Patient with ARDS, acute pancreatitis patient, icu management
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive ICU management guide covering both ARDS and acute pancreatitis.
ICU Management: ARDS + Acute Pancreatitis
PART 1 — ARDS
Berlin Definition & Classification
| Severity | P:F Ratio | PEEP Requirement |
|---|---|---|
| Mild | 201–300 | ≥5 cmH₂O |
| Moderate | 101–200 | ≥5 cmH₂O |
| Severe | ≤100 | ≥5 cmH₂O |
Other Berlin criteria: bilateral opacities on CXR/CT not explained by effusions or collapse; respiratory failure not explained by cardiac failure/volume overload; onset within 1 week of clinical insult.
Mortality correlates with severity: mild 27%, moderate 32%, severe 45%.
Treatment — Escalating by Severity
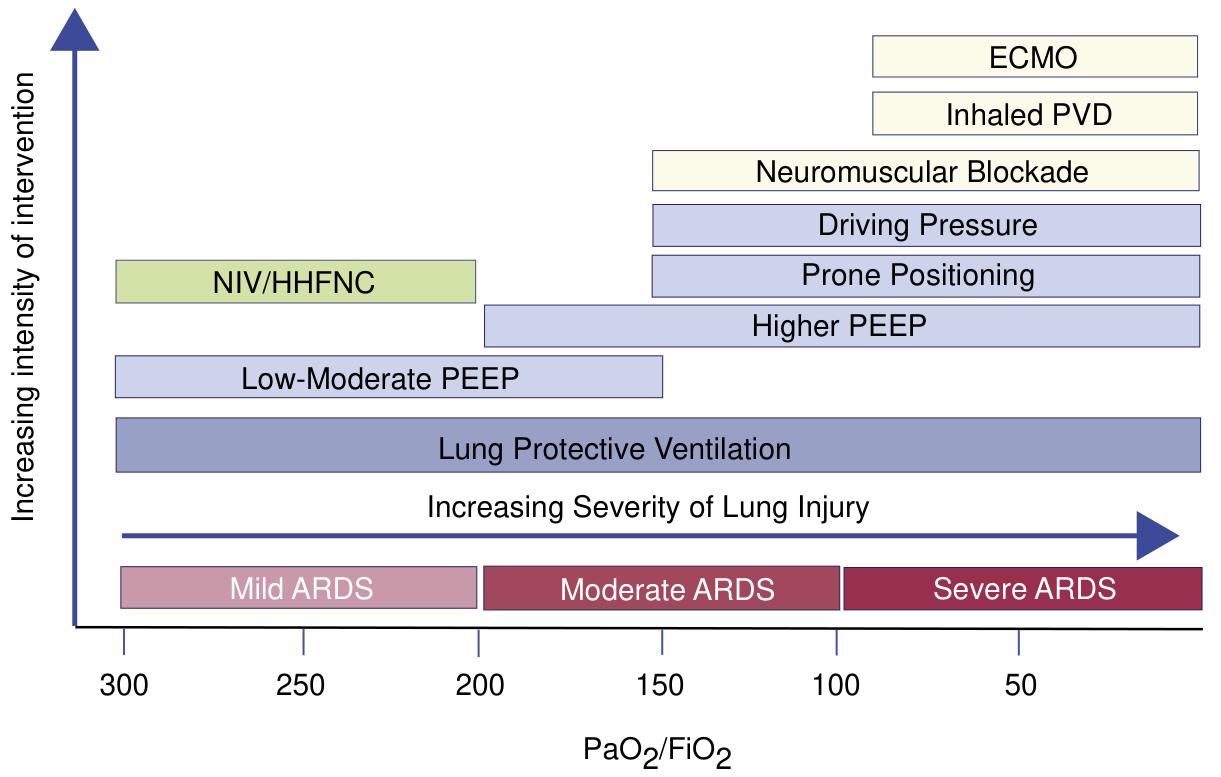
1. Lung-Protective Ventilation (ALL ARDS — cornerstone)
- Tidal volume: 6 mL/kg PBW (start 6–8, reduce by 1 mL/kg q2h to reach 6)
- PBW men: 50 + 2.3 kg per inch over 5 ft
- PBW women: 45.5 + 2.3 kg per inch over 5 ft
- Plateau pressure: <30 cmH₂O (can reduce TV to 4 mL/kg if needed)
- Oxygenation targets: PaO₂ 55–80 mmHg or SpO₂ 88–95%
- Evidence: ARMA trial — 6 mL/kg vs 12 mL/kg → significant mortality reduction
— Current Surgical Therapy 14e
2. PEEP Titration
- Titrate PEEP using FiO₂/PEEP tables (higher PEEP for moderate–severe ARDS)
- Example high-PEEP table:
| FiO₂ | 0.3 | 0.4 | 0.5 | 0.8 | 0.9 | 1.0 |
|---|---|---|---|---|---|---|
| PEEP (cmH₂O) | 8–14 | 14–16 | 16–20 | 22 | 22 | 22–24 |
- ARDS subphenotypes matter: hyperinflammatory (subphenotype 2) benefits from high PEEP; hypoinflammatory (subphenotype 1) does better with low PEEP
— Murray & Nadel's Textbook of Respiratory Medicine
3. Driving Pressure
- ΔP = Plateau pressure − PEEP (reflects tidal volume normalized to lung size)
- Even with "safe" TV and plateau pressures, elevated driving pressure is associated with increased mortality
- Target driving pressure minimization as an independent ventilator goal
4. Permissive Hypercapnia
- Accept elevated PaCO₂ to allow lower tidal volumes and pressures
- Respiratory acidosis managed with NaHCO₃ or THAM
- Caution in TBI — worsens intracranial pressure
5. Prone Positioning (Moderate–Severe ARDS, P:F <150)
- Mechanism: V/Q matching + recruits dependent lung zones
- PROSEVA trial: ≥16 hours/day pronation → 90-day mortality 23.6% vs 41% in supine
- Initiate within 36 hours of onset
- Risks: unplanned extubation, pressure sores, line dislodgement — careful planning essential
6. Conservative Fluid Management
- Target lowest CVP consistent with adequate perfusion
- Consider diuretics when hypoxemia + CVP >4 cmH₂O
- FACTT trial reanalysis: hyperinflammatory subphenotype benefits from conservative strategy; hypoinflammatory from liberal
7. Neuromuscular Blockade (Moderate–Severe, P:F ≤150, <36 h)
- Reduces ventilator dyssynchrony, consumptive O₂ use, excessive tidal volumes
- ACURASYS trial: improved 90-day survival; ROSE trial showed no mortality benefit with light sedation comparison
- Current status: salvage/adjunct for severe ARDS, not routine
8. Corticosteroids
- Early ARDS (within 14 days): methylprednisolone or dexamethasone shown to increase ventilator-free days and reduce mortality
- Dexamethasone protocol (Spanish RCT, 277 patients): 20 mg/day × 5 days → 10 mg/day × 5 days IV → 12.3 vs 7.5 ventilator-free days; 60-day mortality 21% vs 36%
- Late ARDS (>14 days): steroids associated with increased 60- and 180-day mortality — avoid
- SCCM/ESICM 2017 guidelines support low-dose methylprednisolone with taper over 28 days in early ARDS
— Murray & Nadel's Textbook of Respiratory Medicine
9. Salvage Strategies (Refractory Severe ARDS)
| Strategy | Details |
|---|---|
| Recruitment maneuvers | 40 cmH₂O airway pressure × 2 min; monitor for hemodynamic compromise |
| Inhaled pulmonary vasodilators | Nitric oxide (iNO) or prostacyclin — improves oxygenation transiently; no mortality benefit; used as bridge to ECMO |
| ECMO | Last resort; EOLIA trial (2018): no significant 60-day mortality reduction but 28% crossover confounding; used at specialized ARDS referral centers |
10. NIV/HHFNC
- Applicable to mild ARDS and non-intubated patients only
- High-flow nasal cannula (HHFNC) reduces work of breathing, maintains PEEP effect
- NIV appropriate for selected mild cases; risk of delayed intubation if failing
PART 2 — Acute Pancreatitis (AP) ICU Management
Indications for ICU Admission
- Persistent organ failure >48 hours (defines severe AP)
- Hemodynamic instability requiring vasopressors
- SIRS severe enough to require mechanical ventilation
- Respiratory failure (AP-related ARDS occurs in ~20% of severe AP)
Core ICU Principles
1. Fluid Resuscitation
- Aggressive early IV fluids are a mainstay — correct hypovolemia from third-spacing
- Lactated Ringer's preferred over normal saline (reduced inflammatory markers in trials)
- Monitor for abdominal compartment syndrome — excessive fluids worsen outcomes
- Goal-directed resuscitation: target urine output, HR, MAP, lactate clearance
2. Nutrition — Paradigm Shift (Critical)
NPO is obsolete in severe AP — early enteral nutrition is now standard of care.
- ICU patients with severe AP: place NG/NJ tube and initiate EN within 24–36 hours of admission
- Two meta-analyses: EN vs PN in severe AP → 2-fold reduction in infectious complications, 2.5-fold reduction in mortality
- AGA technical review (12 RCTs): EN reduced infected peripancreatic necrosis (OR 0.28), single organ failure (OR 0.25), and MOF (OR 0.41) vs PN
- Gastric vs jejunal feeding: 3 RCTs showed no significant difference in tolerance or clinical outcomes
- Caution: do not initiate EN in hemodynamically unstable patients requiring high-dose vasopressors — risk of non-occlusive mesenteric ischemia
- If patient is managing on ward with minimal SIRS: offer oral diet as tolerated; start EN only if failing to advance diet after 4 days
— Sleisenger & Fordtran's Gastrointestinal and Liver Disease
3. Analgesia
- AP causes severe pain — adequate analgesia is essential and does not worsen outcomes
- IV opioids (morphine, fentanyl, hydromorphone) are appropriate
- Epidural analgesia may be considered in severe cases
- Avoid NSAIDs (renal impairment risk in a volume-depleted patient)
4. Management of Infected Pancreatic Necrosis
- Sterile necrosis: no prophylactic antibiotics (evidence does not support them)
- Infected necrosis (fever + CT evidence of necrosis with gas, or positive FNA): antibiotics — carbapenems (imipenem) or fluoroquinolones + metronidazole (good pancreatic penetration)
- Intervention: step-up approach — percutaneous/endoscopic drainage before open necrosectomy
- Timing: delay necrosectomy ≥4 weeks to allow walling-off (better outcomes)
5. Glycemic Control
- Pancreatitis disrupts endocrine function → hyperglycemia common
- Target glucose 140–180 mg/dL in ICU (tight control <110 increases hypoglycemia risk)
- Insulin infusion as needed
6. Organ Support
| Organ System | Management |
|---|---|
| Respiratory | If ARDS develops (common complication), apply lung-protective ventilation as above |
| Renal | Monitor creatinine, urine output; avoid nephrotoxins; RRT if AKI with severe fluid overload/hyperkalemia/acidosis |
| Cardiovascular | Vasopressors (norepinephrine first-line) for septic shock; MAP target ≥65 |
| Hematologic | Monitor for DIC — AP-associated coagulopathy; FFP/platelets as indicated |
7. Biliary AP
- Urgent ERCP (within 24–72 h) only if concurrent cholangitis or biliary obstruction
- No benefit of ERCP in predicted severe AP without cholangitis
- Cholecystectomy before discharge for biliary AP (or interval in severe cases)
8. Monitoring
- CT abdomen with contrast: not required on admission; indicated at 48–72 h if clinical deterioration or diagnostic uncertainty (CT Severity Index / Balthazar score)
- Serial labs: CRP (>150 mg/L at 48 h = severe disease), CBC, LFTs, creatinine, calcium, glucose, lactate
AP-Related ARDS: The Overlap
Acute pancreatitis is a major cause of indirect (extrapulmonary) ARDS via systemic inflammatory mediator release, phospholipase A₂ activation, and neutrophil sequestration in the pulmonary microvasculature. When AP patients develop ARDS:
- Apply all ARDS management principles above
- Nutritional strategy: continue EN (jejunal) even with ARDS if hemodynamically stable
- Abdominal compartment syndrome can worsen respiratory compliance → monitor intra-abdominal pressure
- The hyperinflammatory ARDS subphenotype is most likely in sepsis-driven AP-ARDS
Sources: Current Surgical Therapy 14e | Murray & Nadel's Textbook of Respiratory Medicine | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.