Oral hypoglycaemic agent
Reading File
Finding Sources
Finding Sources
Searching PubMed
"oral hypoglycemic agents" AND "type 2 diabetes"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have excellent, comprehensive content from both Katzung's Pharmacology and Lippincott's Pharmacology. I have enough to deliver a thorough, well-organized answer covering all major classes of oral hypoglycaemic agents.
Oral Hypoglycaemic Agents
Oral hypoglycaemic agents (OHAs) are drugs taken by mouth to lower blood glucose in type 2 diabetes mellitus. They are categorized based on their primary mechanism: insulin secretagogues, insulin sensitizers, glucose absorption inhibitors, glucose excretion enhancers, and incretin-based agents.
1. Sulfonylureas (Insulin Secretagogues)
Mechanism: Bind to a 140-kDa sulfonylurea receptor associated with an ATP-sensitive K⁺ channel (K-ATP channel) on pancreatic beta cells. Channel blockade causes membrane depolarization → voltage-gated Ca²⁺ channel opens → Ca²⁺ influx → insulin exocytosis. They are effective only if functioning beta cells remain (ineffective in Type 1 DM or after pancreatectomy).
First Generation
| Drug | Half-life | Duration | Key Feature |
|---|---|---|---|
| Tolbutamide | 4-5 h | 6-10 h | Safe in elderly/renal impairment; max 3000 mg/day |
| Tolazamide | - | Intermediate | Less potent |
| Chlorpropamide | ~36 h | Up to 60 h | Causes SIADH; avoid in elderly |
Second Generation (higher receptor affinity, lower doses)
| Drug | Dose | Key Feature |
|---|---|---|
| Glipizide | 2.5-40 mg/day | Short-acting; renal-safe |
| Glyburide (glibenclamide) | 1.25-20 mg/day | Active metabolites; risk in renal failure |
| Glimepiride | 1-8 mg/day | Once daily; fewest interactions |
Adverse effects: Hypoglycaemia (main risk), weight gain, skin rashes, rarely haematologic toxicity (leukopenia, thrombocytopenia <0.1%). Metabolized by the liver; metabolites excreted renally (or partly in bile for 2nd generation).
The UKPDS (UK Prospective Diabetes Study) found no excess cardiovascular mortality with sulfonylureas.
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
2. Biguanides (Insulin Sensitizer - Hepatic)
Drug: Metformin (only biguanide in current clinical use)
Mechanism: Activates hepatic AMP-activated protein kinase (AMPK), which:
- Reduces hepatic gluconeogenesis and glycogenolysis
- Reduces hepatic lipogenesis
- Does NOT stimulate insulin release - no hyperinsulinaemia, no hypoglycaemia as monotherapy
Pharmacokinetics:
- Half-life: 1.5-3 hours; not protein bound; excreted unchanged in urine
- Not metabolized hepatically
- eGFR ≥60: safe; eGFR 30-45: use cautiously; eGFR <30: contraindicated
Dosing: Start 500 mg daily with food, titrate to 1000 mg twice daily; max benefit at 2000 mg/day.
Adverse effects:
- GI (nausea, diarrhoea, abdominal discomfort) in ~20% - dose-related, often transient; extended-release formulation reduces this
- Lactic acidosis (rare) - risk increased in renal/hepatic failure, tissue hypoxia
- Vitamin B12 malabsorption (long-term use) - due to impaired calcium-dependent ileal absorption of B12-intrinsic factor complex; monitor periodically
Benefits beyond glucose lowering:
-
UKPDS: metformin reduced cardiovascular and microvascular events in obese Type 2 diabetics
-
Diabetes Prevention Program: metformin prevents new-onset Type 2 DM in obese patients with impaired glucose tolerance
-
Possible reduction in cancer risk (epidemiological data)
-
Katzung's Basic and Clinical Pharmacology, 16th Ed.
3. Meglitinides (Short-Acting Insulin Secretagogues)
Drugs: Repaglinide, Nateglinide
Mechanism: Similar to sulfonylureas - close K-ATP channels on beta cells → depolarization → insulin release. However, they have a rapid onset and shorter duration making them "postprandial glucose regulators." Taken before each meal.
Metabolism:
- Nateglinide: CYP2C9 and CYP3A4; metabolites excreted in urine
- Repaglinide: CYP2C8 and CYP3A4; excreted in feces - safer in renal disease
Adverse effects: Hypoglycaemia and weight gain (less than sulfonylureas). Gemfibrozil markedly increases repaglinide levels (CYP2C8 inhibition) - concurrent use contraindicated. Do NOT combine with sulfonylureas (overlapping mechanism + severe hypoglycaemia risk).
- Lippincott Illustrated Reviews: Pharmacology
4. Thiazolidinediones / TZDs (Insulin Sensitizers - Peripheral)
Drugs: Pioglitazone, Rosiglitazone
Mechanism: Agonists at PPARγ (peroxisome proliferator-activated receptor gamma), a nuclear hormone receptor. PPARγ activation upregulates transcription of insulin-responsive genes → increased insulin sensitivity in adipose tissue, liver, and skeletal muscle. Require insulin to act but do NOT promote its release.
Pharmacokinetics: Well absorbed orally, extensively bound to serum albumin, metabolized by CYP2C8. Pioglitazone: mainly biliary/fecal excretion. Rosiglitazone: mainly renal. No dose adjustment needed for renal impairment.
Adverse effects:
-
Weight gain (increased subcutaneous fat) and fluid retention
-
Heart failure exacerbation - avoid in symptomatic heart failure
-
Osteopenia and increased fracture risk in women
-
Pioglitazone: possible increased bladder cancer risk
-
Rosiglitazone: boxed warning - possible increased risk of MI and angina
-
Hepatotoxicity (rare) - monitor LFTs
-
Lippincott Illustrated Reviews: Pharmacology
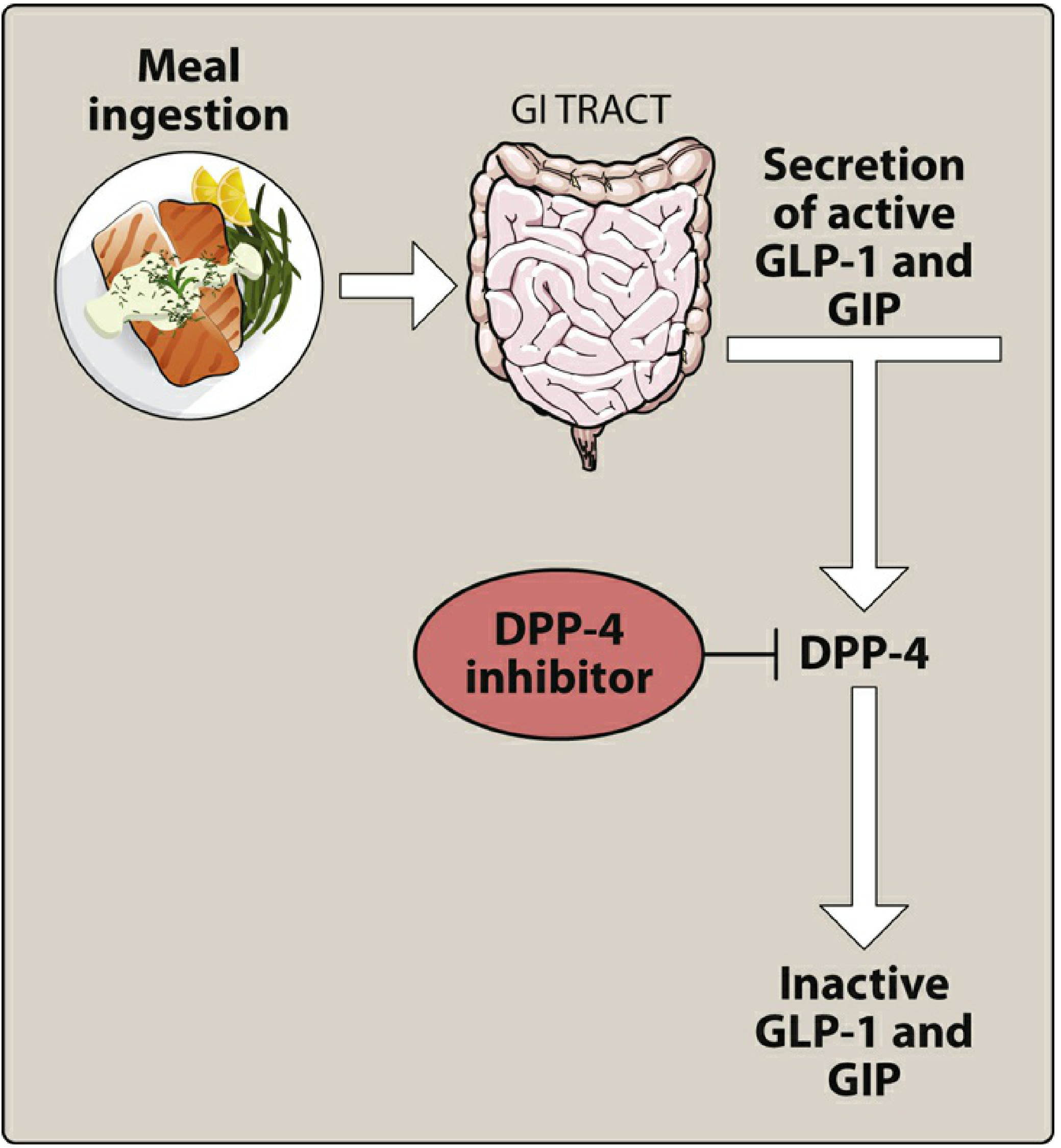
5. DPP-4 Inhibitors ("Gliptins") - Incretin Enhancers
Drugs: Sitagliptin, Saxagliptin, Linagliptin, Alogliptin, Vildagliptin
Mechanism: Inhibit DPP-4 (dipeptidyl peptidase-4), the enzyme that rapidly degrades incretin hormones (GLP-1 and GIP). This prolongs incretin activity, increasing glucose-dependent insulin secretion and suppressing glucagon - only when glucose is elevated (glucose-dependent effect, so low hypoglycaemia risk as monotherapy).
Key pharmacokinetic notes:
- All except linagliptin require dose reduction in renal impairment
- Linagliptin: primarily eliminated via enterohepatic system - no renal dose adjustment needed
- Saxagliptin: active metabolite; metabolized by CYP3A4/5
Adverse effects:
- Generally well tolerated; nasopharyngitis and headache most common
- Rare: serious hypersensitivity (anaphylaxis, angioedema, Stevens-Johnson syndrome), pancreatitis
- Severe disabling joint pain (rare - FDA warning)
- Saxagliptin and alogliptin: increased risk of heart failure hospitalization - use with caution
HbA1c reduction: ~0.5-1.0%
- Katzung's Basic and Clinical Pharmacology, 16th Ed.; Lippincott Illustrated Reviews: Pharmacology
6. GLP-1 Receptor Agonists (Incretin Mimetics)
Drugs: Semaglutide (oral and injectable), Liraglutide, Dulaglutide, Exenatide, Lixisenatide
Mechanism: Mimic endogenous GLP-1 (glucagon-like peptide-1):
- Glucose-dependent insulin secretion
- Suppress postprandial glucagon
- Slow gastric emptying → reduced postprandial hyperglycaemia
- Central satiety enhancement → weight loss
- Promote beta-cell proliferation
Incretin hormones account for 60-70% of postprandial insulin secretion. This "incretin effect" is markedly reduced in Type 2 diabetes.
Administration: Most are subcutaneous injections (not oral - polypeptides). Exception: oral semaglutide (Rybelsus) is the only oral GLP-1 agonist.
Cardiovascular benefits: Dulaglutide, liraglutide, and semaglutide are approved to reduce cardiovascular mortality, MI, and stroke in Type 2 DM with established cardiovascular disease.
Adverse effects: Nausea, vomiting, diarrhoea (common, especially on initiation), pancreatitis (rare), injection site reactions.
- Lippincott Illustrated Reviews: Pharmacology
7. SGLT2 Inhibitors ("Gliflozins") - Glucose Excretion Enhancers
Drugs: Empagliflozin, Dapagliflozin, Canagliflozin, Ertugliflozin
Mechanism: Inhibit sodium-glucose cotransporter 2 (SGLT2) in the proximal renal tubule, which normally reabsorbs ~90% of filtered glucose. Inhibition causes glucosuria (glucose excretion in urine) → blood glucose lowering, independent of insulin.
Additional benefits:
- Osmotic diuresis and natriuresis → blood pressure reduction
- Weight loss
- Reduced cardiovascular mortality (empagliflozin, canagliflozin)
- Reduce heart failure hospitalization (empagliflozin, dapagliflozin - also approved for HFrEF regardless of DM status)
- Slow progression of diabetic kidney disease
Adverse effects:
-
Genital mycotic infections (glucosuria promotes fungal growth) - most common
-
Urinary tract infections
-
Euglycaemic DKA (rare but serious)
-
Canagliflozin: increased risk of lower limb amputation (FDA warning), bone fractures
-
Volume depletion/hypotension (especially with diuretics)
-
Katzung's Basic and Clinical Pharmacology, 16th Ed.; Lippincott Illustrated Reviews: Pharmacology
8. Alpha-Glucosidase Inhibitors
Drugs: Acarbose, Miglitol
Mechanism: Competitively inhibit intestinal alpha-glucosidases (enzymes that break down complex carbohydrates in the brush border), delaying glucose absorption from the gut → reduces postprandial hyperglycaemia.
Adverse effects: Flatulence, bloating, diarrhoea (due to unabsorbed carbohydrates fermenting in the colon). Must be taken with the first bite of a meal.
Summary Comparison Table
| Class | Example(s) | Mechanism | Hypoglycaemia Risk | Weight Effect | Key Concern |
|---|---|---|---|---|---|
| Sulfonylureas | Glipizide, Glimepiride | K-ATP channel closure → insulin release | High | Gain | Hypoglycaemia |
| Biguanides | Metformin | ↓ Hepatic gluconeogenesis (AMPK) | None | Neutral/loss | Lactic acidosis (rare); B12 deficiency |
| Meglitinides | Repaglinide | K-ATP closure (short-acting) | Moderate | Gain | Hypoglycaemia (less than SU) |
| TZDs | Pioglitazone | PPARγ agonist → insulin sensitivity | None | Gain | Heart failure, fractures |
| DPP-4 inhibitors | Sitagliptin, Linagliptin | Prolong GLP-1/GIP activity | Low | Neutral | Pancreatitis, joint pain |
| GLP-1 agonists | Semaglutide, Liraglutide | GLP-1 receptor activation | Low | Loss | Nausea/vomiting; pancreatitis (rare) |
| SGLT2 inhibitors | Empagliflozin, Dapagliflozin | Urinary glucose excretion | None | Loss | Genital infections, DKA (rare) |
| Alpha-glucosidase inhibitors | Acarbose | ↓ Carbohydrate absorption | None | Neutral | GI flatulence |
Clinical Notes
- Metformin remains the first-line agent for Type 2 DM (unless contraindicated) per most guidelines.
- In patients with established cardiovascular disease or heart failure, SGLT2 inhibitors or GLP-1 agonists with proven CV benefit are preferred add-on agents.
- DPP-4 inhibitors + GLP-1 agonists should not be combined (overlapping mechanism, increased toxicity risk).
- Meglitinides + sulfonylureas should not be combined (overlapping mechanism, severe hypoglycaemia).
- Metformin is also used for prevention of Type 2 DM in high-risk individuals (impaired glucose tolerance, obesity).
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Lippincott Illustrated Reviews: Pharmacology; Ganong's Review of Medical Physiology, 26th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.