Severe acute malnutrition supplements
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of supplements used in Severe Acute Malnutrition (SAM):
Severe Acute Malnutrition — Supplements & Therapeutic Foods
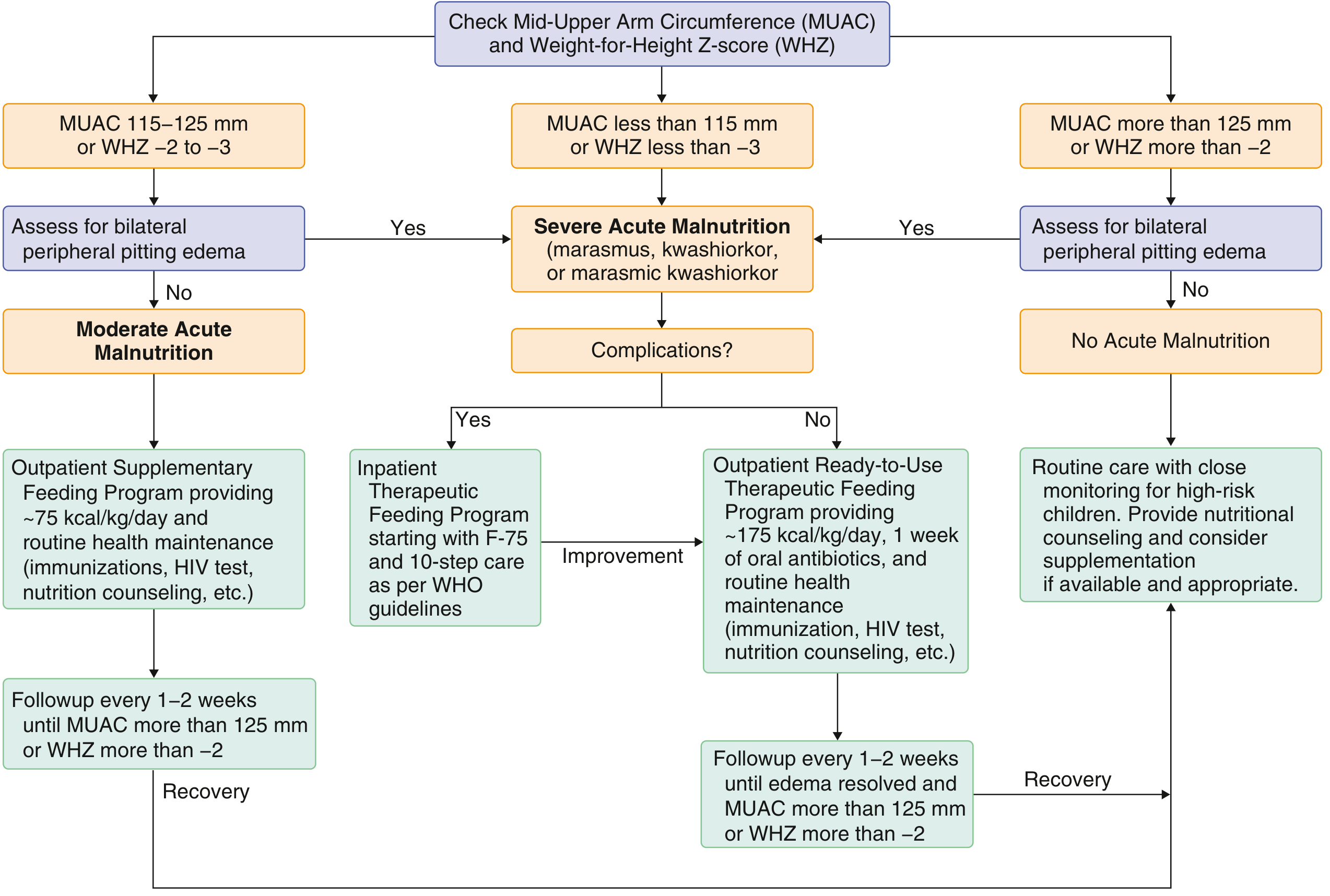
Diagnosis Criteria (WHO)
SAM is defined by:
- Weight-for-height Z-score < −3, or
- MUAC < 115 mm, or
- Presence of bilateral nutritional oedema
Assessment & Treatment Algorithm
Therapeutic Foods
There are three main therapeutic food formulas used in SAM management. Their nutritional compositions per the WHO protocol are:
| Nutrient | F-75 (100 mL) | F-100 (100 mL) | RUTF (100 g) |
|---|---|---|---|
| Energy (kcal) | 75 | 100 | 543 |
| Protein (g) | 0.9 | 2.9 | 13.6 |
| Lactose (g) | 1.3 | 4.2 | — |
| Potassium (mg) | 156 | 246 | 1111 |
| Sodium (mg) | 14 | 44 | 189 |
| Magnesium (mg) | 10.5 | 17.7 | 92 |
| Zinc (mg) | 2 | 3 | 11 |
F-75 (75 kcal/100 mL): Used in the initial/stabilisation phase for inpatient complicated SAM. Low protein and sodium to avoid overloading a metabolically fragile child.
F-100 (100 kcal/100 mL): Used in the rehabilitation/catch-up phase after stabilisation. Higher protein and energy density to rebuild lean mass.
RUTF — Ready-to-Use Therapeutic Food (e.g., fortified peanut paste): The standard for uncomplicated outpatient SAM. Provides ~175 kcal/kg/day. The child ingests approximately 30 g under directly observed therapy to confirm tolerability before outpatient discharge.
Key Micronutrient Supplements in SAM
SAM is almost always accompanied by multiple micronutrient deficiencies. Single vitamin/mineral deficiencies are uncommon — they cluster together. The following supplements are routinely provided:
| Micronutrient | Role / Notes |
|---|---|
| Potassium | Severely depleted in SAM; essential to prevent cardiac arrhythmias during re-feeding |
| Magnesium | Depleted; needed for enzyme function, muscle, and heart |
| Zinc | Critical for immune function, wound healing, growth; deficiency worsens diarrhoea |
| Vitamin A | Routine supplementation recommended; deficiency causes blindness and immune suppression |
| Folic acid | Commonly deficient; given especially when anaemia is present |
| Iron | Added only in the rehabilitation phase (NOT in the stabilisation phase — can worsen oxidative stress and infection) |
| Multivitamins | Broad-spectrum deficiency is expected; a combined multivitamin supplement is standard |
Antibiotic Supplementation
Even in uncomplicated SAM, 1 week of empiric oral antibiotics is recommended alongside RUTF — this has been shown to:
- Decrease mortality
- Improve nutritional recovery
- Decrease need for hospitalisation
Inpatient (Complicated SAM) — WHO 10-Step Protocol
Priorities on admission:
- Treat hypoglycaemia
- Treat hypothermia
- Treat dehydration (using ReSoMal, not standard ORS)
- Correct electrolyte imbalances
- Treat infections
- Correct micronutrient deficiencies (no iron initially)
- Begin cautious re-feeding (F-75)
- Transition to catch-up growth (F-100)
- Provide sensory stimulation and emotional support
- Prepare for discharge and follow-up
Monitoring & Recovery
- Outpatient: Follow up every 1–2 weeks until MUAC > 125 mm or WHZ > −2
- Inpatient: Transition to outpatient once complications resolve
- Community-based management outcomes are generally superior to inpatient care, and are the current international standard
— Goldman-Cecil Medicine, International Edition | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.