Ace inhibitors
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ACE inhibitors" AND "heart failure"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of ACE inhibitors, drawn from authoritative pharmacology textbooks.
ACE Inhibitors (Angiotensin-Converting Enzyme Inhibitors)
Mechanism of Action
ACE inhibitors block the enzyme angiotensin-converting enzyme (ACE), which normally cleaves angiotensin I (inactive) into angiotensin II (potent vasoconstrictor). ACE is also responsible for the breakdown of bradykinin - a peptide that stimulates the production of nitric oxide and prostacyclin (both vasodilators).
The net result:
- Decreased angiotensin II → less vasoconstriction, less aldosterone secretion
- Increased bradykinin → enhanced vasodilation, nitric oxide release
- Decreased aldosterone → reduced Na⁺ and water retention → decreased preload
- Efferent arteriolar dilation → reduced intraglomerular pressure → renoprotection
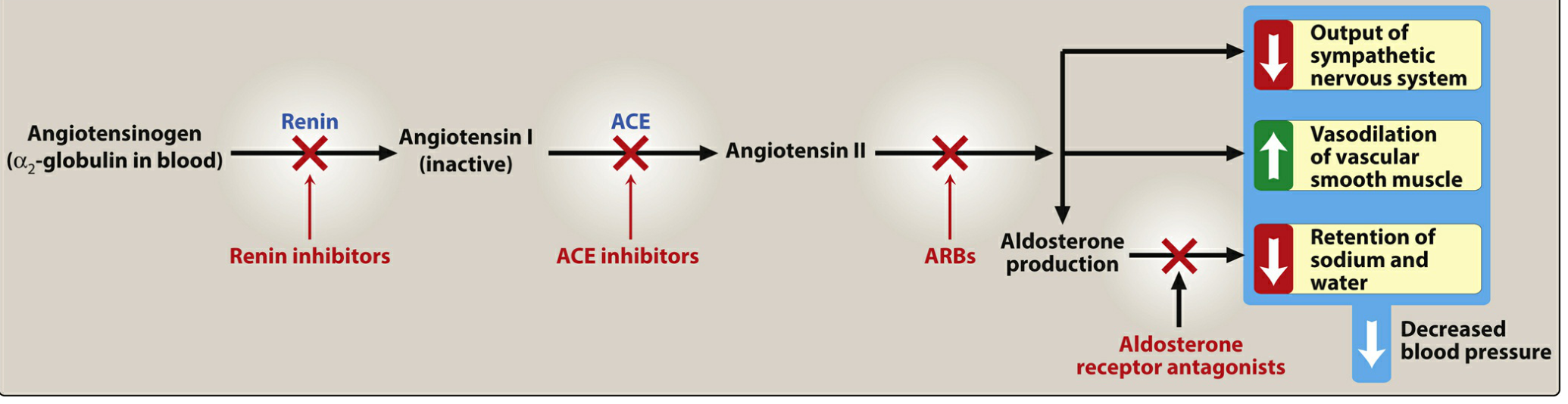
Figure: The renin-angiotensin-aldosterone system (RAAS) and the sites of action of renin inhibitors, ACE inhibitors, ARBs, and aldosterone antagonists. - Lippincott Illustrated Reviews: Pharmacology
Drugs in This Class
| Generic Name | Brand Name |
|---|---|
| Captopril | Generic only |
| Enalapril | Vasotec |
| Lisinopril | Prinivil, Zestril |
| Ramipril | Altace |
| Quinapril | Accupril |
| Fosinopril | Generic only |
| Benazepril | Lotensin |
| Perindopril | Generic only |
| Trandolapril | Generic only |
| Enalaprilat | IV form only |
Therapeutic Uses
ACE inhibitors are a first-line drug class for multiple conditions:
- Hypertension - all agents equally effective at equivalent doses
- Heart failure with reduced ejection fraction (HFrEF) - reduce preload and afterload, improve ventricular remodeling
- Post-myocardial infarction - standard of care; improve ventricular remodeling
- Diabetic nephropathy - slow progression, reduce albuminuria; preferred in diabetics with proteinuria
- Chronic kidney disease - first-line for hypertensive CKD patients
- Coronary artery disease - reduce risk in high-risk patients
"ACE inhibitors are first-line drugs for treating heart failure, hypertensive patients with chronic kidney disease, and patients at increased risk of coronary artery disease." - Lippincott Illustrated Reviews: Pharmacology
Pharmacokinetics
- All ACE inhibitors are orally bioavailable as drug or prodrug
- Most (except captopril and lisinopril) require hepatic conversion to active metabolites - captopril and lisinopril are preferred in severe hepatic impairment
- Fosinopril is the only ACE inhibitor with dual renal/hepatic elimination - does NOT require dose adjustment in renal impairment
- Enalaprilat is the only IV formulation available
Adverse Effects
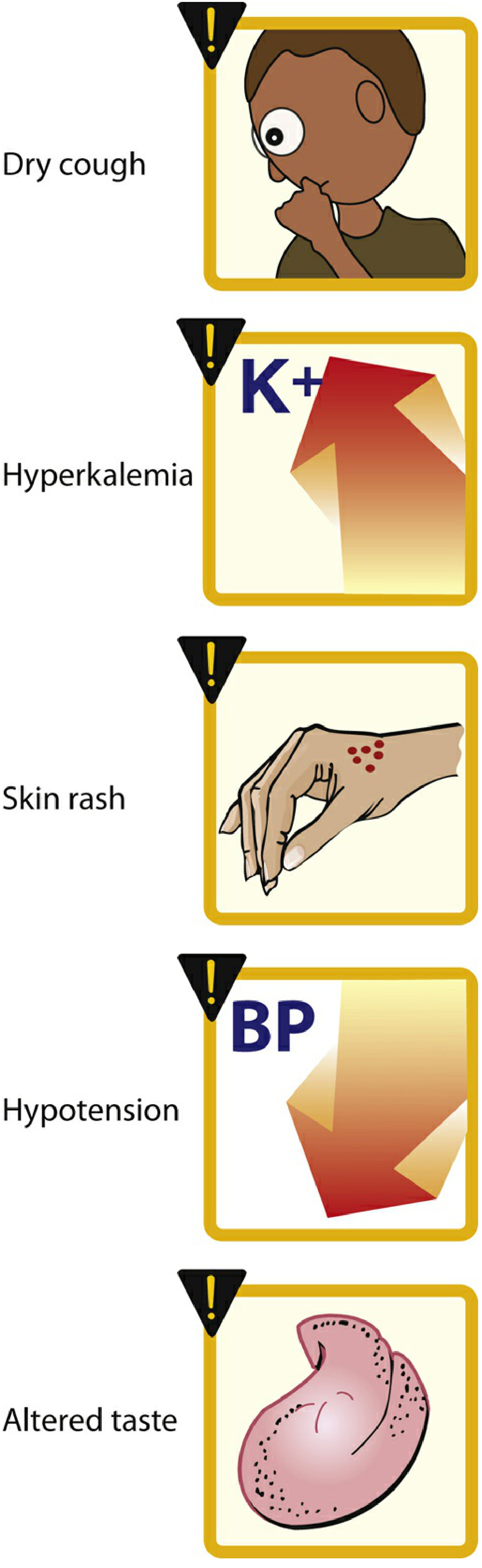
Figure: Common adverse effects of ACE inhibitors - Lippincott Illustrated Reviews: Pharmacology
| Adverse Effect | Mechanism | Notes |
|---|---|---|
| Dry cough | Accumulation of bradykinin and substance P in the pulmonary tree | Occurs in ~10% of patients; more common in women; resolves on discontinuation |
| Angioedema | Increased bradykinin → swelling of lips, oral mucosa, throat | Rare but life-threatening; 5x more frequent in people of African ancestry |
| Hyperkalemia | Decreased aldosterone → reduced K⁺ excretion | Monitor K⁺; avoid K⁺ supplements/K⁺-sparing diuretics |
| Hypotension | Vasodilation; first-dose effect | Especially in volume-depleted patients |
| Elevated creatinine | Reduced efferent arteriolar tone | Rise of up to 30% above baseline is acceptable and not a reason to stop |
| Skin rash / altered taste | Captopril-related (sulfhydryl group) | Less common with newer agents |
| Teratogenicity | Fetal renal hypoperfusion | Contraindicated in pregnancy |
Contraindications
- Pregnancy (category D in 2nd/3rd trimester - causes fetal renal dysgenesis, oligohydramnios, skull hypoplasia)
- Bilateral renal artery stenosis (can precipitate acute renal failure)
- History of angioedema with any ACE inhibitor
- Hyperkalemia (K⁺ >5.5 mEq/L)
- Concurrent use with aliskiren in diabetics or CKD patients
Drug Interactions
- Potassium-sparing diuretics / K⁺ supplements → hyperkalemia
- NSAIDs → blunted antihypertensive effect, increased nephrotoxicity
- Lithium → ACE inhibitors increase lithium levels (reduced renal clearance)
- ARBs → combination not recommended (increased adverse effects without added benefit)
- Aliskiren → combination contraindicated in DM or CKD
ACE Inhibitors vs ARBs - Key Distinction
ARBs block the AT₁ receptor directly and do not increase bradykinin levels, which is why:
- ARBs have a much lower incidence of cough (~1-2% vs ~10%)
- ARBs have lower risk of angioedema (though not zero, since AT₂-mediated bradykinin also rises)
- ARBs are the preferred alternative when ACE inhibitors cause intolerable cough
"Bradykinin contributes to many of the protective effects of ACE inhibitors... A rare side effect of ACE inhibitors is angioedema, which is likely due to the inhibition of kinin metabolism." - Goodman & Gilman's Pharmacological Basis of Therapeutics
Sources:
- Lippincott Illustrated Reviews: Pharmacology, Chapter 8 (Antihypertensives)
- Goodman & Gilman's Pharmacological Basis of Therapeutics, Chapter 43 (Kinins)
This is a shared conversation. Sign in to Orris to start your own chat.