Explain the bronchial asthma
In Practice of medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"bronchial asthma" AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content from both Harrison's Principles of Internal Medicine (22nd Ed, 2025) and Goldman-Cecil Medicine. Here is a detailed, well-structured explanation:
Bronchial Asthma
Definition
Asthma is a clinical syndrome of unknown etiology characterized by recurrent episodes of airway obstruction that resolve spontaneously or as a result of treatment. These changes occur in the setting of various types of airway inflammation thought to reflect specific endotypes. Although airway obstruction is largely reversible, some changes leading to obstruction may become irreversible over time.
- Goldman-Cecil Medicine, p. 879
Epidemiology
-
Affects approximately 8% of the adult US population and an estimated 340 million people worldwide, with ~420,000 annual deaths
-
More common in boys than girls before puberty; after puberty, women > men (rate ratio ~1.8:1)
-
Most cases begin before age 25, but new-onset asthma can develop at any age
-
Worldwide prevalence increased >50% in the latter half of the 20th century, particularly in countries adopting industrialized lifestyles; prevalence has plateaued since ~2015
-
Growing up on a farm in close contact with cattle is associated with a markedly lower risk
-
Goldman-Cecil Medicine, p. 880
Pathobiology
Genetics
Asthma has about 60% heritability (twin studies). Multiple genome-wide association studies have identified genetic loci related to immune mechanisms, confirming that both genetic and environmental factors play a role.
Pathology and Endotypes
The asthma syndrome shows marked heterogeneity. Classically, two forms were recognized (atopic and non-atopic), but this is an oversimplification. Multiple endotypes underlie the common signs and symptoms:
1. Atopic (Allergic) Asthma - the most common subtype
- IgE-mediated sensitization to environmental allergens
- Present in almost all school-aged children with asthma and ~50% of adult asthmatics
- Pathologic features: airway inflammation and remodeling - epithelial fragility, edema, mucosal hyperemia, subepithelial reticular basement thickening (collagen III and IV deposition)
- In severe/chronic disease: airway wall thickening from smooth muscle hyperplasia, mucus gland hypertrophy, and subepithelial angiogenesis
- Inflammatory infiltrate: eosinophils, CD4+ T-lymphocytes, mast cells, macrophages
- IgE-coated mast cells in the airway epithelium and lumen are hallmarks
2. Non-Atopic (Non-Allergic) Asthma
- Triggered by irritants, pollutants, microbes, viruses
- Driven by neutrophilic inflammation, Th1 and Th17 cells
- Mediated by IL-6, IL-17, TNF-alpha, IL-1beta, IL-8
3. Pauci-Granulocytic Asthma
- A small subset with pathologic changes but no tissue infiltration by inflammatory cells; etiology unclear
Pathophysiology
Mechanisms of Airway Obstruction
Three major processes can occur individually or simultaneously:
1. Airway Hyperresponsiveness
The hallmark of asthma. Defined as an exaggerated narrowing response to agents that cause no response in unaffected individuals. Occurs at the level of airway smooth muscle (shown by hyperresponsiveness to histamine or methacholine). It can also arise from indirect activation of inflammatory cells that release bronchoconstricting mediators.
2. Airway Inflammation
- Type 2 (T2-high) inflammation: driven by allergens activating dendritic cells → Th2 cells and ILC2 cells → release of IL-4, IL-5, IL-13 → eosinophil recruitment, IgE production, mast cell activation → bronchoconstriction, mucus secretion, airway remodeling
- Non-Type 2 (T2-low) inflammation: triggered by irritants, pollutants, viruses → Th1/Th17 cells, neutrophilic inflammation → IL-17, IL-6, IL-8 → smooth-muscle constriction
3. Airway Remodeling
Chronic inflammation leads to structural changes: subepithelial fibrosis, smooth-muscle hypertrophy/hyperplasia, goblet cell hyperplasia (excess mucus), and angiogenesis.
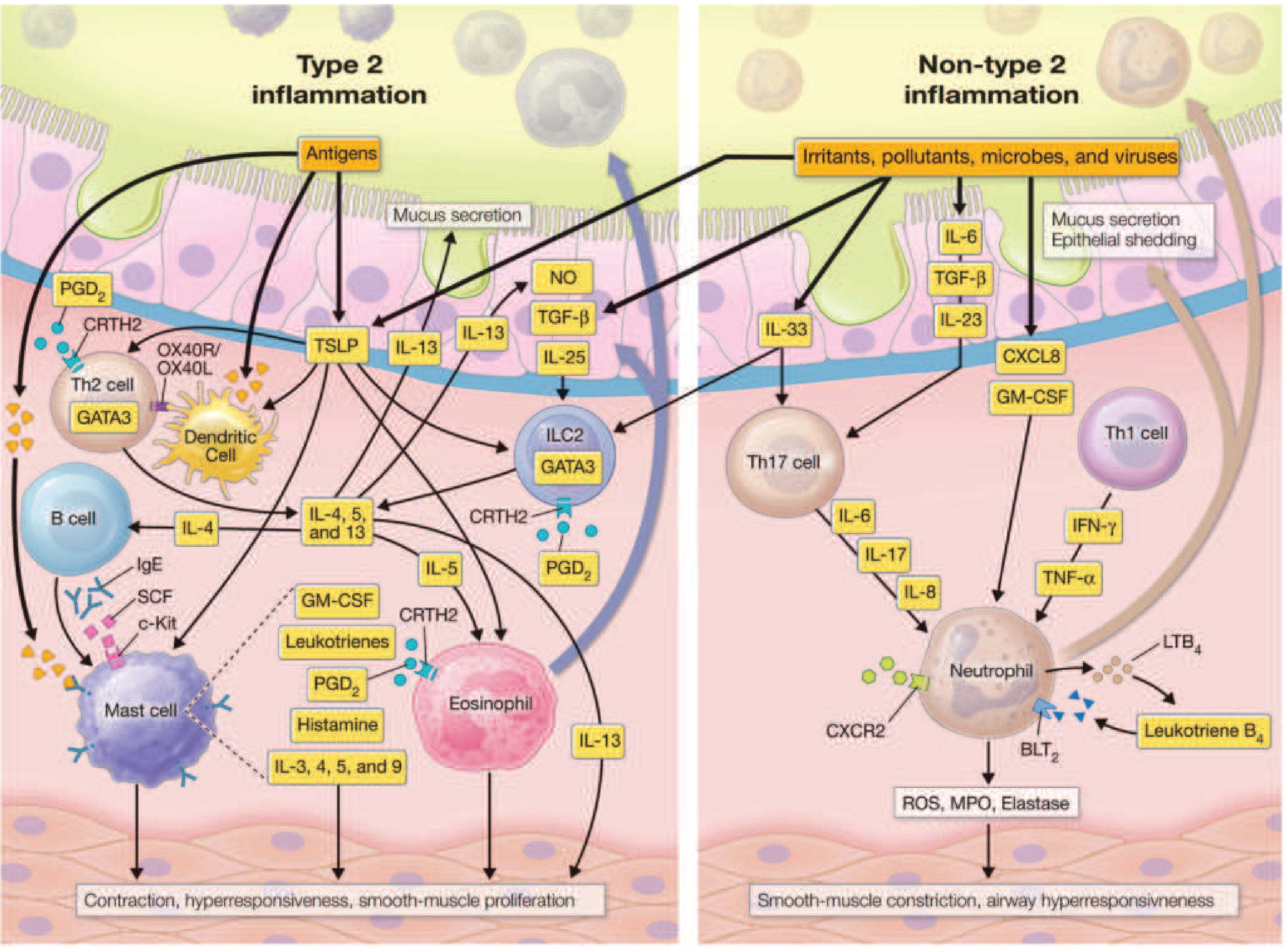
Key Mediators
| Mediator | Source | Effect |
|---|---|---|
| IL-4, IL-5, IL-13 | Th2 cells, ILC2 | Core T2 cytokines; IgE switching, eosinophil recruitment, mucus |
| TSLP, IL-25, IL-33 | Airway epithelium | Alarm signals (alarmins); amplify T2 cascade |
| Cysteinyl leukotrienes (LTC4, LTD4, LTE4) | Eosinophils, mast cells | Potent smooth-muscle constrictors, mucus secretion, microvascular leakage |
| Histamine | Mast cells | Bronchoconstriction, vasodilation |
| PGD2 | Mast cells | Activates CRTH2 receptors on T2/ILC2/eosinophil cells; upregulates T2 inflammation |
| LTB4 | Neutrophils | Neutrophil chemoattractant |
| TNF-alpha, IL-6, IL-17, IL-8 | Neutrophils, macrophages | Non-T2 inflammation |
- Harrison's 22E, p. 2262
Risk Factors and Triggers
Development Risk Factors:
- Allergen exposure in atopic individuals
- Occupational exposures
- Air pollution
- Viral and Mycoplasma infections
- Tobacco smoke
- Obesity
- Diet
- Fungi (allergic airway mycoses)
- Reactive airway dysfunction syndrome (RADS)
- High-intensity exercise in elite athletes
Triggers of Acute Airway Narrowing:
- Allergens
- Irritants
- Viral infections (most common cause of exacerbations)
- Exercise and cold, dry air
- Air pollution
- Drugs (NSAIDs, aspirin, beta-blockers)
- Occupational exposures
- Hormonal changes
- Pregnancy
Clinical Features
Symptoms:
- Episodic wheezing, particularly expiratory
- Dyspnea (breathlessness)
- Chest tightness
- Cough (dry or productive), especially at night or early morning
- Symptoms often worse at night (nocturnal asthma)
Signs:
- Prolonged expiration and wheeze on auscultation
- Use of accessory muscles in severe attacks
- Pulsus paradoxus in severe/life-threatening attacks
- Cyanosis (late, ominous sign)
Investigations
Pulmonary Function Tests (PFTs) - cornerstone of diagnosis:
- Obstructive pattern: reduced FEV1, reduced FEV1/FVC ratio
- Reversibility: ≥12% and ≥200 mL improvement in FEV1 after bronchodilator - confirms diagnosis
- Methacholine challenge test: positive (PC20 ≤8 mg/mL) if PFTs normal but asthma suspected
Blood Findings:
- Eosinophilia (common in T2-high phenotype)
- Elevated serum IgE (total and specific IgE via RAST)
- FeNO (fractional exhaled nitric oxide): elevated in eosinophilic/T2-high asthma; used to guide treatment
Radiology:
- Chest X-ray usually normal
- Severe asthma: hyperinflation (depressed diaphragm, lucent lung fields)
- Complications: pneumomediastinum, subcutaneous emphysema, pneumothorax may be seen
Arterial Blood Gas (ABG) in Acute Severe Asthma:
- Initially: hypoxemia (PaO2 55-70 mmHg) + hypocapnia (PaCO2 25-35 mmHg) + respiratory alkalosis
- As severity worsens: PaCO2 normalizes or rises - ominous sign indicating impending respiratory failure
- A "normal" PaCO2 in a patient with several days of severe airflow obstruction signals that respiratory failure may be imminent
Sputum:
- May be clear or colored (color does not always indicate infection)
- Microscopy: eosinophils, Charcot-Leyden crystals, Curschmann spirals
ECG:
-
Usually normal (sinus tachycardia) in mild/moderate attacks
-
Severe attacks: right axis deviation, right bundle branch block, "P pulmonale", ST-T changes (resolve with treatment)
-
Goldman-Cecil Medicine, p. 882-884
Treatment
Goals of Therapy (GINA/NAEPP)
- Reduction of symptoms to ≤2 times/week
- Nighttime awakenings ≤2 times/month
- Reliever use ≤2 times/week (except pre-exercise)
- No more than 1 exacerbation/year
- Optimization of lung function (FEV1/PEF)
- Maintenance of normal daily activities
- Minimal or no medication side effects
Non-Pharmacological Measures
- Trigger avoidance: remove pets, pest control, impermeable mattress covers for dust mites, smoking cessation
- Allergen immunotherapy: reduces IgE-mediated reactions; effective for mild-moderate allergic asthma under control
- Vaccination: annual influenza, pneumococcal (all adult asthmatics), COVID-19, RSV vaccines
- Treat comorbidities: allergic rhinitis, GERD, obesity, obstructive sleep apnea
Pharmacotherapy
Reliever (Rescue) Medications
Short-Acting Beta-2 Agonists (SABAs)
- Salbutamol (albuterol), terbutaline
- Onset 5-10 min, duration 4-8 hours
- First-line for acute symptom relief; all patients should have a SABA rescue inhaler
Short-Acting Anticholinergics
- Ipratropium bromide - used in acute exacerbations, especially in combination with SABAs
Systemic Corticosteroids (acute severe attacks)
- IV hydrocortisone 2 mg/kg bolus then 0.5 mg/kg/hr for non-life-threatening severe exacerbations
- IV methylprednisolone 125 mg every 6 hours for life-threatening exacerbations
- Oral prednisolone for outpatient step-up; taper over 1-3 weeks
Controller (Preventive) Medications
Inhaled Corticosteroids (ICS) - cornerstone of preventive therapy
- Beclomethasone, budesonide, fluticasone
- Most effective anti-inflammatory agents; reduce exacerbations, symptoms, and improve lung function
Long-Acting Beta-2 Agonists (LABAs)
- Salmeterol, formoterol
- Always used in combination with ICS, never as monotherapy
Leukotriene Receptor Antagonists (LTRAs)
- Montelukast, zafirlukast
- Useful add-on therapy, especially in aspirin-exacerbated asthma and exercise-induced asthma
Theophylline
- Narrow therapeutic window; used as add-on in patients not controlled on ICS/LABA; blood level monitoring required
Biologic (Monoclonal Antibody) Therapies
For severe asthma inadequately controlled on high-dose ICS/LABA:
| Drug | Target | Indication |
|---|---|---|
| Omalizumab (Xolair) | Anti-IgE | Moderate-severe allergic asthma with elevated IgE; reduces exacerbations; risk of anaphylaxis - monitor 30-60 min post-injection |
| Mepolizumab (Nucala) | Anti-IL-5 | Severe eosinophilic asthma (eosinophils >150/µL); 100 mg SC every 4 weeks; ~50% reduction in exacerbations |
| Reslizumab (Cinqair) | Anti-IL-5 | Severe eosinophilic asthma; 3 mg/kg IV every 4 weeks |
| Benralizumab (Fasenra) | Anti-IL-5Rα | Near-complete eosinophil/basophil depletion from blood and lung tissue |
| Dupilumab (Dupixent) | Anti-IL-4Rα (blocks IL-4 + IL-13) | T2-high asthma; also effective in OCS-dependent asthma regardless of biomarkers; also approved for COPD with eosinophilia |
| Tezepelumab (Tezspire) | Anti-TSLP | Broadest indication - reduces exacerbations even in non-T2 asthma without elevated FeNO or eosinophils; 50-70% exacerbation reduction |
- Harrison's 22E, p. 2581-2589
Stepwise GINA Approach (Simplified)
| Step | Treatment |
|---|---|
| Step 1 (Mild intermittent) | SABA as needed; consider low-dose ICS |
| Step 2 (Mild persistent) | Low-dose ICS + SABA reliever |
| Step 3 (Moderate persistent) | Low-dose ICS/LABA or medium-dose ICS |
| Step 4 (Moderate-severe) | Medium- to high-dose ICS/LABA |
| Step 5 (Severe uncontrolled) | High-dose ICS/LABA + add-on (tiotropium, LTRA, macrolides) + biologic therapy |
Special Situations
- Asthma attacks: Escalation of bronchodilators + systemic corticosteroids; if no response - ICU referral
- Status asthmaticus: Life-threatening attack unresponsive to standard treatment; requires IV methylprednisolone, IV magnesium sulfate, possible intubation
- High-risk patients: Prior ICU admission, recent OCS use, >2 hospitalizations/year, history of near-fatal attack
- Elderly: Diagnostic challenges due to overlap with COPD and cardiac disease; underdiagnosis common
- Asthma-COPD Overlap (ACO): Features of both diseases; ICS-based treatment essential
- Pregnancy: Uncontrolled asthma is more dangerous to mother and fetus than asthma medications; continue ICS; salbutamol safe; most biologics category C
- Exercise-induced asthma: Pre-treatment with SABA 15 minutes before exercise; ICS for frequent episodes; LTRA also effective
Summary
Bronchial asthma is a chronic inflammatory airway disease with episodic, largely reversible airway obstruction driven by a complex interplay of genetic susceptibility and environmental triggers. Its pathophysiology centers on airway hyperresponsiveness, inflammation (T2-high or T2-low), and remodeling. Diagnosis rests on clinical history and confirmed reversible airflow obstruction on spirometry. Treatment follows a stepwise approach from SABA rescue inhalers through ICS-based controllers to targeted biologic therapies for severe disease.
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 298
- Goldman-Cecil Medicine, International Edition, Chapter 75 (Drazen JM & Bel EH)
This is a shared conversation. Sign in to Orris to start your own chat.