) duct |
| Efferent ductules | Mesonephric tubules |
| Uterus, fallopian tubes | Paramesonephric (Müllerian) ducts |
| Median umbilical ligament | Obliterated urachus (allantois) |
References:
- The Developing Human: Clinically Oriented Embryology (Moore et al.) - Chapter 12
- Campbell-Walsh-Wein Urology - Chapters 20 and 143 (Development of the Prostate)
This is a shared conversation. Sign in to Orris to start your own chat.