Recurrent Laryngeal Nerve Anatomy, variations, and identification during Thyroid Surgery, MS ENT university - exam format for 20 marks also add a note on prevention of Recent Laryngeal nerve damage for 10 marks. as per standard ENT textbooks.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive 30-mark answer. Let me compose the full university exam-format response.
RECURRENT LARYNGEAL NERVE - ANATOMY, VARIATIONS, AND IDENTIFICATION DURING THYROID SURGERY
MS ENT University Examination | Total: 30 Marks
(20 Marks: Anatomy, Variations, Identification | 10 Marks: Note on Prevention of RLN Damage)
PART A: ANATOMY, VARIATIONS, AND IDENTIFICATION DURING THYROID SURGERY [20 Marks]
1. EMBRYOLOGICAL BASIS AND ORIGIN [2 Marks]
The Recurrent Laryngeal Nerve (RLN) is the principal motor and sensory nerve to the larynx. Its asymmetric course on the two sides arises from the embryological fate of the 6th aortic arch:
- Right RLN: The right 6th arch regresses, leaving the nerve looping around the right subclavian artery (4th arch derivative). It arises from the right vagus (CN X) at the level of the right subclavian artery, hooks posterior to it, and ascends obliquely into the neck.
- Left RLN: The left 6th arch persists as the ductus arteriosus/ligamentum arteriosum. The left RLN arises from the left vagus at the level of the aortic arch, loops posterior to the arch at the level of the ligamentum arteriosum, and ascends more vertically in the tracheoesophageal (TE) groove.
Developmental abnormalities of the aortic arch directly determine RLN position - this is the embryological basis of the non-recurrent laryngeal nerve (NRLN).
(Mulholland & Greenfield's Surgery, 7e; Scott-Brown's ORL H&N Surgery)
2. SURGICAL ANATOMY OF THE RLN [6 Marks]
2a. Course in the Neck
| Feature | Right RLN | Left RLN |
|---|---|---|
| Origin | At level of right subclavian artery | At level of aortic arch |
| Course | More oblique, lateral position | More vertical, medial in TE groove |
| Variability | More anatomically variable | More consistent |
| Tracheoesophageal groove | May lie anterior or lateral to groove | Lies consistently in TE groove |
From the mediastinum, both nerves ascend posterior to the common carotid artery and the thyroid gland, lying within or immediately adjacent to the tracheoesophageal groove. The right nerve, because of its more oblique angle of ascent, carries greater anatomic variability in its relationship to surrounding structures.
(Current Surgical Therapy, 14e)
2b. Relationship to the Inferior Thyroid Artery
This is one of the most surgically important - and variable - anatomical relationships. Multiple patterns have been described:
- Deep/posterior to ITA - most common (~60%)
- Anterior to ITA - at risk during medial retraction of thyroid lobe (~20%)
- Between branches of ITA - branched vessels interdigitate with nerve (~20%)
Nerves anterior to the inferior thyroid artery are at particularly high risk of injury as they are drawn anteriorly with medial retraction of the thyroid lobe. Anatomic variations are more common on the right. (Current Surgical Therapy, 14e)
2c. Relationship to the Ligament of Berry
The ligament of Berry is a condensation of the pretracheal fascia that firmly attaches the thyroid to the trachea posteromedially. The RLN is most vulnerable at this point - it passes either just medial or deep to this ligament before inserting into the cricothyroid muscle/cricopharyngeus. The three most common sites of inadvertent injury are:
- Posterior to the inferior pole of the thyroid
- At the intersection with the inferior thyroid artery
- Behind the ligament of Berry (Current Surgical Therapy, 14e)
2d. Relationship to the Tubercle of Zuckerkandl
The tubercle of Zuckerkandl is a posterior thickening of thyroid tissue representing fusion of the lateral thyroid anlage. It serves as an important surgical landmark - the RLN lies just medial and posterior to it (see Figure 75.3B/C below). It must be mobilized laterally and lifted anteromedially to expose the nerve fissure.
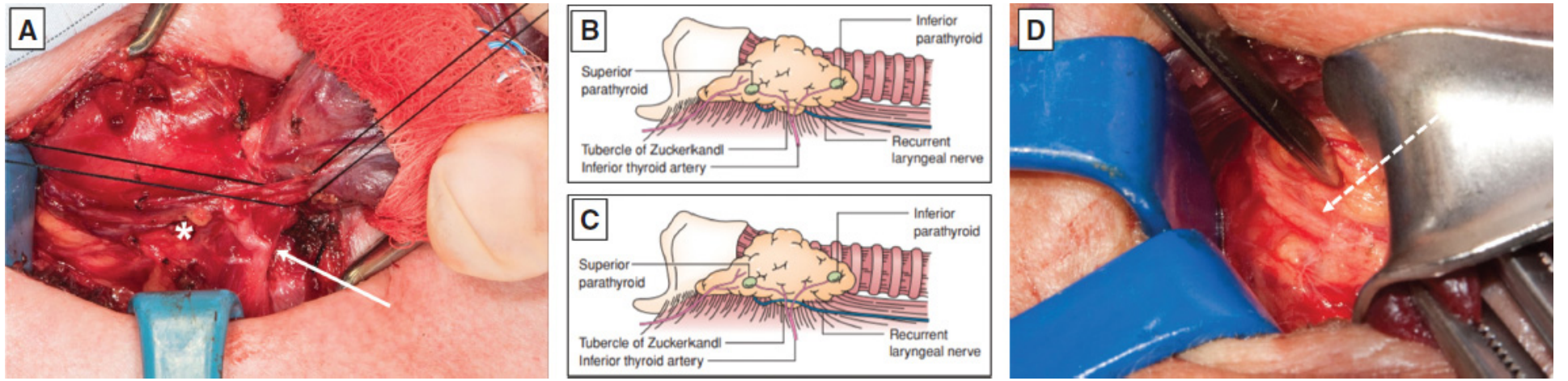
Fig 75.3 - RLN course variations at thyroidectomy. (A) Standard course with superior parathyroid preserved (star). (B) RLN passes medial and posterior to tubercle. (C) RLN lateral to enlarged tubercle. (D) Non-recurrent laryngeal nerve (dashed arrow). - Mulholland & Greenfield's Surgery, 7e
2e. Branching and Extralaryngeal Divisions
Up to 30-34% of RLNs branch before entering the larynx (extralaryngeal branching). When this occurs:
- Anterior branch carries motor fibres (abductor and adductor function)
- Posterior branch carries sensory fibres; injury causes aspiration
This branching may occur significantly proximal to the cricothyroid muscle, such that two separate nerve trunks may be identified within the surgical field. This is a major source of incomplete identification and inadvertent injury. (Scott-Brown's ORL, Vol 1; Mulholland, 7e)
2f. Motor and Sensory Function
The RLN supplies all intrinsic muscles of the larynx except the cricothyroid (which is supplied by the external branch of the superior laryngeal nerve). Specifically:
- Motor: Posterior cricoarytenoid (only abductor), lateral cricoarytenoid, transverse/oblique arytenoids, thyroarytenoid, vocalis
- Sensory: Subglottic mucosa
3. ANATOMICAL VARIATIONS OF THE RLN [5 Marks]
3a. Non-Recurrent Laryngeal Nerve (NRLN)
This is the most dangerous variant - the nerve runs a near-horizontal, direct course from the vagus to the larynx without looping in the mediastinum, making it susceptible to being mistaken for another structure and transected.
| Feature | Right NRLN | Left NRLN |
|---|---|---|
| Incidence | Up to 1.6% of patients | Extremely rare |
| Vascular association | Retroesophageal right subclavian artery (arteria lusoria) | Right aortic arch (situs inversus) |
| CT finding | Absent brachiocephalic trunk on right | Situs inversus |
| Risk of injury | 12.9% - significantly elevated | Similar |
| Course | Near-transverse trajectory behind thyroid | Mirrors right NRLN |
(Mulholland & Greenfield's Surgery, 7e; Current Surgical Therapy, 14e)
Preoperative identification: When CT chest/neck shows aberrant subclavian artery or absent brachiocephalic trunk, suspect NRLN. Surgeon-performed ultrasound can identify aberrant neck vasculature with high accuracy (median 5 minutes examination time) and is recommended as a cost-effective screening tool.
3b. Relationship to the ITA - Variations
As described above (Section 2b), the nerve may be found anterior, posterior, or between branches of the inferior thyroid artery. Anterior position is particularly hazardous.
3c. Extralaryngeal Branching
Occurs in 30-34% of cases. Branches may arise well below the level of the cricothyroid muscle and diverge significantly within the surgical field. Both branches must be identified and preserved. (Scott-Brown's ORL, Vol 1)
3d. High Bifurcation
Rarely, the nerve bifurcates so proximally that two distinct trunks are visible throughout the tracheoesophageal groove. This is a trap for the unwary surgeon who, having identified one trunk, assumes the nerve is preserved while inadvertently damaging the other.
3e. Position Relative to TE Groove
The RLN may not always lie within the TE groove - it can be found anterior or lateral to the tracheoesophageal groove, especially on the right side. Expecting the nerve exclusively within the groove leads to missed identification.
4. IDENTIFICATION OF THE RLN DURING THYROID SURGERY [7 Marks]
4a. Importance of Identification
Direct visualization of the RLN is the gold standard for its protection during thyroidectomy. Incidence of permanent RLN paralysis is approximately 1-2% with thyroid surgery; temporary dysfunction occurs in at least 2-5%. The incidence of permanent injury rises in revision procedures, malignancy, and neck dissection cases. (Cummings Otolaryngology, H&N Surgery)
4b. Landmarks for Identification
Behr's Triangle (Lateral Approach) - Most Reliable:
This is the standard and safest landmark for RLN identification. The triangle is bounded by:
- Superiorly: Inferior thyroid artery
- Medially: Trachea
- Laterally: Common carotid artery
The RLN is identified in the lower lateral part of the neck within this triangle. It should be found before ligating the inferior thyroid artery. (Scott-Brown's ORL, Vol 1)
Technique: Spread perpendicular to the expected nerve axis through the fatty and nodal tissue posterior to the thyroid gland to initially expose the nerve. Once identified, use a blunt hemostatic clamp with the tip upward to separate the nerve from superficial structures along its course. (Current Surgical Therapy, 14e)
4c. Approach Options
1. Lateral/Standard Approach (preferred)
- Identify RLN at the level of the inferior pole within Behr's triangle
- Trace nerve superiorly to the ligament of Berry
- Safest for routine cases
2. Superior/Cricothyroid Approach
- Identify the nerve at the cricothyroid junction (point of laryngeal entry)
- Once identified, dissect caudally using the "toboggan technique": tunnelling tissue with a fine-tip mosquito dissector, then dividing the overlying tissue with bipolar diathermy
- Useful in: cancer patients with nodal disease, reoperative surgery, failed lateral approach, suspected NRLN (Scott-Brown's ORL, Vol 1)
3. Inferior Pole Approach
- Expose nerve at the inferior pole before committing to any vascular ligation
4d. Intraoperative Neuromonitoring (IONM)
IONM has expanded in popularity as a useful adjunct to facilitate RLN identification and real-time assessment of nerve function. It uses:
- A specialized endotracheal tube electrode positioned at the level of the vocal cords
- A handheld probe to intermittently stimulate the vagus or RLN
- Auditory or visual electromyographic (EMG) signals indicating nerve integrity
Important caveat: Routine use of IONM has not been definitively shown to decrease rates of RLN injury compared to visual identification alone. However, it facilitates:
- Intraoperative nerve identification
- Recognition of nerve irritation (signal loss = warning)
- Surgical decision-making regarding contralateral exploration if ipsilateral nerve injury is detected
- Medicolegal documentation
IONM requires general anesthesia (neuromuscular blockade must be reversed), incurs additional cost, and requires surgeon/team familiarity. Visual identification remains the gold standard. (Current Surgical Therapy, 14e; Scott-Brown's ORL, Vol 1)
4e. Characteristics of the RLN at Surgery
The nerve can be identified by its characteristic features:
- White, cord-like structure (whiter than surrounding tissues)
- Palpable "snap" when plucked with a dissector (unlike blood vessels)
- Branching pattern (may show multiple small fascicles)
- Non-pulsatile (distinguishes from ITA)
- Lies within or near the TE groove, just posterior to the thyroid capsule
- IONM probe will elicit vocal fold movement on stimulation (0.5-2 mA)
4f. Consequences of Injury
| Injury | Presentation |
|---|---|
| Unilateral RLN injury | Ipsilateral vocal cord in paramedian position; breathy, low-volume voice that fatigues easily |
| Bilateral RLN injury | Immediate stridor and dyspnea; potential airway emergency; cords move to midline over time |
| Concurrent SLN + RLN injury | More laterally positioned cord; worsened voice quality and glottic competence; aspiration risk |
If the nerve is transected, microsurgical repair (re-anastomosis) is recommended. Although full function restoration is unlikely, it maintains some vocal cord tone and reduces atrophy. Ansa cervicalis-to-RLN anastomosis prevents laryngeal synkinesis. (Cummings ORL, H&N Surgery)
PART B: NOTE ON PREVENTION OF RECURRENT LARYNGEAL NERVE DAMAGE [10 Marks]
PREVENTION OF RLN DAMAGE DURING THYROID SURGERY
Prevention of RLN injury is central to safe thyroid surgery and requires a systematic, multi-layered approach.
1. PREOPERATIVE MEASURES [2 Marks]
a. Preoperative Laryngoscopy (Mandatory)
Vocal cord function must be evaluated and documented by indirect laryngoscopy or flexible fiberoptic laryngoscopy before surgery in all patients - especially those who have had previous neck surgery. This establishes a baseline and allows informed consent regarding the small but real risk of voice change.
b. Imaging Review
- Review all available CT scans of the neck and chest for aberrant vascular anatomy (absent brachiocephalic trunk on the right = suspect NRLN)
- Preoperative ultrasound by the surgeon can correctly identify absent brachiocephalic trunk and predict NRLN with minimal examination time
c. Surgeon Experience and Volume
- Thyroid surgery should be performed by, or under supervision of, experienced thyroid surgeons. Risk of permanent RLN injury is directly correlated with surgical volume.
d. Patient Selection and Counseling
- Risk-stratify patients: recurrent thyroid carcinoma, substernal goiter, thyroiditis, and revision surgery carry elevated risk; patients should be counseled explicitly
(Mulholland & Greenfield's Surgery, 7e; Cummings ORL H&N Surgery)
2. INTRAOPERATIVE MEASURES [6 Marks]
a. Routine Visual Identification of the RLN (Cornerstone)
The most effective preventive measure is routine, systematic identification of the RLN in every thyroidectomy. Studies have shown that routine identification reduces permanent RLN palsy compared to surgery without identification. Identification in Behr's triangle before any major vascular ligation is the standard approach.
b. Careful Ligation of the Inferior Thyroid Artery
The ITA should be ligated close to the thyroid capsule (rather than in the main trunk) to preserve parathyroid blood supply and avoid avulsing or compressing the RLN. Never blindly clamp or ligate structures in the TE groove before identifying the nerve.
c. Gentle Tissue Handling - Avoiding the Three Sites of Common Injury
Extra caution is required at:
- Posterior to the inferior pole (initial mobilization)
- At the intersection with the inferior thyroid artery (vascular ligation)
- Behind the ligament of Berry (final dissection step)
At the ligament of Berry, the RLN is vulnerable to pinching during medial retraction of the thyroid gland before dividing the ligament. The nerve should be directly visualized before dividing this ligament.
d. The Tubercle of Zuckerkandl as a Guide
Always identify and mobilize the tubercle of Zuckerkandl. The RLN runs in the fissure immediately medial/posterior to it. Attempting to divide the gland without recognizing this tubercle risks RLN entrapment.
e. Avoidance of Thermal Injury
- Use bipolar diathermy (not monopolar) when working near the nerve
- Keep all heat sources at a safe distance from the nerve (>3 mm from nerve fascicles)
- Avoid prolonged compression from retractors (neuropraxia from ischaemia)
f. Gentle Retraction
Excessive and prolonged medial retraction of the thyroid lobe is a common cause of neuropraxia (stretch injury). Retraction should be intermittent and the minimum force required.
g. Intraoperative Neuromonitoring (IONM) as Adjunct
IONM allows real-time functional assessment and early warning of nerve stress. Although it does not replace visual identification, it:
- Helps identify the nerve faster
- Detects signal changes indicating traction or thermal stress before permanent damage occurs
- Guides decision-making (e.g., staged bilateral thyroidectomy if ipsilateral signal loss detected)
- Particularly valuable in revision, cancer, and substernal goiter cases
h. If the Nerve is Accidentally Transected
Immediate microsurgical re-anastomosis should be performed (end-to-end, with fine sutures under magnification). Alternatively, ansa cervicalis-to-RLN anastomosis prevents synkinesis. Abandon the contralateral thyroid dissection in the same sitting if bilateral injury is suspected, to avoid bilateral cord palsy.
(Current Surgical Therapy, 14e; Scott-Brown's ORL, Vol 1; Cummings ORL H&N Surgery; Mulholland & Greenfield's Surgery, 7e)
3. POSTOPERATIVE MEASURES [2 Marks]
a. Postoperative Laryngoscopy
Formal documentation of vocal cord mobility should be performed in the early postoperative period in all patients who present with voice change or hoarseness after thyroidectomy. If bilateral injury is suspected, immediate airway assessment is mandatory.
b. Management of Established RLN Injury
- Temporary neuropraxia: Supportive management; return of normal function generally occurs within 12 months. Speech therapy is valuable during this period.
- Permanent unilateral paralysis: Serial examinations to document function or contralateral compensation. For persistent vocal incompetence or aspiration: vocal cord medialization options include (1) vocal cord injection, (2) thyroplasty (Type I), (3) arytenoid adduction.
- Bilateral RLN paralysis: Management is directed at improving the airway without completely sacrificing voice. Options: arytenoidectomy, transverse cordotomy (posterior), or tracheostomy in acute airway compromise.
c. Documentation and Audit
All thyroid surgeons should audit their personal rates of RLN injury (temporary and permanent) and benchmark against published standards. Permanent RLN palsy rate of <1% is the accepted standard for experienced surgeons.
(Cummings Otolaryngology H&N Surgery; Mulholland & Greenfield's Surgery, 7e)
SUMMARY TABLE: Prevention Strategy at a Glance
| Phase | Key Action |
|---|---|
| Preoperative | Laryngoscopy; imaging review for NRLN; patient counselling |
| Intraoperative | Routine visual RLN identification in Behr's triangle; ligate ITA close to capsule; avoid heat/traction; IONM as adjunct; protect at 3 danger zones |
| Postoperative | Laryngoscopy for voice change; speech therapy; medialization procedures if needed |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1 (Ch. 67) - RLN identification approaches, Behr's triangle
- Mulholland & Greenfield's Surgery: Scientific Principles and Practice, 7e (Ch. 75) - RLN anatomy, NRLN, tubercle of Zuckerkandl, embryology
- Cummings Otolaryngology Head and Neck Surgery - RLN injury incidence, consequences, management
- Current Surgical Therapy, 14e - Preservation of RLN, IONM, intraoperative technique
- Fischer's Mastery of Surgery, 8e - RLN-ITA relationships
minimally invasive Thyroid Surgery & Endoscopic thyroidectomy. MS ENT university exam format for 10 marks each. as per standard textbooks
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Scott-Brown's, Sabiston, Schwartz, and Current Surgical Therapy. Let me now compose the full exam-format answer.
MINIMALLY INVASIVE THYROID SURGERY & ENDOSCOPIC THYROIDECTOMY
MS ENT University Examination
10 Marks Each | Total: 20 Marks
QUESTION 1: MINIMALLY INVASIVE THYROID SURGERY [10 Marks]
1. INTRODUCTION AND HISTORICAL BACKGROUND [1 Mark]
The principles of safe thyroid surgery were established by Theodor Kocher at the beginning of the 20th century, earning him the Nobel Prize in 1909. For nearly a century, the technique remained largely unchanged. The key driver for minimally invasive thyroid surgery (MITS) is patient demand for improved cosmesis - studies show 71% of patients in thyroid clinics would prefer not to have a visible neck scar, independent of sex or skin colour.
Technological enablers - development of the endoscope, energy-sealing devices (harmonic/bipolar), and high-definition cameras - provided the prerequisites for small-incision thyroidectomy techniques.
(Scott-Brown's ORL H&N Surgery, Vol 1 - Ch. 69, Tolley)
2. CLASSIFICATION OF MINIMALLY INVASIVE APPROACHES [2 Marks]
Minimally invasive thyroid surgery is broadly divided into:
A. Minimally Invasive Cervical Approaches (scar remains in the neck but is smaller)
- Minimally Invasive Video-Assisted Thyroidectomy (MIVAT / Miccoli technique)
- Minimally Invasive Thyroidectomy (MIT)
- Endoscopic-Assisted Thyroidectomy (EAT)
- Henry technique (gas insufflation, lateral ports)
B. Scarless-in-the-Neck / Remote Access Approaches (incision placed away from neck)
- Transaxillary approach (gasless or CO2 insufflation)
- Bilateral Axillo-Breast Approach (BABA)
- Axillo-Bilateral-Breast Approach (ABBA)
- Facelift / Retroauricular approach
- Transoral Endoscopic / Robotic approaches (see Question 2)
C. Robotic-Assisted Thyroidectomy (RAT)
(Scott-Brown's ORL; Sabiston Textbook of Surgery)
3. MICCOLI TECHNIQUE (MIVAT) [2 Marks]
Pioneered by Paolo Miccoli in Pisa, this is the most widely validated minimally invasive cervical technique.
Key features:
- Incision: 2-3 cm midline cervical incision
- Gas-free (gasless) - no CO2 insufflation required
- Endoscopic dissection of the superior pole through the small incision; gland then delivered into the neck through the same incision
- Lower pole dissection and completion of thyroidectomy performed conventionally once the lobe is delivered
- Uses a 30-degree 4 mm endoscope with specialized Miccoli instruments: suction dissectors, spatulas, and purpose-designed retractors
- Requires two competent assistants and a video stack
- Total thyroidectomy is possible through a single incision
Indications (strict patient selection):
- Solitary nodules up to 3 cm
- Total thyroid lobe volume not exceeding 20 mL (nodule volume ≤14 mL)
- Selected Graves' disease and thyroid cancer in expert hands
- Patients with tendency to hypertrophic/keloid scarring
Contraindications:
- Prior thyroiditis, previous neck surgery, large goitre
- Confirmed malignancy with nodal disease (relative)
Advantages:
- Superior cosmesis vs. conventional thyroidectomy
- Excellent visualization of RLN, external laryngeal nerve, and parathyroids
- No risk of CO2 insufflation complications
- Comparable complication rates to conventional thyroidectomy
Limitations:
- Steep learning curve: >50 cases required for expert status
- Requires high-volume thyroid practice
- Suitable for only ~8% of UK thyroid surgical practice
- Two trained assistants mandatory
- Excessive traction through small incision can paradoxically cause hypertrophic scarring
(Scott-Brown's ORL, Vol 1; Schwartz's Principles of Surgery, 11e)
4. HENRY TECHNIQUE (GAS INSUFFLATION) [1 Mark]
Pioneered by Jean-François Henry in Marseille, this technique uses CO2 insufflation to create the working space:
- Three lateral ports along the anterior border of the sternomastoid muscle: two 3 mm instrument ports + one 1 cm port for the insufflating endoscope
- CO2 at 8 mmHg creates operative space and achieves a relatively bloodless field
- An assistant holds and manipulates the endoscope while dissection proceeds
- Delivery of the thyroid lobe is through the endoscope port on completion
- Technically more challenging than the Miccoli method
- Total thyroidectomy is not possible by this method
- More suited to parathyroidectomy; not widely adopted for thyroidectomy
(Scott-Brown's ORL H&N Surgery, Vol 1)
5. REMOTE ACCESS / SCARLESS-IN-THE-NECK APPROACHES [2 Marks]
These techniques place the incision away from the visible neck, typically driven by cultural factors (particularly in East Asia, where a horizontal neck scar carries negative cultural connotations).
Transaxillary Approach:
- Originated in Japan (2000); popularized in South Korea (Chung et al., Yonsei University)
- A single incision in the axilla with 3 ports (12 mm + 5 mm + 5 mm)
- Subcutaneous tunnel dissected to the neck, sternothyroid muscle split to expose thyroid
- Performed gasless (with custom long tunnelled retractors) or with CO2 insufflation
- Robotic assistance (da Vinci) has been the dominant modality for this approach in South Korea - >3000 cases published by 2013
- Complications: brachial plexus injury, tracheoesophageal injury, lymph leak (especially during early adoption phase - FDA warnings issued in 2013 due to initial upsurge of US complications)
- Recent US experience (301 cases): 1.3% permanent RLN injury, 1.1% permanent hypoparathyroidism
Bilateral Axillo-Breast Approach (BABA/ABBA):
- Ports in both axillae and bilateral periareolar sites
- Permits bimanual instrument work and total thyroidectomy
- Both gasless and insufflation techniques used; CO2 insufflation risks hypercarbia
- Steep learning curve; requires a competent assistant working with 2D view
(Scott-Brown's ORL, Vol 1; Sabiston Textbook of Surgery)
6. EVIDENCE BASE AND PATIENT SELECTION [1 Mark]
Meta-analyses (Radford et al.) of MIVAT showed:
- Complication rates no higher than conventional thyroidectomy
- Superior cosmetic outcomes in the early postoperative period
- Longer operative time compared to conventional thyroidectomy
- Long-term scar satisfaction may not differ significantly after 18 months once full healing is complete (little/no difference in long-term scar satisfaction)
For safe practice:
- Large-volume thyroid practice (>50 procedures per year) is essential
- 86% of BAETS members perform fewer than 50 thyroidectomies/year - hence low adoption in the UK
- Prospective long-term cohort studies comparing MIT to conventional thyroidectomy are still lacking
(Scott-Brown's ORL, Vol 1)
7. SUMMARY TABLE [1 Mark]
| Feature | Miccoli (MIVAT) | Henry | Transaxillary (Robotic) |
|---|---|---|---|
| Incision site | 2-3 cm neck (midline) | Lateral neck (3 ports) | Axilla |
| Gas insufflation | No (gasless) | Yes (CO2 8 mmHg) | Optional |
| Total thyroidectomy | Yes | No | Yes |
| Neck scar | Yes (small) | Yes (lateral) | No |
| Learning curve | >50 cases | Very steep | Very steep |
| Robotic | No | No | Yes (da Vinci) |
| Main complication risk | Hypertrophic scar | Hypercarbia | Brachial plexus injury |
QUESTION 2: ENDOSCOPIC THYROIDECTOMY [10 Marks]
1. DEFINITION AND RATIONALE [1 Mark]
Endoscopic thyroidectomy refers to thyroid surgery performed entirely or partially using an endoscope (with or without robotic assistance), placing the incision at a remote site away from the neck to completely avoid a cervical scar. The core principle distinguishing endoscopic from minimally invasive cervical approaches is the creation of a subcutaneous working space by dissecting a tunnel from a distant incision site to the thyroid, using either gasless retraction or CO2 insufflation.
This is more accurately termed "scarless in the neck" rather than truly minimally invasive, since the total extent of tissue dissection is often significantly greater than conventional thyroidectomy.
(Scott-Brown's ORL, Vol 1; Sabiston Textbook of Surgery)
2. APPROACHES [3 Marks]
A. Transoral Endoscopic Thyroidectomy Vestibular Approach (TOETVA)
The most recently developed and only truly scarless (no skin incision whatsoever) approach.
Technique:
- Popularized in Thailand by Anuwong (largest series: 425 patients)
- Three laparoscopic ports placed in the oral vestibule (lower lip mucosa):
- One 10-12 mm central port for the camera
- Two 5 mm lateral ports for instruments
- CO2 gas insufflation at 6 mmHg creates a subplatysmal working space
- Dissection proceeds through the subplatysmal plane in the neck down to the thyroid
- The thyroid is extracted through the central oral vestibular port
FIGURE 73.36 - Transoral endoscopic thyroidectomy vestibular approach (TOETVA). Three laparoscopic ports placed in the oral vestibule, dissection carried to subplatysmal plane. - Sabiston Textbook of Surgery
Indications (consensus criteria for early adoption):
- Benign thyroid nodules ≤6 cm
- Well-differentiated thyroid cancer (papillary) without lateral nodal disease
- No prior neck surgery or infection
- Patient motivated for scarless surgery and accepts longer operative time
Results (Anuwong, 425-patient series):
- Zero permanent RLN injury
- Zero permanent hypoparathyroidism
- 3 intraoperative conversions to open
- 0.7% transient mental nerve palsy (approach-specific complication)
- No postoperative infections
Robotic variant (TORT - Transoral Robotic Thyroidectomy):
- Single-port or multiport robotic approach via oral vestibule
- da Vinci Single Port (SP) system used
- Better instrument articulation in confined transoral space
- Shorter working distance; steeper setup learning curve
(Sabiston Textbook of Surgery; Current Surgical Therapy, 14e)
B. Robotic-Assisted Thyroidectomy (RAT) - Transaxillary Robotic Approach
Historical development:
- Lobe et al. (2005) - first reported da Vinci lobectomy with insufflation
- Chung and colleagues, Yonsei University, Seoul - pioneers of transaxillary RAT; >3000 cases by 2013
- First adopted in USA with subsequent FDA warnings (2013) due to complications from inadequate training
The da Vinci System - Components:
- Surgeon console - remote workstation with 3D binocular viewer; surgeon controls instruments via hand cradles and foot pedals; infrared sensors halt movement if surgeon leaves console
- Patient-side cart - 4 arms: one camera arm + 3 instrument arms; docks to patient through process of 'docking'
- Vision stack - dual CCDs, 3D imaging (two 8 mm/12 mm endoscopes providing true stereoscopic depth)
Key technological advantages:
- Tremor filtration - algorithms remove natural hand tremor
- Motion scaling - console movements scaled to finer operative field movements
- EndoWrist - 7 degrees of freedom (vs. 4 degrees for human hand); 270-degree arc rotation in both directions
- 3D HD visualization - true depth perception (vs. flat 2D in conventional endoscopy)
- Equal dexterity with dominant and non-dominant hands
Applications in thyroid surgery:
- Hemithyroidectomy, lobectomy, total thyroidectomy
- Central compartment (level VI) neck dissection
- Lateral compartment neck dissection via axillary approach
Safety data:
- Meta-analysis (2013): complication rates including RLN palsy and hypocalcaemia rates comparable to conventional thyroidectomy
- However: high heterogeneity, heavy weighting from pioneer Korean units, and publication bias (complications under-reported)
(Scott-Brown's ORL H&N Surgery, Vol 1 - Ch. 69)
C. Anterior Chest Wall / Breast Approach (Endoscopic)
- Two 5 mm trocars below the ipsilateral clavicle + 12 mm trocar at anterior chest wall ~3-5 cm below clavicle border
- CO2 insufflation at 4 mmHg
- Anterior border of SCM separated from sternohyoid muscle
- Sternothyroid muscle split to expose thyroid
- Lower pole retracted upward; RLN identified; Berry's ligament divided with laparoscopic coagulating shears
- Upper pole freed from cricothyroid muscle; gland extracted through the chest port
(Schwartz's Principles of Surgery, 11e)
3. PATIENT SELECTION - GENERAL PRINCIPLES FOR ALL ENDOSCOPIC APPROACHES [2 Marks]
Suitable candidates:
- Motivated patients who specifically wish to avoid a visible neck scar
- Benign thyroid pathology (nodule, Graves' disease) - well-defined criteria per approach
- Well-differentiated thyroid cancer without gross nodal/extrathyroidal disease (in high-volume centres only)
- BMI within acceptable range (obesity increases risk and reduces working space)
- No prior neck surgery or radiation
Contraindications:
- Large goitre (>6 cm nodule / total volume unsuitable for extraction)
- Gross extrathyroidal extension or lateral nodal metastases
- Previous neck surgery (scar tissue obliterates planes)
- Thyroiditis (fibrotic planes)
- Substernal extension
- Patient unable to accept longer operative time and higher cost
4. COMPLICATIONS [2 Marks]
General complications (shared with conventional thyroidectomy):
- RLN injury (transient/permanent)
- Hypocalcaemia / hypoparathyroidism
- Haematoma, wound infection
Approach-specific complications:
| Approach | Unique Complications |
|---|---|
| Transaxillary (all) | Brachial plexus injury, tracheoesophageal injury, arm lymphedema, seroma |
| BABA / ABBA (breast) | Breast skin flap devascularization, chest wall seroma, medial nerve injury |
| Facelift / retroauricular | Marginal mandibular nerve injury, alopecia, skin flap devascularization |
| Transoral (TOETVA/TORT) | Mental nerve palsy (transient), oral wound infection, submental skin flap injury, CO2 embolism |
| CO2 insufflation (all) | Hypercarbia, CO2 embolism, subcutaneous emphysema |
(Sabiston Textbook of Surgery; Scott-Brown's ORL, Vol 1)
5. CURRENT STATUS AND LIMITATIONS [1 Mark]
Advantages over conventional open thyroidectomy:
- No visible neck scar (true scarless in TOETVA)
- 3D magnified field in robotic approaches (improved nerve/parathyroid identification)
- Potentially better postoperative cosmesis and patient satisfaction
Limitations:
- Longer operative time than conventional thyroidectomy in all series
- Greater total tissue dissection (more invasive in total extent)
- Steep learning curve - requires structured training and credentialing
- Cost - robotic systems (da Vinci) add substantial operative cost; reimbursement tariffs vary widely
- Limited evidence: No definitive RCT showing superiority over conventional thyroidectomy in clinical outcomes
- Ethical concern: Most Korean robotic thyroidectomy data involve microcarcinomas (mean 8 mm) - risk-benefit ratio for this pathology is debatable
- Restricted adoption: FDA warnings (2013) led to retraction of active industry support for robotic thyroidectomy; currently confined to high-volume, specialized centers
- ATA guidelines state: clear benefits over traditional open approach via small neck incisions have not yet been established
(Scott-Brown's ORL, Vol 1; Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery)
SUMMARY COMPARISON TABLE
| Feature | MIVAT (Miccoli) | TOETVA | Robotic (Transaxillary) |
|---|---|---|---|
| Neck scar | Small (2-3 cm) | None | None |
| Access route | Neck midline | Oral vestibule | Axilla |
| Insufflation | No | CO2 | No (gasless) / CO2 |
| Instruments | Endoscopic | Laparoscopic | Robotic (da Vinci) |
| 3D vision | No | No | Yes |
| Total thyroidectomy | Yes | Yes | Yes |
| Learning curve | >50 cases | Steep | Very steep |
| Unique risk | Hypertrophic scar | Mental nerve palsy | Brachial plexus injury |
| Adoption | Moderate (Europe) | Growing (Asia, USA) | Declining post-FDA 2013 |
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1 - Ch. 69 (Tolley): MIVAT, Miccoli, Henry, Robotic Thyroidectomy
- Sabiston Textbook of Surgery, 21e - Ch. 73: Alternative approaches to thyroidectomy, TOETVA
- Schwartz's Principles of Surgery, 11e - Ch. 38: Minimally invasive approaches, anterior chest technique
- Current Surgical Therapy, 14e - Technical considerations and IONM
This is a shared conversation. Sign in to Orris to start your own chat.