Detection of diseases of the hepatobillary system, portal hypertension, syndromes of liver damage. Etiology ,pathology, diagnostic,mechanism, medication,normal physiology,, physical examination, therapy,related syndromes, complications
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive, textbook-grounded review of hepatobiliary diseases, portal hypertension, and syndromes of liver damage.
Hepatobiliary Disease, Portal Hypertension & Syndromes of Liver Damage
1. Normal Hepatic Physiology
The liver is the central metabolic organ, responsible for:
- Synthetic functions: coagulation factors (II, V, VII, IX, X, XI, XII, fibrinogen), albumin, acute-phase proteins
- Metabolic functions: gluconeogenesis, lipid metabolism, drug/toxin biotransformation, ammonia detoxification (urea cycle)
- Excretory functions: bilirubin conjugation and secretion into bile, bile salt synthesis
- Immune/clearance functions: Kupffer cell phagocytosis; removal of activated coagulation factors from circulation
The hepatic sinusoid is unique: sinusoidal endothelial cells contain large fenestrae (100–200 nm), allowing passage of macromolecules up to 250,000 Da. There is no basement membrane, permitting free exchange between plasma and hepatocytes across the Space of Disse. — Goldman-Cecil Medicine, p. 1614
2. Etiology of Hepatobiliary Disease
Infectious
| Agent | Disease |
|---|---|
| HAV | Acute hepatitis A (self-limited, fecal-oral) |
| HBV | Acute/chronic hepatitis B, cirrhosis, HCC |
| HCV | Chronic hepatitis C → cirrhosis |
| HEV | Acute hepatitis E (especially pregnant women in Asia) |
| EBV, CMV, HSV | Hepatitis in systemic infection / immunosuppression |
Toxic / Drug-Induced
- Acetaminophen accounts for ~50% of acute liver failure in the United States (zone 3 perivenular necrosis via N-acetyl-p-benzoquinone imine — NAPQI)
- Alcohol: steatohepatitis → cirrhosis
- Valproate, tetracycline, methotrexate (idiosyncratic or dose-related)
Metabolic / Genetic
| Condition | Defect |
|---|---|
| Hemochromatosis | Iron overload |
| Wilson disease | Copper accumulation |
| α1-Antitrypsin deficiency | Protein misfolding, polymerization in hepatocytes |
| Glycogen storage diseases | Enzyme deficiencies |
| NAFLD/NASH | Metabolic syndrome–associated steatohepatitis |
Biliary/Vascular
- Primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC)
- Budd-Chiari syndrome (hepatic vein outflow obstruction)
- Right-sided heart failure → congestive hepatopathy
— Robbins Pathologic Basis of Disease, p. 767–773
3. Pathology of Liver Damage
Cellular Response to Injury
Hepatocyte injury manifests as:
- Steatosis (fat accumulation) — macro- or microvesicular
- Ballooning degeneration (hydropic change)
- Apoptosis → acidophil/Councilman bodies
- Necrosis: zone-specific (zone 3 in ischemia/acetaminophen; zone 1 in yellow fever); bridging necrosis spans portal tracts to central veins; pan-acinar necrosis in massive failure
Fibrosis and Cirrhosis
The key cell is the hepatic stellate cell (Ito cell), which:
- Normally stores vitamin A (lipid droplets) in the Space of Disse
- When activated by TGF-β, PDGF, TNF-α, ROS → differentiates into fibrogenic myofibroblasts → collagen deposition
- Collagen in the Space of Disse causes "capillarization" of sinusoids (defenestration), disrupting hepatocyte-plasma exchange
Cirrhosis = diffuse fibrosis + regenerative nodules. Functionally: loss of normal hepatic architecture, impaired exchange across sinusoids, and sinusoidal compression → portal hypertension. — Robbins, p. 767
4. Portal Hypertension
Definition & Normal Threshold
Normal portal pressure: ~5–10 mmHg. Portal hypertension is defined by hepatic venous pressure gradient (HVPG) >5 mmHg. Clinical complications appear at:
- HVPG ≥10 mmHg: varices begin to form
- HVPG ≥12 mmHg: variceal hemorrhage and ascites risk
Etiology — Classification by Level
Prehepatic
- Portal vein thrombosis / structural narrowing
- Massive splenomegaly with ↑ splenic blood flow
Intrahepatic (most common)
- Cirrhosis (all causes) — dominant cause worldwide
- Nodular regenerative hyperplasia
- Primary biliary cholangitis
- Schistosomiasis (periportal fibrosis)
- Massive fatty change, sarcoidosis, amyloidosis
- Infiltrative malignancy (primary or metastatic)
- HCC with portal vein invasion
Posthepatic
- Severe right-sided heart failure
- Constrictive pericarditis
- Budd-Chiari syndrome (hepatic vein outflow obstruction)
— Robbins, p. 55–62
Pathophysiology / Mechanism
Two components operate simultaneously:
-
Increased sinusoidal resistance (fixed + functional):
- Fixed: fibrosis, regenerative nodules compress sinusoids
- Functional: intrahepatic vasoconstriction due to ↓ NO production by sinusoidal endothelium + ↑ endothelin-1, angiotensinogen, eicosanoids → stellate cell/myofibroblast contraction
-
Increased portal venous inflow (hyperdynamic circulation):
- Splanchnic arterial vasodilation (principal mediator: NO from excessive systemic production)
- ↑ splanchnic blood flow → ↑ portal venous efflux
- Systemic vasodilation → ↓ effective arterial blood volume → activation of RAAS + sympathetic NS → Na⁺ and water retention → plasma volume expansion → further ↑ portal inflow
The paradox: intrahepatic NO is deficient (vasoconstriction), while extrahepatic/splanchnic NO is excess (vasodilation). — Goldman-Cecil, p. 1615
5. Four Major Consequences of Portal Hypertension
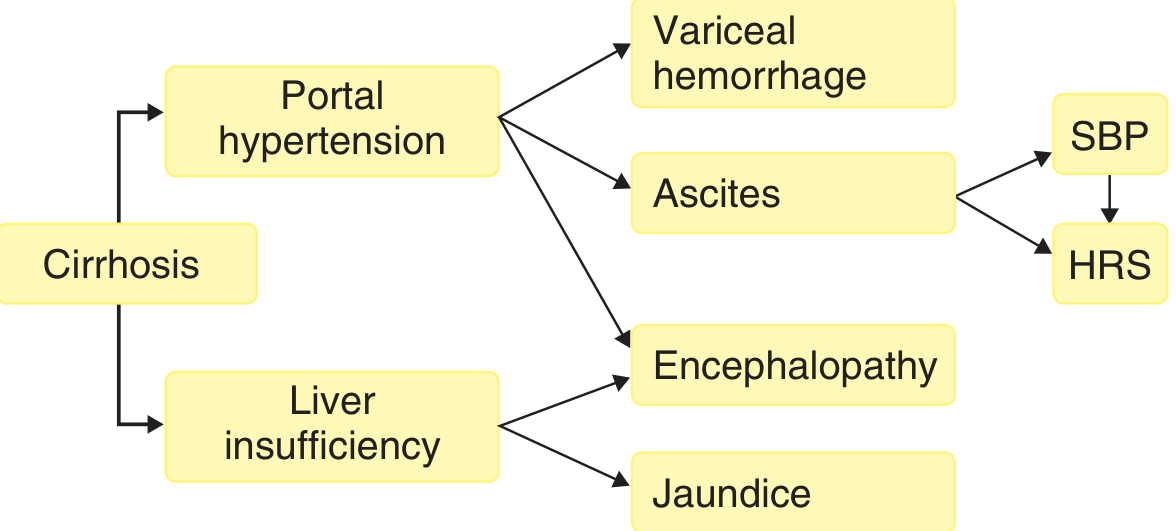
(A) Varices & Variceal Hemorrhage
- Portosystemic collaterals form when coronary/gastric veins reverse flow
- Gastroesophageal varices are clinically most important
- Rupture risk proportional to variceal diameter and intravariceal pressure
- Mortality from first bleed: ~20–30%
(B) Ascites
- Accumulation of fluid in the peritoneal cavity; cirrhosis accounts for 85% of cases
- Requires HVPG ≥12 mmHg
- Mechanism: sinusoidal hypertension + Na⁺ retention (RAAS activation)
- Advanced: refractory ascites, hyponatremia (water retention), hepatorenal syndrome
(C) Portosystemic Venous Shunts
- Esophageal varices, hemorrhoidal varices, caput medusae (periumbilical), retroperitoneal collaterals
- Bypass hepatic Kupffer cells → toxins/bacteria reach systemic circulation → encephalopathy risk
(D) Congestive Splenomegaly
- Passive congestion → splenomegaly → hypersplenism: thrombocytopenia, leukopenia, anemia
6. Syndromes of Liver Damage / Hepatic Failure
Acute Liver Failure (Fulminant Hepatic Failure)
Definition: encephalopathy + coagulopathy within 26 weeks of acute liver injury, without preexisting liver disease.
Etiology:
- Acetaminophen overdose (~50% of US cases)
- Autoimmune hepatitis, other drugs/toxins
- Viral: HAV, HBV, HEV (Asia)
- Rare: Budd-Chiari, Wilson disease, lymphoma/leukemia
Clinical features (in sequence):
- Nausea, vomiting, jaundice → transaminases markedly elevated
- Encephalopathy (asterixis, confusion → coma)
- Coagulopathy (easy bruisability → intracranial bleeding)
- Cholestasis (↑ bilirubin, bile stasis)
- Multi-organ failure
Important caveat: falling transaminases in the setting of worsening jaundice + coagulopathy + encephalopathy = prognostic sign of hepatocyte depletion, not improvement. — Robbins, p. 768
Chronic Liver Failure / Decompensated Cirrhosis
80–90% of functional capacity must be lost before failure appears.
7. Physical Examination Signs
| Sign | Mechanism / Significance |
|---|---|
| Jaundice / icterus | Bilirubin retention (liver insufficiency) |
| Spider angiomata | Hyperestrogenemia (↓ estrogen catabolism) |
| Palmar erythema | Hyperestrogenemia |
| Caput medusae | Periumbilical portosystemic collaterals |
| Asterixis (flapping tremor) | Hepatic encephalopathy; nonrhythmic rapid extension-flexion of dorsiflexed wrists |
| Fetor hepaticus | Sweet/musty breath; portosystemic shunting of sulfur compounds |
| Leukonychia / Terry's nails | Hypoalbuminemia |
| Dupuytren contracture | Associated with alcoholic liver disease |
| Gynecomastia / testicular atrophy | Hyperestrogenemia |
| Ascites | Shifting dullness, fluid wave, everted umbilicus |
| Hepatomegaly / liver atrophy | Depends on stage |
| Splenomegaly | Congestive, hypersplenism |
| Clubbing + cyanosis | Hepatopulmonary syndrome |
8. Diagnostic Evaluation
Liver Function Tests
| Test | What It Reflects |
|---|---|
| ALT, AST | Hepatocellular injury (ALT more liver-specific) |
| ALP, GGT | Cholestatic disease / biliary pathology |
| Bilirubin (total, direct/indirect) | Conjugation and excretion capacity |
| Albumin | Synthetic function (chronic disease) |
| PT/INR | Synthetic function (acute or chronic) |
| Ammonia | Urea cycle function; encephalopathy |
Serologic Markers
- HBsAg: active HBV infection
- Anti-HBs: recovery/immunity
- HBeAg: high replicative state of HBV
- Anti-HCV: exposure; confirmed by HCV RNA
- Anti-HAV IgM: acute HAV infection
- AMA (anti-mitochondrial Ab): primary biliary cholangitis
- ANA, anti-smooth muscle Ab: autoimmune hepatitis
- Ceruloplasmin ↓, urine copper ↑: Wilson disease
- Ferritin, transferrin saturation ↑: hemochromatosis
Ascites Evaluation: SAAG
- SAAG (serum-ascites albumin gradient) ≥1.1 g/dL → portal hypertension cause
- PMN count in ascitic fluid >250/μL → spontaneous bacterial peritonitis (SBP)
Hepatic Venous Pressure Gradient (HVPG)
- Gold standard to quantify portal hypertension
- HVPG >10 mmHg: clinically significant portal hypertension
MELD Score
Used to assess severity of chronic liver disease and prioritize liver transplantation:
MELD = [0.957 × ln(Cr) + 0.378 × ln(Bil) + 1.12 × ln(INR) + 0.643] × 10
MELD-Na incorporates serum sodium when initial MELD ≥12. — Goldman-Cecil, p. 1619
Imaging
- Ultrasound: first-line; detects nodularity, ascites, splenomegaly, portal vein dilation, Doppler flow reversal
- CT/MRI: staging, detection of HCC, vascular anatomy
- Elastography (FibroScan): non-invasive fibrosis quantification
- Liver biopsy: gold standard for fibrosis staging, hepatitis grading, storage disease diagnosis
9. Complications and Related Syndromes
Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid without secondary cause
- Mechanism: bacterial translocation from gut lumen → mesenteric lymph nodes → transient bacteremia → colonizes ascitic fluid (low complement, low opsonic activity)
- Organisms: gram-negative enteric (E. coli, Klebsiella) predominantly; increasing multidrug-resistant organisms with prophylaxis use
- Diagnosis: PMN >250/μL in ascitic fluid
- Treatment: 3rd-generation cephalosporins (cefotaxime); albumin IV to prevent hepatorenal syndrome
- Prophylaxis: norfloxacin or trimethoprim-sulfamethoxazole in high-risk patients (prior SBP, low protein ascites)
Hepatorenal Syndrome (HRS)
- Prerenal kidney injury in cirrhosis from maximal splanchnic vasodilation → renal vasoconstriction
- HRS-AKI (Type 1): rapidly progressive, creatinine doubles within 2 weeks; triggered by SBP, hemorrhage
- HRS-non-AKI (Type 2): slower, associated with refractory ascites
- Treatment: vasoconstrictor (terlipressin or norepinephrine) + albumin; liver transplantation is definitive
Hepatic Encephalopathy (HE)
- Neuropsychiatric manifestation caused by ammonia (from gut bacteria + enterocytes) bypassing hepatic detoxification
- Ammonia → astrocyte swelling (glutamine as osmolyte) → cerebral edema
- Grades:
- Grade 1: sleep-wake inversion, forgetfulness
- Grade 2: confusion, bizarre behavior, disorientation
- Grade 3: lethargy, profound disorientation
- Grade 4: coma
- Hallmark sign: asterixis (flapping tremor)
- Treatment: lactulose (reduces ammonia production/absorption), rifaximin (non-absorbable antibiotic), dietary protein restriction (avoid excess)
- Precipitants: GI bleed, infection, constipation, hypokalemia, sedatives
Hepatopulmonary Syndrome
- Intrapulmonary vascular dilatations → V/Q mismatch and shunting → hypoxemia
- Diagnosis: PaO₂ <80 mmHg + positive contrast echocardiography (microbubbles in left heart)
- Signs: platypnea (dyspnea worsening upright), orthodeoxia, clubbing, cyanosis
- Present in 5–10% of liver transplant candidates; resolves post-transplant
Portopulmonary Hypertension
- Pulmonary arterial hypertension in the setting of portal hypertension
- Diagnosis: mean PAP >25 mmHg on right heart catheterization + PCWP <15 mmHg
Coagulopathy of Liver Disease
- Liver synthesizes factors II, V, VII, IX, X, XI, XII, fibrinogen + anticoagulants (protein C, S, antithrombin)
- Paradoxically "rebalanced" coagulopathy — bleeding AND thrombosis risk
- PT/INR prolonged; thrombocytopenia from hypersplenism
10. Treatment Overview
Treating the Underlying Cause
| Disease | Specific Therapy |
|---|---|
| HBV | Tenofovir, entecavir (nucleos(t)ide analogues) |
| HCV | Direct-acting antivirals (DAAs) — >95% cure |
| Alcoholic hepatitis | Prednisolone (severe); abstinence |
| Autoimmune hepatitis | Prednisolone + azathioprine |
| Hemochromatosis | Phlebotomy; chelation (deferasirox) |
| Wilson disease | Penicillamine, trientine, zinc |
| NASH | Weight loss, metabolic control |
| PBC | Ursodeoxycholic acid (UDCA); obeticholic acid |
| PSC | UDCA (limited benefit); manage complications |
Reducing Portal Pressure
- Non-selective beta-blockers (propranolol, carvedilol): reduce cardiac output AND splanchnic vasodilation; primary and secondary prophylaxis against variceal hemorrhage and decompensation
- Endoscopic band ligation (EBL): acute variceal bleeding and secondary prophylaxis
- Endoscopic sclerotherapy: alternative to EBL
- TIPS (Transjugular Intrahepatic Portosystemic Shunt): refractory bleeding, refractory ascites; creates intrahepatic porto-systemic shunt; risk: worsening encephalopathy
Managing Ascites
- Na⁺ restriction (<2 g/day), fluid restriction (if hyponatremic)
- Spironolactone (first-line diuretic; blocks aldosterone) ± furosemide
- Large-volume paracentesis + albumin replacement (8 g per liter removed) for tense ascites
- TIPS for refractory ascites
Hepatic Encephalopathy
- Identify and treat precipitants
- Lactulose: cathartic; acidifies colon → traps NH₃ as NH₄⁺; target 2–3 soft stools/day
- Rifaximin: poorly absorbed antibiotic; reduces gut ammonia-producing bacteria; maintenance therapy
Liver Transplantation
- Definitive therapy for end-stage liver disease
- Indicated when MELD-Na ≥15 or decompensating events occur
- Corrects both liver failure and portal hypertension
- HCC within Milan criteria is a transplant indication
- Post-transplant: lifelong immunosuppression (calcineurin inhibitors ± mycophenolate)
Summary Table: Syndromes of Liver Damage
| Syndrome | Key Feature | Mechanism |
|---|---|---|
| Acute liver failure | Encephalopathy + coagulopathy <26 wks | Massive hepatocyte necrosis |
| Cirrhosis | Fibrosis + nodules | Chronic stellate cell activation |
| Portal hypertension | HVPG >5 mmHg | ↑ resistance + ↑ portal inflow |
| Ascites | Peritoneal fluid | Sinusoidal HTN + Na⁺ retention |
| Variceal hemorrhage | GI bleed | Portosystemic collaterals rupture |
| SBP | PMN >250 in ascites | Bacterial translocation |
| HRS | AKI without intrinsic renal disease | Renal vasoconstriction |
| HE | Neuropsychiatric | Ammonia + cerebral edema |
| Hepatopulmonary syndrome | Hypoxemia | Intrapulmonary vascular dilation |
| Portopulmonary HTN | PAH in liver disease | Vasoactive mediators in pulmonary vasculature |
| Coagulopathy | Prolonged PT, bleeding | ↓ factor synthesis |
| Hypersplenism | Cytopenias | Congestive splenomegaly |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 55–120, 767–780); Goldman-Cecil Medicine International Edition (pp. 1613–1625)
Diagnosis and physical examination, complications for hepatobillary disease
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Here is a focused, textbook-level deep dive on diagnosis, physical examination, and complications of hepatobiliary disease.
Diagnosis & Physical Examination of Hepatobiliary Disease
1. Diagnostic Approach — Overview
The initial goal is to distinguish hepatocellular disease from biliary obstruction (cholestatic disease), as the management differs fundamentally.
The diagnostic workup begins with:
- Careful history
- Physical examination
- Screening laboratory studies: total and direct bilirubin, ALT, AST, ALP, PT
"Regardless of how the patient comes to medical attention, the diagnostic approach begins with a careful history, physical examination, and screening laboratory studies... The ability to distinguish between liver disease and biliary tract obstruction is the major goal of the initial evaluation." — Goldman-Cecil Medicine, p. 1558
2. History Taking — Key Elements
| Domain | Clues |
|---|---|
| Alcohol consumption | Amount, duration, type — alcoholic hepatitis / cirrhosis |
| Medications / supplements | Drug-induced liver injury (DIL I); herbal products often overlooked |
| IV drug use / cocaine | Viral hepatitis risk (HBV, HCV) |
| Sexual history / exposures | HBV sexual transmission |
| Prior hepatobiliary surgery | Biliary stricture, retained stones, post-op jaundice |
| Family history | Wilson disease, hemochromatosis, α1-antitrypsin deficiency, Gilbert syndrome |
| Travel history | HAV, HEV, amoebiasis |
| Abdominal pain character | RUQ colicky pain → biliary; dull constant → hepatic capsule stretch |
| Acholic stools + dark urine | Biliary obstruction (conjugated hyperbilirubinemia) |
| Fever, rigors | Cholangitis (Charcot's triad: RUQ pain + fever + jaundice) |
| Anorexia, myalgias, viral prodrome | Acute viral hepatitis |
| Weight loss | Malignancy |
3. Physical Examination
Systematic Approach
Inspection (General)
| Finding | Significance |
|---|---|
| Jaundice (scleral icterus first) | Bilirubin >2–3 mg/dL; begins in sclerae before skin |
| Cachexia / muscle wasting | Advanced cirrhosis, malignancy |
| Xanthelasma / xanthomas | Chronic cholestasis (PBC) — lipid retention |
| Scratch marks (excoriations) | Pruritus from cholestasis; bile salt deposition in skin |
Hands & Arms
| Finding | Mechanism |
|---|---|
| Palmar erythema | Hyperestrogenemia (impaired estrogen catabolism by failing liver) |
| Leukonychia (white nails / Terry's nails) | Hypoalbuminemia |
| Dupuytren's contracture | Associated with alcoholic liver disease |
| Asterixis (flapping tremor) | Hepatic encephalopathy — ask patient to dorsiflex wrists with arms outstretched; nonrhythmic rapid extension-flexion movements |
| Clubbing | Hepatopulmonary syndrome |
| Bruising / petechiae | Coagulopathy + thrombocytopenia |
Face & Neck
| Finding | Mechanism |
|---|---|
| Scleral icterus | First visible sign of jaundice |
| Parotid enlargement | Alcoholic liver disease |
| Fetor hepaticus | Sweet/musty odor; portosystemic shunting of mercaptans and dimethyl sulfide |
| Kayser-Fleischer rings | Copper deposition in Descemet's membrane; pathognomonic for Wilson disease (requires slit-lamp) |
Chest & Abdomen
| Finding | Mechanism |
|---|---|
| Spider angiomata | Central arteriole with radiating vessels; >5 significant; hyperestrogenemia |
| Gynecomastia | Hyperestrogenemia in males |
| Caput medusae | Dilated periumbilical veins; portosystemic collaterals via paraumbilical vein |
| Hepatomegaly | Active hepatitis, infiltration, early cirrhosis, congestion |
| Liver atrophy | End-stage cirrhosis |
| Liver tenderness | Hepatitis (acute), congestive hepatopathy, abscess |
| Murphy's sign | Inspiratory arrest on RUQ palpation during deep breath; acute cholecystitis |
| Palpable gallbladder (Courvoisier's sign) | Non-tender palpable gallbladder + jaundice → carcinoma of pancreatic head or biliary tree (not gallstones, which cause a fibrotic gallbladder) |
| Splenomegaly | Portal hypertension / hypersplenism |
| Ascites | Shifting dullness (500 mL needed), fluid wave (>1000 mL); everted umbilicus |
Lower Limbs
| Finding | Mechanism |
|---|---|
| Pitting oedema | Hypoalbuminemia + Na⁺/water retention |
| Testicular atrophy | Hyperestrogenemia |
Summary Table: Physical Exam Signs by Disease Type
| Sign | Disease Association |
|---|---|
| Spider angiomata, palmar erythema | Cirrhosis (any cause) |
| Asterixis, fetor hepaticus | Hepatic encephalopathy |
| Kayser-Fleischer rings | Wilson disease |
| Xanthelasma, scratch marks | PBC / chronic cholestasis |
| Caput medusae | Portal hypertension |
| Courvoisier's sign | Pancreatic/biliary malignancy |
| Murphy's sign | Acute cholecystitis |
| Dupuytren, parotid enlargement | Alcoholic liver disease |
| Clubbing + cyanosis | Hepatopulmonary syndrome |
4. Diagnostic Algorithm — Liver Test Abnormalities
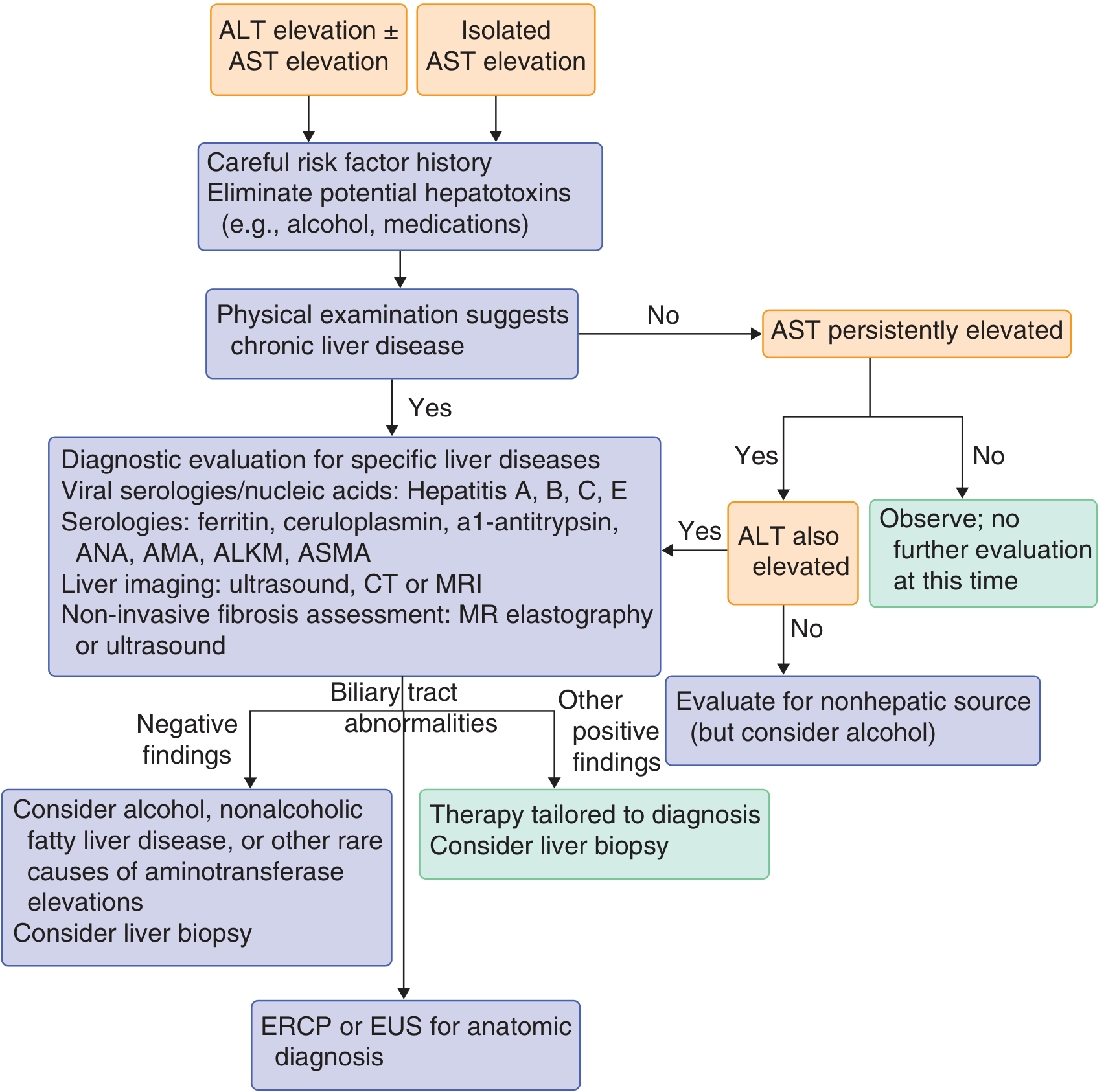
Approach to evaluation of isolated elevated ALT/AST — Goldman-Cecil Medicine
5. Laboratory Investigations
Serum Enzyme Tests (Markers of Injury)
Enzymes are released when hepatocyte plasma membrane phospholipases are activated by injury, creating "holes" in the cell membrane.
| Test | Normal Role | Elevation Suggests |
|---|---|---|
| ALT (SGPT) | Cytosolic enzyme, liver-specific | Hepatocellular necrosis |
| AST (SGOT) | Mitochondrial + cytosolic; less specific (heart, muscle, RBCs) | Hepatocellular injury; cardiac, muscle |
| AST:ALT ratio >2 | — | Alcoholic liver disease (mitochondrial AST + pyridoxine deficiency depletes ALT), Wilson disease |
| ALP | Biliary canalicular membrane | Cholestasis (obstruction, infiltrative disease); also bone |
| GGT | Biliary epithelium | Cholestasis; elevated by alcohol; confirms hepatic source of elevated ALP |
| 5'-Nucleotidase | Biliary epithelium | Liver-specific marker of cholestasis; confirms hepatic source of ALP elevation |
ALP interpretation:
- ≤3× ULN: parenchymal disease (hepatitis, cirrhosis)
- 3–10× ULN: biliary obstruction, cholestatic disease
-
10× ULN: complete biliary obstruction, infiltrative disease (lymphoma, granulomas)
Markers of Hepatic Synthetic Function
| Test | Details |
|---|---|
| PT / INR | Most sensitive acute marker; factor VII has the shortest half-life (~4–6 hrs); fails to normalize with vitamin K in hepatocellular failure (distinguishes from cholestatic deficiency) |
| Albumin | Reflects chronic synthetic function (t½ = 21 days); hypoalbuminemia = diminished hepatic synthesis OR increased losses (nephrotic syndrome, GI losses, burns) |
| Fibrinogen | Decreased in severe hepatic failure |
Bilirubin Fractions
| Type | Mechanism | Causes |
|---|---|---|
| Unconjugated (indirect) ↑ | Hemolysis, impaired uptake/conjugation | Hemolysis, Gilbert syndrome, Crigler-Najjar |
| Conjugated (direct) ↑ | Impaired canalicular excretion or biliary obstruction | Hepatitis, cirrhosis, cholestasis, obstruction |
| Delta bilirubin | Covalently bound to albumin; persists weeks after resolution | Post-obstructive jaundice; may mislead post-ERCP |
Special Serologic Tests
| Test | Interpretation |
|---|---|
| HBsAg | Active HBV infection |
| Anti-HBs | Recovery / vaccination immunity |
| HBeAg | High viral replicative state (HBV) |
| HBV DNA | Quantifies replication; guides therapy |
| Anti-HCV → HCV RNA | Exposure; RNA confirms active infection |
| Anti-HAV IgM | Acute HAV |
| Anti-AMA | Primary biliary cholangitis (PBC) — >95% sensitivity |
| ANA, anti-smooth muscle Ab (ASMA) | Autoimmune hepatitis |
| Anti-LKM1 | Type 2 autoimmune hepatitis |
| Ferritin ↑, transferrin saturation >45% | Hemochromatosis → confirm HFE gene mutation |
| Ceruloplasmin ↓, 24-hr urine copper ↑ | Wilson disease |
| α1-Antitrypsin level + phenotype (PiZZ) | α1-AT deficiency |
Ammonia
- Elevated in portosystemic shunting or severe hepatic dysfunction
- Does not correlate well with encephalopathy grade clinically
- Levels >150 μmol/L useful as supportive evidence only
- Best measured on iced arterial sample — Goldman-Cecil Medicine, p. 1560
Hematologic Findings in Liver Disease
| Finding | Mechanism |
|---|---|
| Thrombocytopenia | Hypersplenism; most common; surrogate marker of portal hypertension |
| Anemia | Hemolysis, marrow suppression (alcohol), GI bleeding |
| Leukopenia | Hypersplenism; atypical lymphocytes in viral hepatitis |
| Target cells | Cholestatic liver disease — abnormal serum lipids expand RBC membrane |
| Spur cell hemolytic anemia (acanthocytes) + hypertriglyceridemia = Zieve syndrome | Severe alcoholic liver disease |
| Macrocytosis | Alcohol (direct marrow effect), folate deficiency |
6. Imaging
Obstructive Jaundice vs. Parenchymal Disease — Imaging Selection
| Scenario | Best Initial Test |
|---|---|
| Suspected cholelithiasis / biliary colic | Ultrasound (no radiation, portable, cheap, highly sensitive for gallstones) |
| Suspected biliary obstruction | Ultrasound → if dilated ducts → MRCP (non-invasive) or ERCP (therapeutic) |
| Liver mass characterization | CT (triple-phase) or MRI with gadolinium |
| Portal hypertension | Ultrasound with Doppler (portal vein flow, diameter, splenomegaly) |
| Intermediate probability of obstruction | MRCP — best non-invasive biliary imaging |
| Suspected pancreatic/bile duct cancer, tissue needed | EUS + FNA |
| Fibrosis staging (non-invasive) | Transient elastography (FibroScan) or MR elastography |
| Post-cholecystectomy biliary anatomy | ERCP or PTC (percutaneous transhepatic cholangiography) |
Key point: biliary dilation is the key imaging finding separating mechanical obstruction from parenchymal liver disease. Mild dilation post-cholecystectomy is a normal variant and should not be over-interpreted.
Liver Biopsy
- Gold standard for: fibrosis staging, hepatitis grading, storage disease diagnosis, infiltrative malignancy
- Indications: persistently elevated aminotransferases without diagnosis after non-invasive workup; suspected autoimmune hepatitis; metabolic liver disease characterization
- Percutaneous, transjugular (if coagulopathy), or laparoscopic
7. Distinguishing Obstructive vs. Parenchymal Jaundice
| Feature | Obstructive (Biliary) Jaundice | Parenchymal Liver Disease |
|---|---|---|
| History | Abdominal pain, fever/rigors, prior biliary surgery, acholic stools | Anorexia, myalgias, viral prodrome, drug/toxin exposure, family history |
| Physical exam | High fever, abdominal tenderness, palpable mass, Murphy's sign, Courvoisier's sign | Ascites, spider angiomata, caput medusae, gynecomastia, asterixis, encephalopathy, K-F rings |
| Labs | ↑↑ ALP with varying bilirubin; PT normalizes with vitamin K | ↑↑ ALT/AST; PT does NOT correct with vitamin K |
| Imaging | Dilated intra/extrahepatic bile ducts | Normal bile ducts; nodular liver, splenomegaly |
— Goldman-Cecil Medicine, p. 1559 (Table 133-3)
8. Complications of Hepatobiliary Disease
A. Complications of Cirrhosis
"Decompensated cirrhosis is defined by the development of ascites, variceal hemorrhage, encephalopathy, or jaundice." — Goldman-Cecil Medicine, p. 1615
1. Portal Hypertension → Varices → Variceal Hemorrhage
- Most lethal acute complication
- Gastroesophageal varices develop when HVPG ≥10 mmHg; rupture when HVPG ≥12 mmHg
- Presentation: hematemesis, melena, hematochezia + hemodynamic compromise
- Mortality 15–20% per episode
- Management: IV octreotide (splanchnic vasoconstriction), endoscopic band ligation, beta-blockers (prophylaxis), TIPS (refractory)
2. Ascites
- HVPG ≥12 mmHg threshold required
- Mechanism: sinusoidal HTN → splanchnic vasodilation → RAAS activation → Na⁺ retention
- Graded: Grade 1 (detectable only on ultrasound) → Grade 2 (moderate, obvious) → Grade 3 (tense/refractory)
- Complications of ascites:
- Spontaneous bacterial peritonitis (SBP)
- Hepatorenal syndrome (HRS)
- Hyponatremia (water retention, dilutional)
- Umbilical hernia (from ↑ intra-abdominal pressure)
3. Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid without secondary cause
- Most common organisms: E. coli, Klebsiella, streptococci
- Diagnosis: ascitic fluid PMN ≥250 cells/μL (even without positive culture)
- Bacteria cultured in only 40–50% of cases
- Clinical features: fever, jaundice, abdominal pain/tenderness ± rebound; up to 1/3 are initially asymptomatic and present with encephalopathy or renal failure
- Treatment: IV cefotaxime (3rd-generation cephalosporin) + IV albumin 1.5 g/kg day 1, 1 g/kg day 3 (prevents HRS)
- Prophylaxis: norfloxacin or trimethoprim-sulfamethoxazole for secondary prevention
4. Hepatorenal Syndrome (HRS)
- Functional (not structural) renal failure in cirrhosis; diagnosis of exclusion
- Caused by maximal splanchnic vasodilation → reflex renal vasoconstriction → ↓ GFR
- HRS-AKI (Type 1): creatinine doubles to >2.5 mg/dL within 2 weeks; poor prognosis; often precipitated by SBP or hemorrhage
- HRS-non-AKI (Type 2): slower onset; associated with refractory ascites; less acute
- Urine: low Na⁺ (<10 mEq/L), no proteinuria, no casts (distinguishes from ATN)
- Treatment: vasoconstrictors (terlipressin, norepinephrine) + IV albumin; liver transplant is definitive
5. Hepatic Encephalopathy (HE)
- Neuropsychiatric syndrome from ammonia + astrocyte swelling
- Incidence 2–3% per year in cirrhosis
- Clinical grades:
- Grade 1: sleep-wake inversion, irritability, mild confusion
- Grade 2: lethargy, disorientation, inappropriate behavior
- Grade 3: marked confusion, stupor, semi-responsiveness
- Grade 4: coma
- Hallmark: asterixis (flapping tremor); fetor hepaticus
- EEG: generalized slow waves + triphasic waves
- Ammonia levels unreliable for grading; levels >150 μmol/L supportive of HE
- Minimal HE (subclinical): present in up to 80% of cirrhotics; detected by psychometric tests only
- Precipitating factors: GI bleed, infection, constipation, hypokalemia, alkalosis, sedatives, excess dietary protein, dehydration
- Treatment: lactulose (target 2–3 soft stools/day), rifaximin (maintenance), identify + correct precipitant
6. Hepatocellular Carcinoma (HCC)
- Complication of cirrhosis (especially HBV, HCV, alcoholic, NASH, hemochromatosis)
- Risk: ~1–4% per year in cirrhotic patients
- Surveillance: ultrasound ± AFP every 6 months
- Diagnosis confirmed by dynamic CT/MRI (arterial enhancement + portal washout = hallmark)
- Regan isozyme (ALP variant) associated with HCC
- Treatment depends on stage: resection, ablation, TACE, sorafenib/lenvatinib, transplant (Milan criteria)
7. Hepatopulmonary Syndrome (HPS)
- Intrapulmonary vascular dilation → V/Q mismatch + right-to-left shunting
- Symptoms: exertional dyspnea → progressive hypoxemia, orthodeoxia (dyspnea worsening upright), platypnea (breathlessness upright)
- Signs: clubbing, cyanosis, vascular spiders
- Present in 5–10% of patients awaiting liver transplant
- Diagnosis: PaO₂ <80 mmHg + contrast echocardiography showing delayed microbubble appearance in left heart (after 3–5 beats)
- Alternative: ⁹⁹ᵐTc-MAA lung scan showing >6% abnormal shunting to brain
- Treatment: liver transplantation (only definitive therapy; reverses HPS)
8. Portopulmonary Hypertension (PPH)
- Pulmonary arterial hypertension in the setting of portal hypertension
- Diagnosis: mean PAP >25 mmHg + PCWP <15 mmHg on right heart catheterization
- Manifestations: progressive dyspnea, right heart failure
- Severe PPH (mPAP >50 mmHg) is a contraindication to liver transplantation (prohibitive surgical mortality)
- Treatment: pulmonary vasodilators (epoprostenol, sildenafil, bosentan)
9. Coagulopathy
- Liver produces ALL coagulation factors except von Willebrand factor
- Factors II, V, VII, IX, X, XI, XII + fibrinogen deficient in liver failure
- Factor VII is first and most severely depressed (shortest half-life)
- Paradox: rebalanced coagulopathy — simultaneous loss of pro- and anticoagulants (protein C, protein S, antithrombin) → both bleeding AND thrombosis risk
- DIC can develop as secondary complication in acute liver failure
10. Hypersplenism
- Passive congestion → splenomegaly → sequestration and destruction of blood cells
- Results: thrombocytopenia (<100,000/μL), leukopenia, anemia
- Thrombocytopenia is often the first lab abnormality in compensated cirrhosis; surrogate marker of portal hypertension
B. Complications of Specific Hepatobiliary Diseases
Acute Cholecystitis
- Complication of gallstone disease (95%): stone impaction in cystic duct → gallbladder inflammation
- Signs: Murphy's sign (positive in ~65%), RUQ tenderness, fever, leukocytosis
- Complications: gangrenous cholecystitis, empyema, perforation (peritonitis), cholecystoenteric fistula, gallstone ileus
Ascending Cholangitis
- Biliary obstruction + infection → Charcot's triad: RUQ pain + fever/rigors + jaundice
- Reynolds' pentad (severe): Charcot's triad + shock + altered mental status → biliary sepsis
- Most common organisms: gram-negatives (E. coli, Klebsiella) ± anaerobes
- Urgently needs biliary drainage (ERCP ± sphincterotomy / PTC)
Choledocholithiasis
- Common bile duct stones: jaundice, cholangitis, acute pancreatitis
- Diagnosis: MRCP (non-invasive), EUS, or ERCP (diagnostic + therapeutic)
Budd-Chiari Syndrome
- Hepatic vein / IVC outflow obstruction → postsinusoidal portal hypertension
- Acute: painful hepatomegaly, ascites, liver failure
- Causes: hypercoagulable states (myeloproliferative disorders, Factor V Leiden, OCP use), tumor invasion
- Diagnosis: Doppler ultrasound (absent/reversed hepatic vein flow), CT/MRI
- Treatment: anticoagulation, TIPS, liver transplantation
9. MELD Score — Severity & Transplant Prioritization
$$\text{MELD} = [0.957 \times \ln(\text{Cr}) + 0.378 \times \ln(\text{Bil}) + 1.12 \times \ln(\text{INR}) + 0.643] \times 10$$
- MELD-Na adds serum sodium adjustment for MELD ≥12
- Predicts 90-day mortality in end-stage liver disease
- Score ≥15: benefits of transplantation outweigh risks
- Score ≥40: >70% 3-month mortality without transplant
— Goldman-Cecil Medicine, p. 1619
10. Summary: Complications at a Glance
| Complication | Key Feature | Diagnostic Test | Treatment |
|---|---|---|---|
| Variceal hemorrhage | Hematemesis + shock | Endoscopy | Octreotide + EBL + beta-blockers |
| Ascites | Shifting dullness, fluid wave | Paracentesis + SAAG | Spironolactone, furosemide, LVP |
| SBP | Ascitic PMN >250/μL | Diagnostic paracentesis | Cefotaxime + albumin |
| Hepatorenal syndrome | Rising Cr, low urine Na | Exclude other causes | Terlipressin + albumin; transplant |
| Hepatic encephalopathy | Asterixis, confusion | Clinical ± ammonia | Lactulose + rifaximin |
| HCC | Liver mass with arterial enhancement | US surveillance → CT/MRI | Resection/transplant/TACE |
| Hepatopulmonary syndrome | Hypoxemia, orthodeoxia | Contrast echo | Liver transplant |
| Portopulmonary HTN | Dyspnea, right HF | RHC (mPAP >25) | Vasodilators; transplant if mPAP <50 |
| Cholangitis | Charcot's triad | Blood cultures + imaging | Antibiotics + biliary drainage (ERCP) |
| Budd-Chiari | Hepatomegaly + ascites | Doppler US / MRI | Anticoagulation + TIPS/transplant |
| Coagulopathy | ↑PT, bleeding | PT/INR, fibrinogen | Treat cause; FFP/PCC if bleeding |
Sources: Goldman-Cecil Medicine International Edition (pp. 1558–1625); Robbins, Cotran & Kumar Pathologic Basis of Disease (pp. 55–90, 767–780); Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.