Breech/Transverse lie/FACE/BROW presentation theory ,clinical and treatment and management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed. Let me compile the comprehensive, structured answer.
Malpresentations in Obstetrics: Breech, Transverse Lie, Face & Brow
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Rosen's Emergency Medicine
RELATIVE INCIDENCE (Rosen's EM)
| Malpresentation | Incidence |
|---|---|
| Breech | 1/25 live births (~3-4%) |
| Shoulder (Transverse lie) | 1/300 live births |
| Face presentation | 1/550 live births |
| Brow presentation | 1/1400 live births |
I. BREECH PRESENTATION
Theory / Definition
Breech presentation = fetal buttocks or lower extremities present at the pelvic inlet. Incidence decreases with advancing gestation: 24% at 18-22 weeks → 8% at 28-30 weeks → 7% at 34 weeks → 2.8% at 38-40 weeks.
Types:
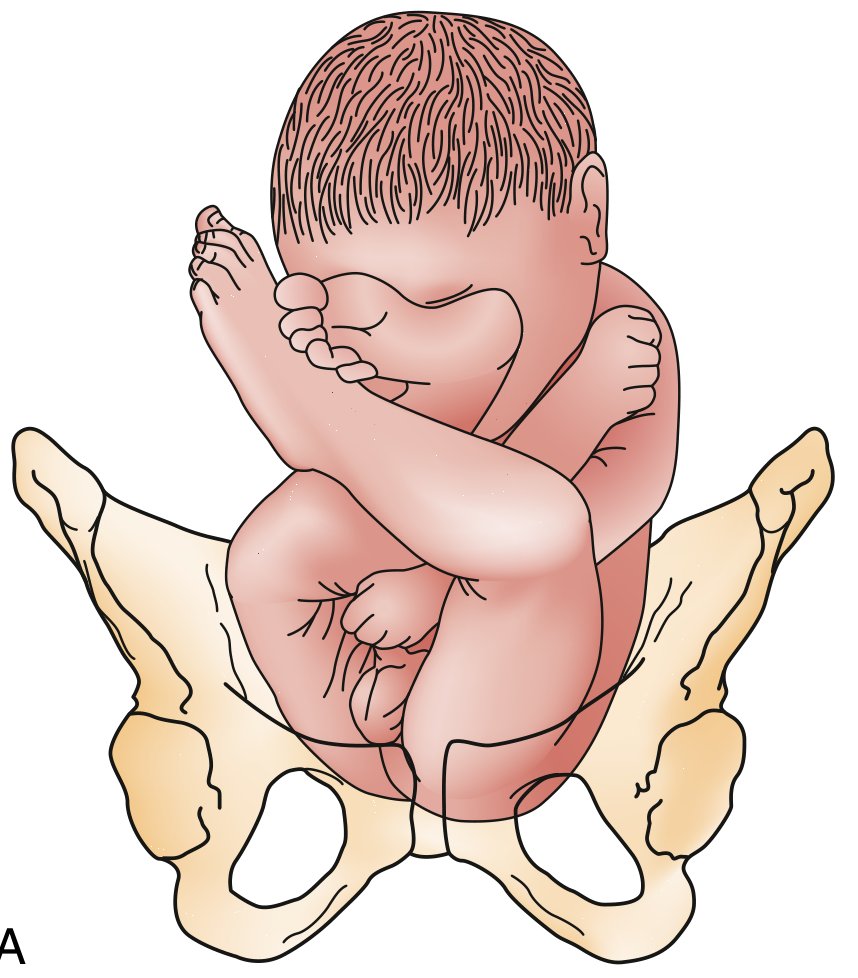
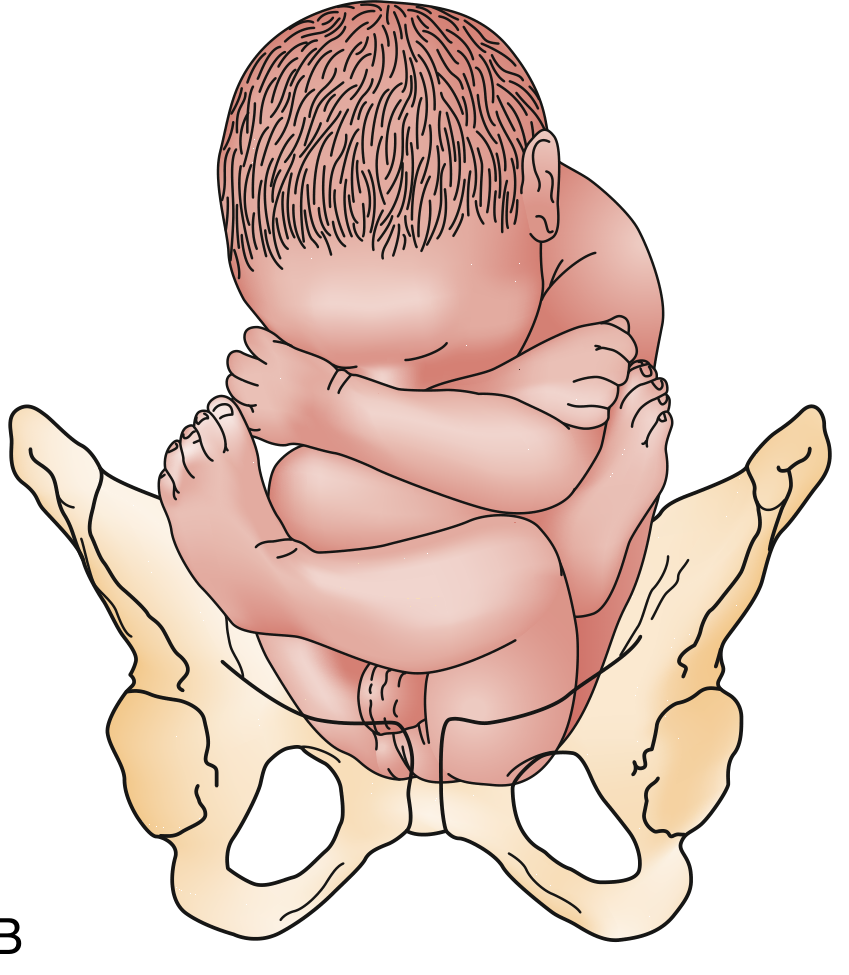
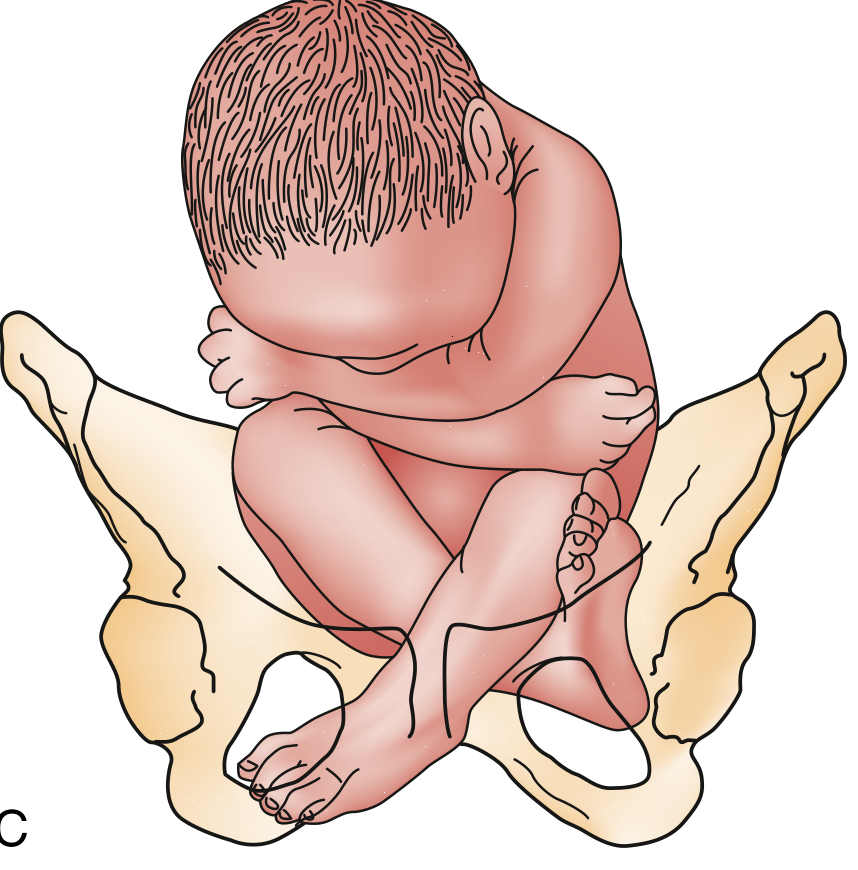
Reference point for position: Sacrum (e.g., sacrum anterior, sacrum posterior)
Etiology / Predisposing Factors
- Fundal-cornual placental implantation (occurs in 7% of pregnancies) - the fetus finds breech position more comfortable
- Prematurity
- Multiparity
- Fetal abnormalities / neuromuscular disorders (reduced fetal mobility)
- Polyhydramnios
- Uterine anomalies (bicornuate, fibroids)
- Prior breech presentation
- Multiple gestation
Note: Children born in breech scored less well on motor skills at age 5 regardless of delivery mode - suggesting some breech fetuses remain breech because of diminished neuromuscular ability.
Risks / Complications
- Umbilical cord prolapse - especially footling breech (presenting part does not fill the cervical os)
- Entrapment of the after-coming head by incompletely dilated cervix - particularly in preterm infants <1500 g
- Trauma from head extension or nuchal arm position
- Brachial plexus injury
- Asphyxia
- Significant variable decelerations in labor (umbilical cord in lower segment during late 1st and 2nd stage)
Diagnosis / Clinical Features
- Leopold maneuvers (before labor): hard, round, ballotable head in fundus; soft, irregular breech at the inlet; FHR heard at or above umbilicus
- Vaginal examination: softer, irregular presenting part; anus felt between two bony prominences (vs. vertex where you feel fontanelles/sutures in a complete bony circle)
- Key distinguishing tip: "the face and skull have a complete circle of bone, whereas the anus is flanked by bone on only two sides"
- If fontanel is not identified on vaginal exam, suspect breech
- Ultrasound (gold standard): confirms type, gestational age, fetal weight, arm/neck position, hyperextended neck (contraindication to vaginal delivery)
Management
A. Antepartum - External Cephalic Version (ECV)
When: Offered at 36-37 weeks with intact membranes, before labor onset
Contraindications to ECV:
- Uterine anomalies
- Third-trimester bleeding / placenta previa
- Multiple gestation
- Oligohydramnios
- Evidence of uteroplacental insufficiency
- Nuchal cord on USS
- Previous cesarean section or significant uterine surgery
- Obvious CPD
Procedure:
- Confirm reactive NST
- Administer tocolytic (terbutaline 0.25 mg SC) to relax uterus
- Attempt forward roll (or backward roll if unsuccessful)
- Monitor FHR intermittently with Doppler during procedure
- Fetal bradycardia occurs in ~20% but almost always resolves when manipulation stops
- Post-procedure FHR monitoring for 1 hour
- Rh-negative mothers: give 300 mcg Rh immune globulin (feto-maternal transfusion risk 6-28%)
Outcome: Reduces cesarean delivery risk by ~50% overall at 36 weeks
B. Mode of Delivery - Key ACOG Position
ACOG recommends: If ECV fails (or is not possible), planned cesarean delivery for term breech.
Criteria for a trial of vaginal breech delivery (selected cases only, with skilled obstetrician):
- Frank or complete breech (NOT footling)
- Estimated fetal weight 2000-3800 g
- Normal gynecoid pelvis with adequate measurements (AP inlet ≥11 cm, transverse inlet ≥12 cm, interspinous ≥9 cm)
- Flexed fetal head (hyperextended neck = contraindication)
Zatchuni Prognostic Index (Diagnostic Index for vaginal breech feasibility - scored on parity, gestational age, EFW, previous breech, cervical dilation, station): Score ≤3 = cesarean preferred.
C. Vaginal Breech Delivery Technique
- Allow buttocks/legs time to dilate cervix completely
- Do NOT pull on hips - this brings shoulders before the cervix is fully dilated, trapping the head
- Support but do not traction the presenting part
- Mauriceau maneuver for the after-coming head: insert finger into fetal mouth to flex the neck and flex chin onto chest, avoiding neck extension (associated with cord injuries)
- Only attempt once fetal elbows and chin have entered the pelvic inlet
- Support fetal pelvis to avoid abdominal injury
- Generous episiotomy may be needed
- Piper forceps can be applied to the after-coming head
- Fetal monitoring throughout (variable decels common); keep membranes intact as long as possible for hydraulic cord protection
D. Cesarean Section in Breech
- For most term breeches
- Uterine incision: low transverse usually adequate; low vertical or classical incision for transverse/back-down shoulder; Durfee high transverse incision is an option
II. TRANSVERSE LIE (Shoulder Presentation)
Theory / Definition
The fetal long axis is perpendicular to the maternal long axis. The shoulder is the presenting part. Incidence ~1/300 deliveries.
Shoulder presentation reference point: Acromion/scapula
Etiology
- Prematurity (38% of cases)
- High parity (87% had ≥3 prior deliveries)
- Premature rupture of membranes (30%)
- Placenta previa (10%)
- Uterine abnormalities
- Polyhydramnios
Risks
- Cord prolapse - potentially catastrophic (patient often arrives with asphyxiated/dead fetus)
- High perinatal mortality (3.9%-24%) - largely due to prevalence of low-birth-weight infants
- If labor progresses untreated with transverse lie: "neglected shoulder presentation" with uterine rupture risk
Diagnosis
- Palpation/Leopold: No fetal poles at fundus or inlet; fetal head felt laterally on one side, breech on the other
- Abdomen appears unusually wide transversely
- Patient may notice the abnormal position
- Ultrasound confirms diagnosis
Management
Decision framework based on gestational age + membrane status:
| Clinical Scenario | Management |
|---|---|
| <viable threshold (<600g) in labor | No intervention; may deliver vaginally (conduplicato corpore) without maternal harm |
| Viable fetus, membranes intact, no labor, <36 wks | Expectant - monitor for spontaneous version; avoid ECV before 36-37 wks (risk of cord entanglement, placental trauma) |
| Viable fetus, membranes intact, ≥36-37 wks, no labor | External version + induction at 38 wks (after excluding CPD and placenta previa); admit to hospital |
| Viable fetus, membranes RUPTURED or in active labor | Cesarean delivery mandatory |
| Placenta previa present | Cesarean delivery mandatory |
| CPD suspected | Cesarean delivery mandatory |
"Unstable lie" protocol (Edwards & Nicholson): Admit all patients ≥37 weeks with unstable lie. Exclude CPD/previa, attempt ECV, induce labor at ≥38 weeks. This policy reduced cord prolapse from 10/50 to 1/102 cases and eliminated perinatal deaths.
Cesarean uterine incision for transverse lie:
- Low transverse incision: usually adequate for "back-up" transverse lie
- Low vertical or classical incision: for "back-down" shoulder presentation
- Durfee high transverse incision: alternative option
III. FACE PRESENTATION
Theory / Definition
Maximum deflection of the cephalic presentation - the occiput extends to contact the fetal back, and the face (chin/mentum) becomes the presenting part.
Engaging diameter: Submento-bregmatic (~9.5 cm) - approximately 0.8 cm larger than vertex presentation.
Reference point for position: Mentum (chin) - e.g., Mentum Anterior (MA), Mentum Transverse (MT), Mentum Posterior (MP)
Frequency: ~1/500 deliveries (though likely higher if all presentations assessed early in labor)
Etiology
- CPD (cephalopelvic disproportion)
- Increased parity
- Prematurity
- Premature rupture of membranes
- Anencephaly - ALMOST ALWAYS results in face presentation (absent cranial vault allows maximum extension)
- Fetal anomalies otherwise do NOT account for most deflection problems
Clinical Features / Diagnosis
- Vaginal exam: Orbital ridges, nose, mouth, and chin felt - a complete bony ring around a soft central orifice (vs. anus in breech = bony on only 2 sides)
- Labor may be prolonged (Friedman found face presentation does NOT significantly affect labor course in nulliparas or multiparas - contrary to clinical impression)
- 50% of deflection diagnoses not made until 2nd stage of labor
- Diagnosis confirmed on ultrasound
Management
Guiding principle: "If a face presentation is progressing, leave it alone."
- Mentum anterior (MA): Usually delivers vaginally - mechanism is flexion of the head as it passes under the symphysis (chin leads)
- Mentum transverse (MT): Frequently rotates spontaneously to MA → vaginal delivery
- 70%-90% of face presentations result in spontaneous delivery
- Mentum posterior (MP, persistent): Cannot deliver vaginally at term (chin cannot flex past sacrum - the occiput would need to enter the pelvis which is too large) → Cesarean section mandatory
- Labor arrest with face presentation → Cesarean section
- Cord prolapse with face presentation → Cesarean section
- No attempts at manual conversion of face presentation
- Oxytocin augmentation may be used if labor is progressing and no CPD
IV. BROW PRESENTATION
Theory / Definition
Partial deflection of the cephalic presentation - intermediate between vertex and face. The frontal bone (between anterior fontanelle and supraorbital ridges) is the presenting part.
Engaging diameter: Mento-occipital (~13-14 cm) - the LARGEST diameter of the fetal head, approximately 1.5 cm larger than vertex. This is why brow presentation causes the most severe dystocia among head presentations.
Reference point: Frontum (forehead)
Frequency: ~1/1400 deliveries
Etiology
Same as face presentation:
- CPD
- Increased parity
- Prematurity
- PROM
- Fetal anomalies (rare)
Clinical Features / Diagnosis
- Vaginal exam: Anterior fontanelle + orbital ridges palpable; neither the occiput posteriorly nor the chin anteriorly can be felt
- If lambdoid sutures and posterior fontanelle cannot be identified centrally in the pelvis → suspect deflection problem
- Brow presentation associated with abnormalities of descent and longer second stage (unlike face presentation)
- Friedman: 10.9% of brow presentations had clinical + radiographic CPD vs. 2.7% of vertex controls
- Ultrasound confirms diagnosis
Management
Key principle: Most brow presentations convert spontaneously.
Decision pathway:
- Labor progressing + converting to face or vertex → manage expectantly for vaginal delivery
- Labor arrested + CPD suspected → Cesarean delivery
- Labor arrested + poor contractions + NO CPD → carefully monitored oxytocin augmentation ± radiographic pelvimetry to exclude CPD
- Brow fails to convert + fetus is term → Cesarean delivery (mento-occipital diameter too large to negotiate pelvis)
- For preterm/small infants: brow presentation is almost always unstable and converts spontaneously to occiput or face
Summary rule: "Successful descent in brow presentation at term depends on conversion to face or vertex." If this conversion does not occur → cesarean.
SUMMARY TABLE: Key Differentiating Points
| Feature | Breech | Transverse Lie | Face | Brow |
|---|---|---|---|---|
| Incidence | 3-4% | 1/300 | 1/550 | 1/1400 |
| Presenting part | Buttocks/feet | Shoulder | Chin | Forehead |
| Reference point | Sacrum | Acromion | Mentum | Frontum |
| Engaging diameter | Bitrocanteric | N/A | Submentobregmatic | Mento-occipital (largest) |
| Most common cause | Prematurity, fundal placenta | High parity, prematurity | CPD, anencephaly | CPD, prematurity |
| Key danger | Cord prolapse, head entrapment | Cord prolapse, neglected shoulder | MP cannot deliver | Largest engaging diameter |
| Spontaneous resolution | Rare after 36 wks | Variable | 70-90% deliver vaginally | >50% convert spontaneously |
| Primary management | ECV → CS if fails | CS if membranes ruptured/labor | Expectant if MA/MT; CS if MP | Expectant if converting; CS if not |
| Vaginal delivery possible? | Selected cases with criteria | Only in non-viable/very preterm | Yes, if MA or MT converts | Only if converts to vertex/face |
CARDINAL RULES TO REMEMBER
- Breech: Never pull - only support. Mauriceau maneuver for after-coming head.
- Transverse lie + ruptured membranes = cesarean. Admit all unstable lie patients ≥37 weeks.
- Face presentation: Mentum anterior = go; Mentum posterior = cesarean.
- Brow presentation: The largest engaging diameter. Almost always needs to convert or → cesarean at term.
- Cord prolapse complicates all malpresentations and is an absolute indication for emergency cesarean.
- ECV (contraindications: placenta previa, ruptured membranes, oligohydramnios, previous uterine surgery, multiple gestation, cord around neck, CPD).
- Creasy & Resnik's Maternal-Fetal Medicine, pp. 953-958 | Rosen's Emergency Medicine, pp. 3415-3418
This is a shared conversation. Sign in to Orris to start your own chat.