Pharmacotherapy of Hypothyroidism
"hypothyroidism"[MeSH Terms] AND "levothyroxine"[MeSH Terms]
"hypothyroidism" AND "treatment" AND "thyroxine"
Pharmacotherapy of Hypothyroidism
Overview
1. Drug of Choice: Levothyroxine (T4)
- Consistent, predictable potency and chemical stability
- Long plasma half-life (~7 days), enabling once-daily dosing
- Peripheral conversion by deiodinases (Dio1, Dio2) to active T3 closely mimics normal physiology
- Approximately 20% of circulating T3 normally derives directly from the thyroid; the remainder comes from peripheral conversion - levothyroxine monotherapy maintains this via tissue deiodination
2. Pharmacokinetics
| Parameter | Details |
|---|---|
| Bioavailability | 60-80% when taken fasted; food delays absorption |
| Time to peak | ~2 hours (fasting); may be prolonged to 3 hours in hypothyroid state |
| Plasma half-life | ~7 days (due to extensive protein binding to TBG, TBPA, albumin) |
| Metabolism | Peripheral deiodination to T3 (active) or rT3 (inactive); hepatic conjugation |
| Steady state | Reached in 6-8 weeks after a consistent dose |
| Route | Oral (standard); IV available for emergencies |
3. Dosing
Standard Adult Dosing
- Average full replacement dose: ~1.7 mcg/kg/day (approximately 125 mcg/day for a 70 kg adult)
- Older adults (>65 years): ~1.6 mcg/kg/day; lower lean body mass reduces requirement
- Post-thyroidectomy TSH suppression (thyroid cancer): ~2.2 mcg/kg/day
Age-Specific Dosing
| Age Group | Dose (mcg/kg/day) |
|---|---|
| Neonates / Infants (1-6 months) | 10-15 |
| Children (6-12 months) | 6-8 |
| Children (1-5 years) | 5-6 |
| Children (6-12 years) | 4-5 |
| Adolescents (>12 years) | 2-3 |
| Adults | ~1.7 |
| Elderly (>65 years) | ~1.6 (or ~0.5 mcg/kg/day per some guidelines) |
Initiating Therapy
- Younger patients / mild disease: Full replacement dose can be started immediately
- Patients >50 years, no cardiac disease: Start at 50 mcg/day
- Elderly / long-standing hypothyroidism / cardiac disease: Start at 12.5-25 mcg/day, increase by 12.5-25 mcg every 2 weeks until euthyroid or toxicity occurs
In patients with coronary artery disease, low thyroid hormone levels paradoxically protect the heart from increased oxygen demand. Overly rapid correction can provoke angina, arrhythmia, or MI. Coronary revascularization should precede aggressive T4 replacement if indicated.
4. Monitoring
| Primary Hypothyroidism | Central (Secondary/Tertiary) Hypothyroidism |
|---|---|
| Serum TSH (most reliable) | Free T4 (TSH unreliable) |
| Target TSH: 0.5-2.5 mIU/L | Maintain free T4 in upper half of reference range |
| Recheck TSH 6-8 weeks after any dose change |
- Children: Monitor for normal growth and development
- Elderly: Monitor for atrial fibrillation and bone mineral density (chronic overtreatment accelerates osteoporosis)
5. Administration Pearls
- Optimal: Take on an empty stomach, 30-60 minutes before breakfast, or at bedtime (4 hours after last meal)
- Avoid co-administration with: calcium supplements, iron salts, proton pump inhibitors, antacids, cholestyramine, soy, bran, coffee - all reduce absorption
- Administer at least 4 hours apart from prenatal vitamins and calcium in pregnant patients
Conditions Requiring Higher Doses
- Malabsorptive states: atrophic gastritis, H. pylori gastritis, celiac disease, lactose intolerance, bariatric surgery
- Pregnancy (see below)
6. Special Clinical Situations
A. Subclinical Hypothyroidism
- TSH >10 mIU/L: Levothyroxine generally recommended, especially in younger patients (<65-70 years)
- TSH <10 mIU/L with symptoms: Consider a trial of levothyroxine; discontinue if symptoms do not improve
- Elderly (>80-85 years) with TSH ≤10 mIU/L: Wait-and-watch strategy recommended (age-related TSH rise may not require treatment)
B. Hypothyroidism in Pregnancy
- Overt hypothyroidism is associated with miscarriage, preterm delivery, fetal distress, and impaired psychoneural development in offspring
- Increase dose by ~25-30% as soon as pregnancy is confirmed (practical tip: two extra tablets per week)
- TSH targets by trimester:
- 1st trimester: 0.1-2.5 mIU/L
- 2nd trimester: 0.2-3.0 mIU/L
- 3rd trimester: 0.3-3.0 mIU/L
- Administer T4 at least 4 hours apart from prenatal vitamins/calcium
- Revert to pre-pregnancy dose the day after delivery; recheck TSH at 6 weeks postpartum
C. Myxedema Coma (Emergency)
- Manage in ICU; may require intubation and mechanical ventilation
- IV Levothyroxine loading dose: 300-400 mcg, then 50-100 mcg IV daily
- Can add IV Liothyronine (T3): 5-20 mcg initially, then 2.5-10 mcg every 8 hours - but T3 is more cardiotoxic and harder to monitor
- IV Hydrocortisone (e.g., 50-100 mg q6-8h) until concomitant adrenal insufficiency is excluded
- Supportive: passive rewarming, ventilation, cautious IV fluids (risk of water intoxication), treat precipitating cause
- Administer all drugs IV (poor GI absorption in myxedema)
D. Congenital Hypothyroidism
- Diagnosis within 2 weeks of life and prompt treatment with levothyroxine results in normal physical and intellectual development
- Delayed diagnosis leads to cretinism (irreversible intellectual disability)
- Doses are weight-based and higher per kg than adults
E. Drug-Induced Hypothyroidism
- If the causative drug can be stopped, thyroid function may recover
- If not, manage with levothyroxine
- Amiodarone: Levothyroxine may be required even after discontinuation, given amiodarone's very long half-life (~40-55 days)
7. Combination T4 + T3 Therapy
- Multiple controlled trials show no consistent superiority of combination therapy
- Limitations acknowledged: trials did not focus on patients who remain symptomatic despite normal TSH/free T4, and no long-acting T3 formulation exists
- Desiccated thyroid extract (DTE) (e.g., Armour Thyroid): contains both T4 and T3 in a ~4:1 ratio; some patients express preference (particularly for weight-related outcomes in crossover studies), but lacks consistent evidence of superiority
- A subgroup with Dio2 Thr92Ala polymorphism (impaired T4-to-T3 conversion) might theoretically benefit - but evidence remains insufficient to guide routine testing
8. Toxicity / Overtreatment
| Adults | Children |
|---|---|
| Nervousness, heat intolerance | Restlessness, insomnia |
| Palpitations, tachycardia | Accelerated bone maturation |
| Unexplained weight loss | Premature craniosynostosis |
| Atrial fibrillation (especially elderly) | |
| Accelerated osteoporosis |
9. Key Drug Interactions with Levothyroxine
| Interaction | Effect |
|---|---|
| Calcium carbonate, iron salts | Reduced T4 absorption (separate by 4h) |
| Cholestyramine, colestipol | Binds T4 in gut, reduces absorption |
| PPIs, sucralfate, antacids | Reduce absorption |
| Rifampin, phenytoin, carbamazepine | Induce hepatic metabolism of T4, increase dose requirement |
| Amiodarone | Inhibits T4→T3 conversion (may cause hypo- or hyperthyroidism) |
| Warfarin | Potentiation of anticoagulation effect |
| Estrogen/oral contraceptives | Increase TBG, may increase dose requirement |
Recent Evidence Note
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Tietz Textbook of Laboratory Medicine, 7th Edition
Pharmacotherapy of Hypothyroidism
"hypothyroidism" AND "treatment" AND "thyroxine"
Pharmacotherapy of Hypothyroidism
Therapeutic Preparations Available
| Preparation | Contents | Key Feature |
|---|---|---|
| Levothyroxine (T4) | Synthetic L-thyroxine | Drug of choice; once-daily dosing |
| Liothyronine (T3) | Synthetic L-triiodothyronine | Faster onset; used in emergencies |
| Desiccated thyroid extract (DTE) | Porcine/bovine T4 + T3 (~4:1) | Historical; occasionally preferred by patients |
1. Levothyroxine - Drug of Choice
Why T4 is Preferred Over T3 or DTE
- Consistent, predictable potency and chemical stability
- Long plasma half-life (~7 days) due to extensive protein binding, enabling once-daily dosing
- Peripheral deiodination (by Dio1 and Dio2 enzymes) converts T4 to active T3 in tissues, maintaining steady free T3 levels - closely mimicking normal physiology
- Multiple controlled trials confirm it is not inferior to combination T4+T3
Note: ~20% of circulating T3 normally derives directly from the thyroid gland; the remaining 80% comes from peripheral T4 deiodination. Levothyroxine monotherapy relies on this pathway and is generally sufficient.
2. Pharmacokinetics of Levothyroxine
| Parameter | Detail |
|---|---|
| Absorption site | Proximal small bowel |
| Bioavailability (fasting) | 60-80% |
| Time to peak concentration | ~2 hours (fasting); may be prolonged to ~3 hours in hypothyroid state |
| Plasma half-life | ~7 days |
| Protein binding | Thyroxine-binding globulin (TBG), transthyretin (TBPA), albumin |
| Metabolism | Peripheral deiodination → T3 (active) or rT3 (inactive); hepatic conjugation |
| Steady state | Achieved at 6-8 weeks after a consistent dose |
| Formulation | Oral tablets (standard); IV available for emergencies |
3. Dosing
Standard Adult Dosing
- Average full replacement: ~1.7 mcg/kg/day (~125 mcg/day for a 70 kg adult); based on lean body mass
- Older adults (>65 years): ~1.6 mcg/kg/day; lower body mass and slower clearance reduce requirement
- Post-thyroidectomy TSH suppression (thyroid cancer): ~2.2 mcg/kg/day
Age-Specific Dosing
| Age Group | Dose (mcg/kg/day) |
|---|---|
| Infants 1-6 months | 10-15 |
| Children (older) | 4-8 (decreasing with age) |
| Adolescents | 2-3 |
| Adults | ~1.7 |
| Elderly (>65 yr) | ~1.6 (some guidelines: ~0.5 mcg/kg/day) |
Initiating Therapy - Clinical Approach
| Patient Type | Starting Dose | Titration |
|---|---|---|
| Young, otherwise healthy, mild disease | Full replacement immediately | Adjust by TSH at 6-8 weeks |
| Age >50 years, no cardiac disease | 50 mcg/day | Increase as tolerated |
| Elderly / long-standing hypothyroidism / cardiac disease | 12.5-25 mcg/day | Increase by 12.5-25 mcg every 2 weeks |
Cardiac caveat: In patients with coronary artery disease, low thyroid hormone paradoxically protects the heart by reducing oxygen demand. Overly rapid correction can precipitate angina, arrhythmia, or myocardial infarction. If coronary revascularization is indicated, it should be performed before aggressive T4 replacement. Reduce or stop T4 immediately if angina or arrhythmia develops.
4. Monitoring
| Type | Monitor | Target | Timing |
|---|---|---|---|
| Primary hypothyroidism | Serum TSH | 0.5-2.5 mIU/L | 6-8 weeks after dose change; 4-6 months; then yearly |
| Secondary/tertiary (central) hypothyroidism | Free T4 (TSH unreliable) | Upper third of reference range | Same intervals |
| Children | TSH + Free T4 + growth/development | Age-appropriate | More frequent |
| Elderly | TSH + watch for AF, bone density | 0.5-2.5 mIU/L | Yearly |
5. Administration Pearls
Factors Reducing Levothyroxine Absorption
- Foods: Bran, soy, soy formula (infants), coffee, grapefruit, papaya, dietary fiber
- Drugs: Calcium carbonate, ferrous sulfate (iron), cholestyramine, colestipol, sucralfate, antacids (aluminum, magnesium), PPIs
- Conditions requiring higher doses: Malabsorption syndromes, celiac disease, atrophic gastritis, H. pylori gastritis, lactose intolerance, post-bariatric surgery, small bowel surgery
Separate levothyroxine from any of the above by at least 4 hours.
Factors Increasing Dose Requirement
- Pregnancy
- Estrogen/oral contraceptives (increase TBG)
- Rifampin, phenytoin, carbamazepine (hepatic enzyme induction, faster T4 clearance)
- Sertraline (accelerates T4 clearance)
- Post-thyroidectomy patients (tend to need higher doses than those with autoimmune thyroiditis)
6. Special Clinical Situations
A. Subclinical Hypothyroidism (SCH)
- TSH >10 mIU/L, age <65-70 years: Levothyroxine recommended
- TSH <10 mIU/L with symptoms: Consider a levothyroxine trial; discontinue if symptoms don't improve
- TSH ≤10 mIU/L, age >80-85 years: Watchful waiting - age-related TSH rise may not require treatment
B. Hypothyroidism in Pregnancy
- Increase levothyroxine dose by ~25-30% as soon as pregnancy is confirmed - practical approach: two extra tablets per week
- TSH targets by trimester:
- 1st trimester: 0.1-2.5 mIU/L
- 2nd trimester: 0.2-3.0 mIU/L
- 3rd trimester: 0.3-3.0 mIU/L
- Separate T4 from prenatal vitamins and calcium by at least 4 hours
- Increase TBG from estrogen elevates total T4 - use TSH as the primary guide
- Revert to pre-pregnancy dose the day after delivery; recheck TSH at 6 weeks postpartum
C. Myxedema Coma (Emergency)
| Drug | Dose | Route | Purpose |
|---|---|---|---|
| Levothyroxine | Loading: 300-400 mcg, then 50-100 mcg/day | IV (GI absorption unreliable) | Primary replacement |
| Liothyronine (T3) | 5-20 mcg initially, then 2.5-10 mcg every 8 h | IV | Added by some clinicians until stable; more cardiotoxic |
| Hydrocortisone | 50-100 mg every 6-8 h | IV | Until concomitant adrenal insufficiency excluded |
Patients have large empty T3/T4 binding-protein pools; these must be saturated before free thyroid hormone can act - hence the large loading dose.
D. Congenital Hypothyroidism
- Neonatal screening (heel-prick TSH) allows early detection
- Treatment within the first 2 weeks of life with levothyroxine allows normal physical and intellectual development
- Delayed treatment leads to cretinism (irreversible cognitive impairment, short stature)
- Initial dose: 10-15 mcg/kg/day orally (crushed tablet mixed with breast milk or water); higher end for severe cases
- Monitor free T4 and TSH every 2 weeks initially, then every 1-3 months in the first year
- Soy formula may impair absorption - dose increase may be needed
E. Drug-Induced Hypothyroidism
| Drug | Mechanism |
|---|---|
| Amiodarone | Inhibits T4→T3 conversion; high iodine load; direct thyroid toxicity |
| Lithium | Inhibits thyroid hormone release; ~30% develop elevated TSH |
| Interferon-alpha | Induces thyroid autoimmunity |
| Tyrosine kinase inhibitors | Impair thyroid hormone synthesis/release |
| Immune checkpoint inhibitors | Autoimmune thyroiditis |
- Remove offending agent if possible
- If drug cannot be stopped, treat with levothyroxine
- Amiodarone: T4 replacement may be required even after drug discontinuation due to its extremely long half-life (~40-55 days)
F. Central (Secondary/Tertiary) Hypothyroidism
- TSH unreliable for monitoring - use free T4
- Dose adjusted to maintain free T4 in upper third of reference range
- Critical: Always exclude concomitant central adrenal insufficiency before starting levothyroxine - starting T4 without replacing cortisol can precipitate an adrenal crisis (T4 accelerates cortisol clearance)
G. Thyroid Cancer (TSH Suppression)
- Higher levothyroxine doses used to suppress TSH as a growth factor for thyroid cancer
- Average dose: ~2.2 mcg/kg/day
- TSH targets depend on risk stratification:
- Low-risk/no persistent disease: low-normal TSH
- High recurrence risk: ~0.1 mU/L
- Persistent disease: <0.1 mU/L
7. Combination T4 + T3 Therapy
- No long-acting T3 preparation exists, so T3 causes peaks and troughs
- Existing trials show no consistent superiority over T4 alone
- Current T4/T3 preparations don't match the thyroid's natural ~11:1 T4:T3 secretion ratio
- Generic-to-generic levothyroxine switching does not cause clinically significant TSH fluctuations
- ~20% of circulating T3 normally comes directly from the thyroid; T4 monotherapy doesn't perfectly replicate this
- A subset with Dio2 Thr92Ala polymorphism (impaired intracellular T4→T3 conversion) may benefit - but evidence is currently insufficient for routine testing
- Some patients persistently feel unwell despite normal TSH/free T4 on levothyroxine alone; trials have not studied this group specifically
- A crossover study showed some patients preferred desiccated thyroid extract (DTE) with associated weight loss
8. Toxicity from Overtreatment
| Adults | Children |
|---|---|
| Nervousness, heat intolerance | Restlessness, insomnia |
| Palpitations, tachycardia | Accelerated bone age |
| Unexplained weight loss | Premature craniosynostosis |
| Atrial fibrillation (elderly) | Accelerated growth |
| Accelerated osteoporosis |
9. Recent Evidence (2025-2026)
Deltopectoral free flap
"deltopectoral flap" AND "reconstruction"
Deltopectoral Flap
Important clarification: The question says "deltopectoral free flap," but the deltopectoral flap is classically a pedicled axial pattern flap - not a free flap. It was historically used as a pedicled regional flap, and in rare instances the internal mammary vessels have been used as a pedicle for free transfer (a technique described but rarely employed). This response covers the classic pedicled deltopectoral flap comprehensively, as this is the clinically standard usage.
1. Historical Background
- Pectoralis major myocutaneous flap (Ariyan, 1979) - single-stage, muscle bulk
- Free tissue transfer (radial forearm, anterolateral thigh, jejunal flaps)
2. Flap Classification
| Property | Detail |
|---|---|
| Type | Axial pattern fasciocutaneous flap |
| Classification | Regional pedicled flap |
| Blood supply | Axial (named vessel perforators) |
| Tissue type | Skin + subcutaneous tissue |
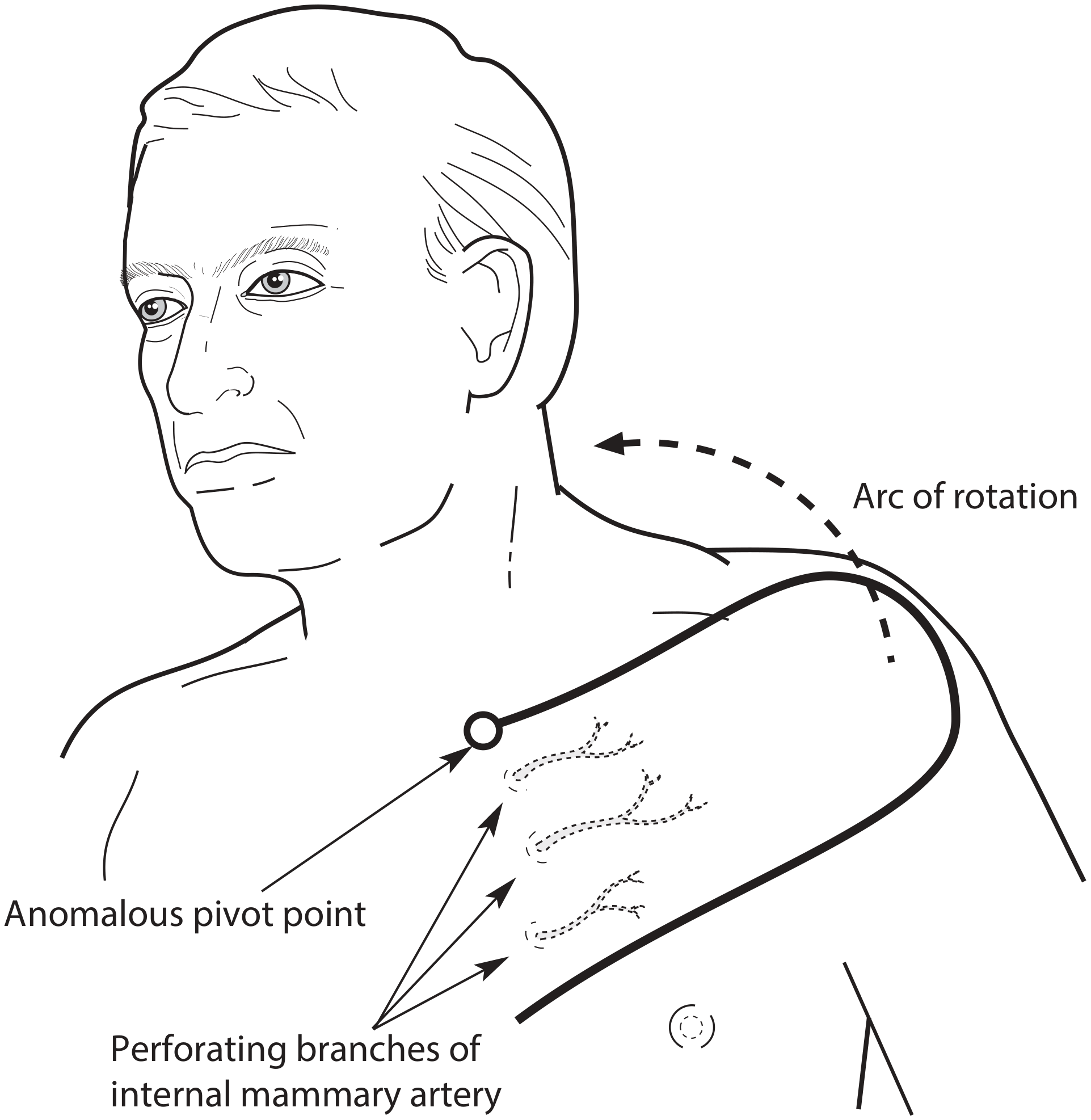
| Pedicle | Perforating branches of internal mammary artery |
3. Vascular Anatomy
4. Flap Boundaries and Dimensions
| Border | Landmark |
|---|---|
| Superior | Clavicle |
| Lateral | Acromion / deltopectoral groove |
| Inferior | Line through anterior axillary fold to above nipple |
| Medial | Sternal border (pedicle base) |
5. Anomalous Pivot Point
- There is considerable laxity of skin on the anterior axillary fold when the arm is abducted
- This means the lower border of the flap is longer than the upper border
- Therefore, the effective pivot point is at the medial end of the upper limb of the flap - not at the lower limb
- This must be factored into flap planning and transfer; failure to appreciate this leads to miscalculation of reach
6. Flap Elevation - Surgical Technique
- Marking: Landmarks are identified - clavicle superiorly, acromion laterally, anterior axillary fold inferiorly, sternal border medially
- Elevation begins laterally, lifting the flap from lateral to medial
- The pectoral fascia is included with the flap, leaving the underlying pectoralis major muscle fibres bare
- Any branches of the acromiothoracic axis encountered must be ligated (these are not the flap's blood supply and their inclusion risks flap elevation complications)
- Monopolar diathermy is used judiciously - excessive use can damage the flap or leave marks on exposed muscle that compromise subsequent skin graft take
- Retraction during elevation is upward using skin hooks - the flap must not be folded back on itself, which risks buttonholing
- The donor site is covered with a split-skin graft
7. Clinical Uses
- Rotated directly to resurface anterior cervical skin defects
- Passed over normal skin as a bridge to a distant defect
- After 3 weeks (once the flap tip has established a new blood supply from the recipient bed), the pedicle is divided
- The remaining flap segment can be returned to the donor site or discarded
- Pedicle is inserted into part of the defect to facilitate vascular ingrowth
- Pedicle is then divided inferiorly and the flap inset into the remainder of the defect
- Most commonly used today to close a fistula after failed hypopharyngeal reconstruction or post-laryngectomy fistula
- Note: where muscle bulk is also required, myocutaneous flaps are preferred
- Used via a controlled fistula approach for circumferential pharyngeal defects
- Largely replaced by free jejunal flap and anterolateral thigh flap
- Thin, pliable skin well suited to external facial resurfacing

8. Advantages
| Advantage | Explanation |
|---|---|
| Reliable axial blood supply | No need for surgical delay in most cases |
| Outside typical radiation fields | Fresh, non-irradiated tissue for post-radiotherapy cases |
| Thin, pliable skin | Good for surface reconstruction; can be tubed |
| No muscle sacrifice | Donor site morbidity is low |
| Large surface area | Can cover substantial defects |
| Reaches upper neck/lower face | Adequate arc of rotation |
9. Disadvantages and Complications
| Disadvantage | Detail |
|---|---|
| Multistage procedure required | For pharyngeal reconstruction - requires a secondary division procedure (at least 3-6 weeks later) |
| Tip necrosis | If flap extended beyond deltopectoral groove (random territory) |
| Donor site morbidity | Requires split-skin graft; visible chest scar |
| Fistula formation | When used for pharyngeal reconstruction |
| Stenosis | Long-term complication in pharyngeal use |
| Bulky in obese patients | Thick subcutaneous tissue makes tubing difficult |
| Limited muscle bulk | Cannot fill deep 3D dead space; not suitable where volume is needed |
| Male patients | Hair-bearing skin problematic for intraoral/intramucosal inset |
10. The Deltopectoral Flap as a Free Flap
- The internal mammary vessels are not easily harvested without significant morbidity (rib cartilage removal required to improve mobility)
- Superior free flap donor sites now exist (radial forearm, ALT, jejunum) with more reliable pedicle anatomy and longer vascular leashes
11. Place in Modern Head and Neck Reconstruction
- Local cervical flaps (random pattern, high failure) - pre-1960s
- Deltopectoral flap (first axial flap, 1965) - transformative
- Pectoralis major myocutaneous flap (1979) - single-stage reliability
- Free tissue transfer (radial forearm, jejunum, ALT) - current gold standard
Surgical anatomy of mastoid bone
Surgical Anatomy of the Mastoid Bone
1. Overview and Development
- May be extensive: involving the mastoid tip, squama, petrous apex, and even adjacent zygoma and occipital bone
- May be limited: to a single antral cell
- Non-pneumatized mastoids contain solid cortical bone or diploic (spongy) bone with fatty marrow
2. Gross Anatomy and Surface Landmarks
| Surface Landmark | Surgical Relevance |
|---|---|
| Temporal line (supramastoid crest) | Upper limit of initial cortical bone removal; marks level of middle cranial fossa floor |
| Mastoid tip | Attachment of sternocleidomastoid, splenius capitis, longissimus capitis |
| Digastric ridge (mastoid notch) | Medial aspect of mastoid tip; points to lateral and inferior mastoid segment of facial nerve |
| Spine of Henle (suprameatal spine) | Anterior superior surface landmark at junction of EAC and mastoid |
| MacEwen's triangle (suprameatal triangle) | Bounded by temporal line superiorly, posterior wall of EAC anteriorly, and tangent line posteriorly; surface projection of mastoid antrum |
| Sigmoid sinus groove | Posterior surface of mastoid; corresponds to position of sigmoid sinus |
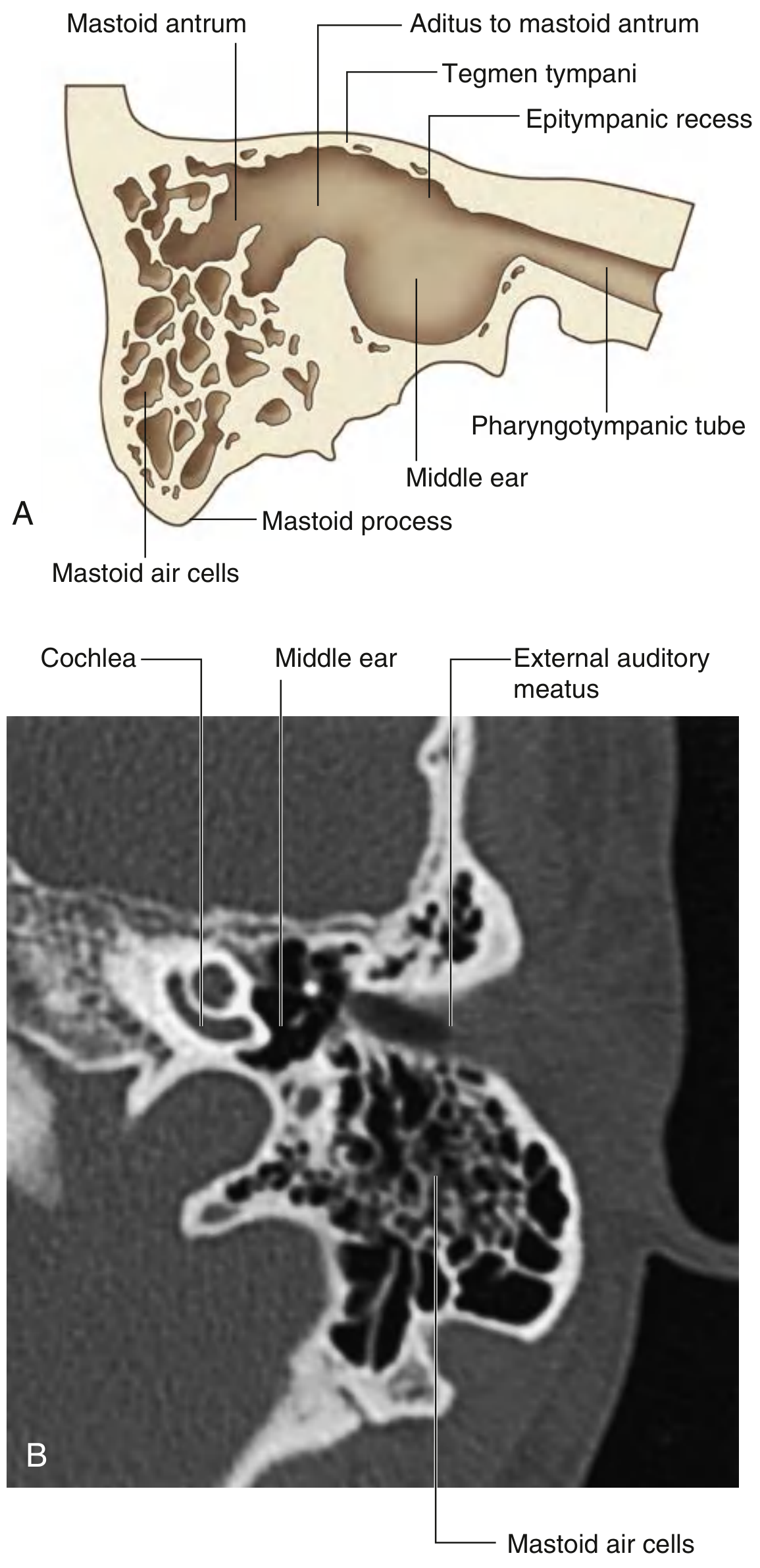
3. Mastoid Antrum
| Feature | Detail |
|---|---|
| Position | Posteromedial to the epitympanic recess |
| Communication anteriorly | Via the aditus ad antrum → epitympanum |
| Roof | Tegmen mastoideum (part of tegmen tympani) - only a thin plate of bone separating antrum from middle cranial fossa |
| Floor | Mastoid tip cells |
| Medial wall | Lateral semicircular canal (dome visible on its floor) |
| Lateral wall | Squamous temporal bone (cortical bone removed during mastoidectomy) |
| Depth from surface | Approximately 12-15 mm in adults (less in children) |
4. Tegmen
- Oriented in the horizontal plane, just inferior to the arcuate eminence (which marks the top of the superior semicircular canal)
- A low-lying tegmen is not uncommon - the floor of the middle fossa can deepen laterally to form a groove above the attic and labyrinth
- Low-hanging dura may cover the roof of the external auditory canal - a surgical hazard in congenital atresia cases
- Fractures or erosion here allow spread of mastoid infection to the middle cranial fossa (subdural empyema, meningitis)
5. Sigmoid Sinus
- Forms a shallow S-shaped groove on the posterior aspect of the mastoid
- Varies considerably in position: in some individuals it curves anteriorly and sits very close to the posterior EAC wall (especially in patients with chronic ear disease - a hazard during mastoidectomy)
- Only a thin bony plate (the bony plate of the sigmoid sinus or sinus plate) separates it from the mastoid cells
- Trautmann's triangle: bounded by the sigmoid sinus posteriorly, the labyrinth anteriorly, and the superior petrosal sinus superiorly - this is the surgical corridor for some posterior fossa approaches
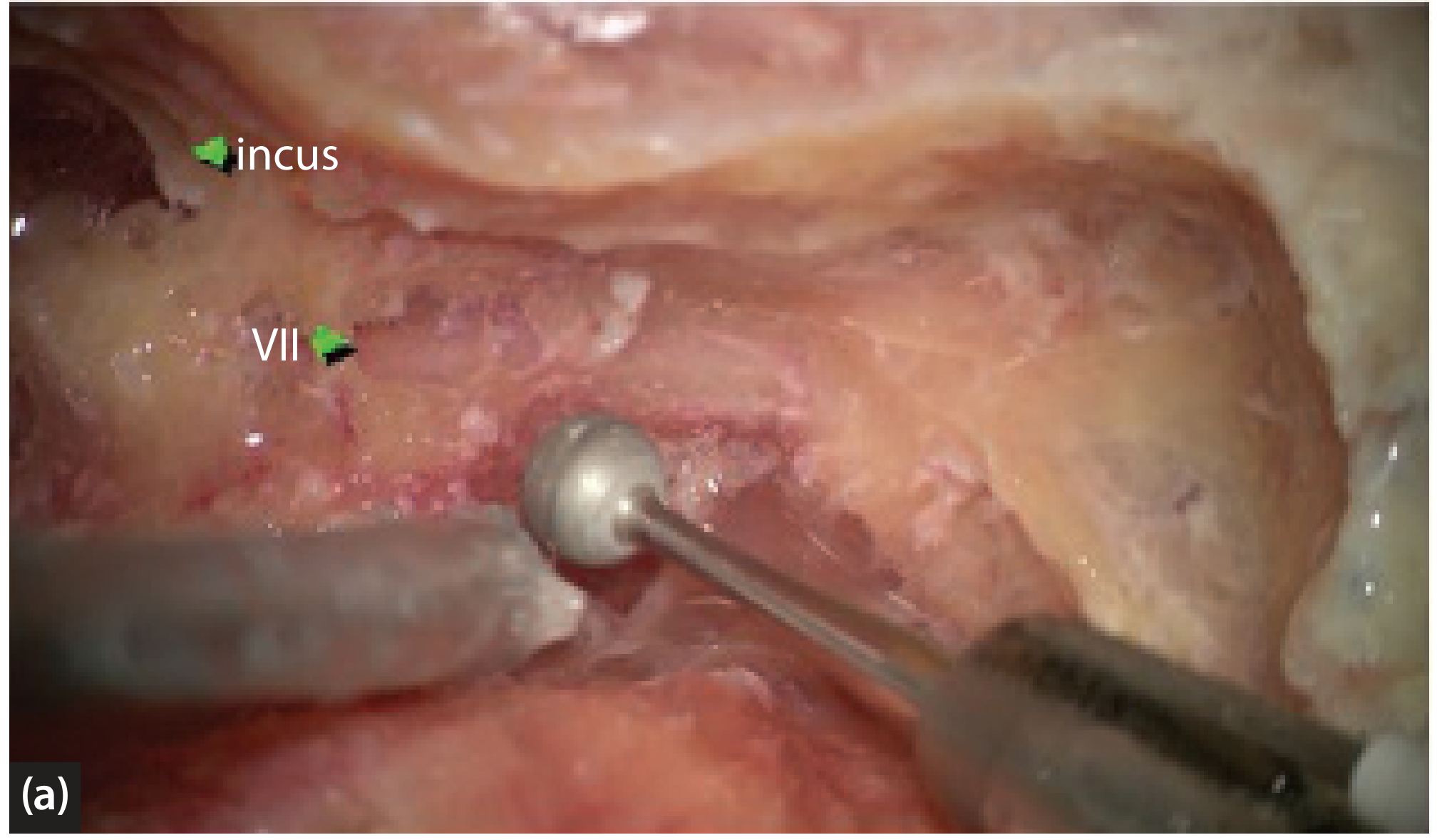
6. Mastoid Segment of the Facial Nerve (CN VII)
- The mastoid (vertical) segment is the longest segment of the intratemporal facial nerve (10-14 mm)
- Runs vertically downward in the posterior wall of the tympanic cavity and anterior wall of the mastoid
- Extends from the second genu (just distal to the pyramidal process) to the stylomastoid foramen at the skull base
- Direction: travels posteromedially to anterolaterally from second genu to stylomastoid foramen
Surgical Landmarks for the Facial Nerve
| Landmark | Significance |
|---|---|
| Horizontal (lateral) semicircular canal | The facial nerve passes just below and medial to the LSCC dome; identifies the level of the second genu |
| Short process of incus | An imaginary line from the short process of incus to the anterior end of the digastric ridge marks the course of the mastoid segment |
| Digastric ridge | Points to the lateral and inferior aspect of the mastoid segment |
| Posterior EAC wall | The nerve lies medial to this - thinning the EAC wall reveals the nerve's position |
| Pyramidal eminence | Marks the position of the second genu |
Key rule: The facial nerve is almost always lateral to the level of the tympanic annulus, but may cross it or lie medial to it in its lower half - so lowering the facial ridge in canal-wall-down procedures risks injury.
7. Semicircular Canals
- Its dome projects into the floor of the antrum and is a key intraoperative landmark
- Identifies the level of the second genu of the facial nerve (nerve lies just inferomedial to dome)
- The posterior semicircular canal (PSCC) lies just posterior and inferior to the LSCC - at risk during posterior tympanotomy and extended mastoidectomy
8. Jugular Bulb and Jugular Fossa
- Highly variable in size - may be small or may extend superiorly to the petrous ridge
- A high-riding jugular bulb may:
- Extend into the hypotympanum or even mesotympanum
- Be dehiscent (without bony cover) within the middle ear - may contact the tympanic membrane
- Cause pulsatile tinnitus
- Bleed profusely if inadvertently entered during tympanostomy tube placement or mastoid surgery
- Mimic a glomus jugulare on otoscopy or MRI
9. Carotid Artery
- Normally covered by the floor of the tympanic cavity
- Can be aberrant/displaced laterally into the middle ear - enters via enlarged inferior tympanic canaliculus, courses through entire middle ear, and reconnects to the horizontal ICA
- An aberrant ICA can be mistaken for a middle ear mass on otoscopy - catastrophic if biopsied or entered surgically
10. Körner's Septum
- Must be recognized and removed to gain access to the true mastoid antrum
- Failure to identify it can lead to false dissection planes
11. Key Spaces and Relationships Summary
| Structure | Location | Surgical Importance |
|---|---|---|
| Mastoid antrum | Posteromedial to epitympanum | Primary target of mastoidectomy |
| Aditus ad antrum | Connects antrum to epitympanum | Route of disease spread |
| Tegmen | Roof of antrum/attic | Boundary with middle cranial fossa; risk of CSF leak |
| Sigmoid sinus | Posterior mastoid | Risk of major venous hemorrhage |
| LSCC | Medial wall of antrum | Landmark for facial nerve; labyrinthine fistula risk |
| Facial nerve (mastoid segment) | Anterior mastoid/posterior tympanic wall | Greatest risk of iatrogenic injury |
| Jugular bulb | Inferior mastoid | Risk of hemorrhage; may be high-riding |
| ICA | Anterior to middle ear | Risk if aberrant |
| Digastric ridge | Inferior mastoid | Guides facial nerve identification |
12. Surgical Application - Canal Wall-Up Mastoidectomy Steps
- Identify temporal line (superior limit) and posterior EAC (anterior limit)
- Remove cortical bone at temporal line - begin exenterating mastoid air cells
- Skeletonize tegmen plate - trace medially toward antrum
- Identify and skeletonize sigmoid sinus posteriorly
- Remove all cells between tegmen and sigmoid sinus
- Identify and open the mastoid antrum
- Identify dome of LSCC at antrum floor
- Identify short process of incus in fossa incudis
- Skeletonize mastoid segment of facial nerve
- Open facial recess (triangle bounded by facial nerve, chorda tympani, and incus buttress) - provides access to middle ear without disturbing EAC wall
The three most critical intraoperative principles: (1) always trace the tegmen medially to find the antrum; (2) identify the sigmoid sinus to define the posterior limit; (3) use the LSCC dome and short process of incus to triangulate the facial nerve before drilling near it.
Pharmacotherapy of Hypothyroidism
Pharmacotherapy of Hypothyroidism
Available Preparations
| Preparation | Contents | Status |
|---|---|---|
| Levothyroxine (T4) | Synthetic L-thyroxine | Drug of choice |
| Liothyronine (T3) | Synthetic L-triiodothyronine | Adjunct / emergency use |
| Desiccated thyroid extract (DTE) | Porcine T4 + T3 (~4:1 ratio) | Occasional patient preference |
1. Levothyroxine - Drug of Choice
- Consistent, predictable potency and chemical stability
- Long plasma half-life (~7 days) → once-daily dosing
- Peripheral deiodination (Dio1, Dio2) converts T4 → active T3 in tissues, mimicking normal physiology
- ~80% of circulating T3 derives from peripheral T4 conversion; levothyroxine relies on this pathway
- Multiple controlled trials confirm no inferiority compared to combination T4+T3
2. Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption site | Proximal small bowel |
| Bioavailability (fasting) | 60–80% |
| Time to peak | ~2 h fasting; ~3 h in hypothyroid state |
| Plasma half-life | ~7 days (extensive TBG/TBPA/albumin binding) |
| Metabolism | Peripheral deiodination → T3 (active) or rT3 (inactive); hepatic conjugation |
| Steady state | 6–8 weeks after a consistent dose |
3. Dosing
Standard Adult Doses
| Indication | Dose |
|---|---|
| Average full replacement | ~1.7 mcg/kg/day (~125 mcg/day for 70 kg adult) |
| Elderly (>65 years) | ~1.6 mcg/kg/day (lower lean body mass) |
| Post-thyroidectomy TSH suppression (thyroid cancer) | ~2.2 mcg/kg/day |
Age-Specific Dosing
| Age | Dose (mcg/kg/day) |
|---|---|
| Infants 1–6 months | 10–15 |
| Children 6–12 months | 6–8 |
| Children 1–5 years | 5–6 |
| Adolescents | 2–3 |
| Adults | ~1.7 |
| Elderly >65 years | ~1.6 |
Initiating Therapy
| Patient | Starting dose | Titration |
|---|---|---|
| Young / mild disease | Full replacement immediately | Check TSH at 6–8 weeks |
| Age >50 years, no cardiac disease | 50 mcg/day | Increase to target |
| Elderly / long-standing hypothyroidism / cardiac disease | 12.5–25 mcg/day | Increase by 12.5–25 mcg every 2 weeks |
Cardiac caveat: In coronary artery disease, low thyroid hormone levels protect the heart from increased oxygen demand. Overly rapid correction can provoke angina, arrhythmia, or MI. If coronary revascularization is needed, perform it before aggressive T4 replacement.
4. Monitoring
| Type | Monitor | Target | Timing |
|---|---|---|---|
| Primary hypothyroidism | Serum TSH | 0.5–2.5 mIU/L | 6–8 weeks post-dose change; then 4–6 months; then yearly |
| Secondary/tertiary (central) | Free T4 (TSH unreliable) | Upper third of reference range | Same intervals |
| Children | TSH + free T4 + growth | Age-appropriate | More frequent |
| Pregnancy | TSH (primary guide) | Trimester-specific targets | Every 4–6 weeks in first 20 weeks |
5. Administration Pearls
Substances Reducing Absorption (separate by ≥4 hours)
- Calcium carbonate, iron salts
- Cholestyramine, colestipol
- Proton pump inhibitors, antacids (Al/Mg)
- Sucralfate
- Soy, bran, dietary fiber, coffee
Conditions Requiring Higher Doses
- Malabsorption: celiac disease, atrophic gastritis, H. pylori gastritis, lactose intolerance
- Post-bariatric surgery / small bowel resection
- Pregnancy
- Enzyme-inducing drugs (rifampin, phenytoin, carbamazepine)
6. Special Clinical Situations
A. Subclinical Hypothyroidism (SCH)
| TSH Level | Age | Recommendation |
|---|---|---|
| >10 mIU/L | <65–70 years | Levothyroxine recommended |
| <10 mIU/L with symptoms | Any | Consider trial; stop if no improvement |
| ≤10 mIU/L | >80–85 years | Watchful waiting |
B. Hypothyroidism in Pregnancy
- Increase levothyroxine by ~25–30% as soon as pregnancy is confirmed (practical: two extra tablets per week)
- TSH targets: 1st trimester 0.1–2.5 mIU/L; 2nd trimester 0.2–3.0 mIU/L; 3rd trimester 0.3–3.0 mIU/L
- Separate T4 from prenatal vitamins/calcium by ≥4 hours
- Revert to pre-pregnancy dose the day after delivery; recheck TSH at 6 weeks postpartum
C. Myxedema Coma (Emergency)
| Drug | Dose | Route |
|---|---|---|
| Levothyroxine (loading) | 300–400 mcg, then 50–100 mcg/day | IV (GI absorption unreliable) |
| Liothyronine (T3) | 5–20 mcg initially, then 2.5–10 mcg every 8 h | IV (optional; more cardiotoxic) |
| Hydrocortisone | 50–100 mg every 6–8 h | IV (until adrenal insufficiency excluded) |
D. Congenital Hypothyroidism
- Treatment within first 2 weeks of life → normal physical and intellectual development
- Delayed diagnosis → cretinism (irreversible cognitive impairment, short stature)
- Initial dose: 10–15 mcg/kg/day orally (crushed tablet in breast milk/water)
- Monitor free T4 and TSH every 2 weeks initially, then every 1–3 months in the first year
- Soy formula impairs absorption - dose increase may be needed
E. Drug-Induced Hypothyroidism
| Drug | Mechanism |
|---|---|
| Amiodarone | Inhibits T4→T3 conversion; high iodine load; direct thyroid toxicity |
| Lithium | Inhibits thyroid hormone release |
| Interferon-alpha | Induces autoimmune thyroiditis |
| Tyrosine kinase inhibitors | Impair hormone synthesis/release |
| Immune checkpoint inhibitors | Autoimmune thyroiditis |
- Remove offending agent if possible; otherwise treat with levothyroxine
- Amiodarone: Replacement may be required even after stopping, due to its ~40–55 day half-life
F. Central (Secondary/Tertiary) Hypothyroidism
- Monitor with free T4, not TSH (pituitary TSH secretion is abnormal)
- Goal: maintain free T4 in upper third of reference range
- Always exclude coexisting central adrenal insufficiency before starting levothyroxine - starting T4 without cortisol replacement can precipitate an adrenal crisis
G. Thyroid Cancer (TSH Suppression)
- Low-risk / no persistent disease: low-normal TSH
- High recurrence risk: ~0.1 mU/L
- Persistent disease: <0.1 mU/L
7. Combination T4 + T3 Therapy
- No long-acting T3 formulation exists (causes peaks and troughs)
- Existing trials show no consistent superiority over T4 alone
- No T4/T3 preparation matches the thyroid's natural ~11:1 ratio
- Patients persistently symptomatic despite clearly normal TSH/free T4 on levothyroxine
- Possible Dio2 Thr92Ala polymorphism carriers (impaired intracellular T4→T3 conversion) - though routine testing is not yet evidence-based
- Desiccated thyroid extract (DTE): Some crossover studies show patient preference and weight loss benefit, but evidence for clinical superiority is insufficient
8. Drug Interactions with Levothyroxine
| Interacting Drug/Substance | Effect |
|---|---|
| Calcium, iron, PPIs, antacids, sucralfate | Reduced T4 absorption |
| Cholestyramine, colestipol | Binds T4 in gut |
| Rifampin, phenytoin, carbamazepine | Increased hepatic metabolism of T4 → higher dose needed |
| Estrogen / OCP | Increase TBG → may increase dose requirement |
| Amiodarone | Inhibits T4→T3 conversion |
| Warfarin | T4 potentiates anticoagulant effect |
| Soy, bran, coffee | Reduce absorption |
9. Toxicity from Overtreatment
| Adults | Children |
|---|---|
| Nervousness, heat intolerance | Restlessness, insomnia |
| Palpitations, tachycardia | Accelerated bone maturation |
| Unexplained weight loss | Premature craniosynostosis |
| Atrial fibrillation (especially elderly) | Accelerated linear growth |
| Accelerated osteoporosis |
10. Recent Evidence (2025–2026 Updates)
- A 2026 network meta-analysis (PMID 39290156) on treatment preferences found evidence for some benefit of non-levothyroxine-alone regimens in patient-reported outcomes
- A 2026 meta-analysis (PMID 40579157) found that liothyronine-containing regimens are associated with reduced risk of dementia and mortality compared to levothyroxine alone - a finding that may prompt future guideline revision, though current guidelines still recommend T4 monotherapy as first-line
Convert first provided pharmacotherapy of Hypothyroidism to a pdf
ls -la /home/daytona/workspace/
mkdir -p /home/daytona/workspace/hypothyroidism-pdf
Convert first provided pharmacotherapy of Hypothyroidism to a pdf
mkdir -p /home/daytona/workspace/hypothyroidism-pdf && python3 -c "import reportlab; print('reportlab ok')" && python3 -c "import weasyprint; print('weasyprint ok')" 2>/dev/null || echo "checking available tools"
~/hypothyroidism-pdf/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, PageBreak, KeepTogether
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_JUSTIFY
OUTPUT = "/home/daytona/workspace/hypothyroidism-pdf/Pharmacotherapy_of_Hypothyroidism.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
rightMargin=2*cm, leftMargin=2*cm,
topMargin=2.5*cm, bottomMargin=2.5*cm,
title="Pharmacotherapy of Hypothyroidism",
author="Orris Medical Reference"
)
W = A4[0] - 4*cm # usable width
# ── Styles ──────────────────────────────────────────────────────────────────
base = getSampleStyleSheet()
TEAL = colors.HexColor("#0D6E6E")
TEAL_DARK = colors.HexColor("#094F4F")
TEAL_LITE = colors.HexColor("#E6F4F4")
GRAY_LINE = colors.HexColor("#CCCCCC")
BLACK = colors.black
WHITE = colors.white
title_style = ParagraphStyle("DocTitle",
fontSize=22, leading=28, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_CENTER, spaceAfter=4)
subtitle_style = ParagraphStyle("DocSub",
fontSize=10, leading=14, textColor=colors.HexColor("#CCE8E8"),
fontName="Helvetica", alignment=TA_CENTER, spaceAfter=0)
h1_style = ParagraphStyle("H1",
fontSize=14, leading=18, textColor=WHITE,
fontName="Helvetica-Bold", alignment=TA_LEFT,
spaceBefore=10, spaceAfter=4,
leftIndent=0)
h2_style = ParagraphStyle("H2",
fontSize=11, leading=15, textColor=TEAL_DARK,
fontName="Helvetica-Bold", alignment=TA_LEFT,
spaceBefore=8, spaceAfter=3)
h3_style = ParagraphStyle("H3",
fontSize=10, leading=14, textColor=TEAL_DARK,
fontName="Helvetica-BoldOblique", alignment=TA_LEFT,
spaceBefore=6, spaceAfter=2)
body_style = ParagraphStyle("Body",
fontSize=9.5, leading=14, textColor=BLACK,
fontName="Helvetica", alignment=TA_JUSTIFY,
spaceBefore=2, spaceAfter=4)
bullet_style = ParagraphStyle("Bullet",
fontSize=9.5, leading=13, textColor=BLACK,
fontName="Helvetica", alignment=TA_LEFT,
leftIndent=14, firstLineIndent=-10,
spaceBefore=1, spaceAfter=1)
note_style = ParagraphStyle("Note",
fontSize=9, leading=13, textColor=colors.HexColor("#333333"),
fontName="Helvetica-Oblique", alignment=TA_LEFT,
leftIndent=10, rightIndent=10,
spaceBefore=4, spaceAfter=4,
borderPad=5)
source_style = ParagraphStyle("Source",
fontSize=8.5, leading=12, textColor=colors.HexColor("#555555"),
fontName="Helvetica-Oblique", alignment=TA_CENTER,
spaceBefore=6, spaceAfter=2)
# ── Helpers ──────────────────────────────────────────────────────────────────
def h1_block(text):
"""Section header with teal background bar."""
tbl = Table([[Paragraph(text, h1_style)]], colWidths=[W])
tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), TEAL),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("TOPPADDING", (0,0), (-1,-1), 6),
("BOTTOMPADDING",(0,0), (-1,-1), 6),
("ROUNDEDCORNERS", [4]),
]))
return tbl
def simple_table(headers, rows, col_widths=None):
"""Styled two-tone table."""
if col_widths is None:
n = len(headers)
col_widths = [W/n]*n
data = [[Paragraph(f"<b>{h}</b>", ParagraphStyle("TH",
fontSize=9, fontName="Helvetica-Bold",
textColor=WHITE, alignment=TA_LEFT)) for h in headers]]
for r in rows:
data.append([Paragraph(str(c), ParagraphStyle("TD",
fontSize=9, fontName="Helvetica",
textColor=BLACK, alignment=TA_LEFT, leading=12)) for c in r])
t = Table(data, colWidths=col_widths, repeatRows=1)
style = [
("BACKGROUND", (0,0), (-1,0), TEAL),
("GRID", (0,0), (-1,-1), 0.4, GRAY_LINE),
("TOPPADDING", (0,0), (-1,-1), 4),
("BOTTOMPADDING", (0,0), (-1,-1), 4),
("LEFTPADDING", (0,0), (-1,-1), 5),
("RIGHTPADDING", (0,0), (-1,-1), 5),
("VALIGN", (0,0), (-1,-1), "TOP"),
]
for i in range(1, len(data)):
bg = TEAL_LITE if i % 2 == 0 else WHITE
style.append(("BACKGROUND", (0,i), (-1,i), bg))
t.setStyle(TableStyle(style))
return t
def note_box(text):
"""Highlighted note / callout box."""
tbl = Table([[Paragraph(f"<b>Note:</b> {text}", note_style)]], colWidths=[W])
tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#FFF8E1")),
("LINEAFTER", (0,0), (0,-1), 2, colors.HexColor("#F5A623")),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
]))
return tbl
def warning_box(text):
tbl = Table([[Paragraph(f"<b>Warning:</b> {text}", note_style)]], colWidths=[W])
tbl.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), colors.HexColor("#FDECEA")),
("LINEAFTER", (0,0), (0,-1), 2, colors.red),
("LEFTPADDING", (0,0), (-1,-1), 8),
("RIGHTPADDING", (0,0), (-1,-1), 8),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
]))
return tbl
def b(txt): return f"<b>{txt}</b>"
def i(txt): return f"<i>{txt}</i>"
# ── Content ──────────────────────────────────────────────────────────────────
story = []
# ── TITLE BANNER ──
title_banner = Table(
[[Paragraph("Pharmacotherapy of Hypothyroidism", title_style)],
[Paragraph("Based on Katzung | Goodman & Gilman | Tietz Laboratory Medicine", subtitle_style)]],
colWidths=[W]
)
title_banner.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,-1), TEAL_DARK),
("TOPPADDING", (0,0), (-1,-1), 16),
("BOTTOMPADDING", (0,0), (-1,-1), 16),
("LEFTPADDING", (0,0), (-1,-1), 10),
("RIGHTPADDING", (0,0), (-1,-1), 10),
]))
story.append(title_banner)
story.append(Spacer(1, 0.4*cm))
# ── SECTION 1 ──
story.append(h1_block("1. Therapeutic Preparations"))
story.append(Spacer(1, 0.2*cm))
story.append(simple_table(
["Preparation", "Contents", "Status"],
[
["Levothyroxine (T4)", "Synthetic L-thyroxine", "Drug of choice"],
["Liothyronine (T3)", "Synthetic L-triiodothyronine", "Adjunct / emergency use"],
["Desiccated thyroid extract (DTE)", "Porcine T4 + T3 (~4:1 ratio)", "Occasional patient preference"],
],
col_widths=[W*0.33, W*0.37, W*0.30]
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 2 ──
story.append(h1_block("2. Levothyroxine — Drug of Choice"))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
"Levothyroxine sodium (synthetic L-thyroxine, T4) is universally recommended as first-line therapy "
"for all forms of hypothyroidism by the American Thyroid Association (ATA) and European Thyroid "
"Association (ETA).",
body_style
))
story.append(Paragraph(b("Why T4 is preferred over T3 or DTE:"), h3_style))
for pt in [
"Consistent, predictable potency and chemical stability",
"Long plasma half-life (~7 days) — enables once-daily dosing",
"Peripheral deiodination (Dio1, Dio2) converts T4 → active T3, closely mimicking normal physiology",
"~80% of circulating T3 derives from peripheral T4 conversion",
"Multiple controlled trials confirm no inferiority compared to T4+T3 combination",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 3 ──
story.append(h1_block("3. Pharmacokinetics of Levothyroxine"))
story.append(Spacer(1, 0.2*cm))
story.append(simple_table(
["Parameter", "Detail"],
[
["Absorption site", "Proximal small bowel"],
["Bioavailability (fasting)", "60–80%"],
["Time to peak concentration", "~2 h (fasting); ~3 h in hypothyroid state"],
["Plasma half-life", "~7 days (extensive TBG, TBPA, albumin binding)"],
["Metabolism", "Peripheral deiodination → T3 (active) or rT3 (inactive); hepatic conjugation"],
["Steady state", "6–8 weeks after a consistent dose"],
["Formulation", "Oral tablets (standard); IV available for emergencies"],
],
col_widths=[W*0.38, W*0.62]
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 4 ──
story.append(h1_block("4. Dosing"))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(b("Standard Adult Dosing"), h2_style))
story.append(simple_table(
["Indication", "Dose"],
[
["Average full replacement (adults)", "~1.7 mcg/kg/day (~125 mcg/day for 70 kg)"],
["Older adults (>65 years)", "~1.6 mcg/kg/day"],
["Post-thyroidectomy TSH suppression (thyroid cancer)", "~2.2 mcg/kg/day"],
],
col_widths=[W*0.55, W*0.45]
))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(b("Age-Specific Dosing"), h2_style))
story.append(simple_table(
["Age Group", "Dose (mcg/kg/day)"],
[
["Infants 1–6 months", "10–15"],
["Children 6–12 months", "6–8"],
["Children 1–5 years", "5–6"],
["Adolescents (>12 years)", "2–3"],
["Adults", "~1.7"],
["Elderly (>65 years)", "~1.6"],
],
col_widths=[W*0.55, W*0.45]
))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph(b("Initiating Therapy"), h2_style))
story.append(simple_table(
["Patient Type", "Starting Dose", "Titration"],
[
["Young / mild disease", "Full replacement immediately", "Check TSH at 6–8 weeks"],
["Age >50 yr, no cardiac disease", "50 mcg/day", "Increase to target"],
["Elderly / long-standing / cardiac disease", "12.5–25 mcg/day", "Increase by 12.5–25 mcg every 2 weeks"],
],
col_widths=[W*0.36, W*0.32, W*0.32]
))
story.append(Spacer(1, 0.2*cm))
story.append(warning_box(
"In coronary artery disease, low thyroid hormone levels protect the heart from increased oxygen demand. "
"Overly rapid T4 correction can precipitate angina, arrhythmia, or MI. "
"Perform coronary revascularization before aggressive T4 replacement if both are needed."
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 5 ──
story.append(h1_block("5. Monitoring"))
story.append(Spacer(1, 0.2*cm))
story.append(simple_table(
["Type", "Monitor", "Target", "Timing"],
[
["Primary hypothyroidism", "Serum TSH", "0.5–2.5 mIU/L", "6–8 wk post-change; then 4–6 months; then yearly"],
["Secondary/tertiary (central)", "Free T4 (TSH unreliable)", "Upper third of reference range", "Same intervals"],
["Children", "TSH + Free T4 + growth", "Age-appropriate", "More frequent"],
["Pregnancy", "TSH (primary guide)", "Trimester-specific", "Every 4–6 wk in first 20 wk"],
],
col_widths=[W*0.22, W*0.22, W*0.26, W*0.30]
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 6 ──
story.append(h1_block("6. Administration Pearls"))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
"Take on an empty stomach — 30–60 min before breakfast <b>or</b> at bedtime (4 h after last meal). "
"Food and caffeine delay absorption.",
body_style
))
story.append(Paragraph(b("Substances Reducing Absorption (separate by ≥4 hours):"), h3_style))
for pt in [
"Calcium carbonate, iron salts (ferrous sulfate)",
"Cholestyramine, colestipol",
"Proton pump inhibitors, sucralfate, antacids (Al/Mg)",
"Soy products, dietary bran/fiber, coffee",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Paragraph(b("Conditions Requiring Higher Doses:"), h3_style))
for pt in [
"Malabsorption: celiac disease, atrophic gastritis, H. pylori gastritis, lactose intolerance",
"Post-bariatric surgery / small bowel resection",
"Pregnancy (increased TBG, Dio3 expression by placenta)",
"Enzyme-inducing drugs (rifampin, phenytoin, carbamazepine)",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 7 ──
story.append(h1_block("7. Special Clinical Situations"))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph("A. Subclinical Hypothyroidism (SCH)", h2_style))
story.append(Paragraph(
"Defined as elevated TSH + normal free T4. Prevalence: 4–10% general population; up to 20% in women >50 years.",
body_style
))
story.append(simple_table(
["TSH Level", "Age", "Recommendation"],
[
[">10 mIU/L", "<65–70 years", "Levothyroxine recommended"],
["<10 mIU/L with symptoms", "Any", "Consider trial; stop if no improvement"],
["≤10 mIU/L", ">80–85 years", "Watchful waiting"],
],
col_widths=[W*0.28, W*0.24, W*0.48]
))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("B. Hypothyroidism in Pregnancy", h2_style))
story.append(Paragraph(
"Overt hypothyroidism: risk of miscarriage, preterm birth, fetal distress, impaired fetal neurodevelopment.",
body_style
))
for pt in [
"Increase levothyroxine by ~25–30% as soon as pregnancy confirmed (practical: 2 extra tablets/week)",
"TSH targets: 1st trimester 0.1–2.5 mIU/L; 2nd trimester 0.2–3.0 mIU/L; 3rd trimester 0.3–3.0 mIU/L",
"Separate T4 from prenatal vitamins/calcium by ≥4 hours",
"Revert to pre-pregnancy dose the day after delivery; recheck TSH at 6 weeks postpartum",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("C. Myxedema Coma — Emergency", h2_style))
story.append(Paragraph(
i("Rare, life-threatening extreme of untreated hypothyroidism. Precipitants: infection, heart failure, "
"non-compliance. Most common in elderly women in winter months."),
body_style
))
story.append(Paragraph(b("Cardinal features: ") + "hypothermia, respiratory depression, decreased consciousness, "
"hyponatremia, hypoglycemia, shock", body_style))
story.append(simple_table(
["Drug", "Dose", "Route"],
[
["Levothyroxine (loading)", "300–400 mcg, then 50–100 mcg/day", "IV (GI absorption unreliable)"],
["Liothyronine (T3)", "5–20 mcg initially, then 2.5–10 mcg every 8 h", "IV (optional; more cardiotoxic)"],
["Hydrocortisone", "50–100 mg every 6–8 h", "IV (until adrenal insufficiency excluded)"],
],
col_widths=[W*0.28, W*0.45, W*0.27]
))
story.append(Spacer(1, 0.15*cm))
story.append(note_box(
"All drugs must be given IV — GI absorption is unreliable in myxedema coma. "
"ICU care, mechanical ventilation if needed, passive rewarming, cautious IV fluids (SIADH risk). "
"Opioids and sedatives must be used with extreme caution."
))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("D. Congenital Hypothyroidism", h2_style))
for pt in [
"Treatment within first 2 weeks of life → normal physical and intellectual development",
"Delayed diagnosis → cretinism (irreversible cognitive impairment, short stature)",
"Initial dose: 10–15 mcg/kg/day orally (crushed tablet in breast milk/water); higher end for severe cases",
"Monitor free T4 + TSH every 2 weeks initially, then every 1–3 months in the first year",
"Soy formula impairs absorption — dose increase may be needed",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("E. Drug-Induced Hypothyroidism", h2_style))
story.append(simple_table(
["Drug", "Mechanism"],
[
["Amiodarone", "Inhibits T4→T3 conversion; high iodine load; direct thyroid toxicity"],
["Lithium", "Inhibits thyroid hormone release (~30% develop elevated TSH)"],
["Interferon-alpha", "Induces autoimmune thyroiditis"],
["Tyrosine kinase inhibitors", "Impair thyroid hormone synthesis/release"],
["Immune checkpoint inhibitors", "Autoimmune thyroiditis"],
],
col_widths=[W*0.38, W*0.62]
))
story.append(Spacer(1, 0.1*cm))
story.append(note_box(
"Amiodarone: Levothyroxine replacement may be required even after stopping, "
"due to amiodarone's extremely long half-life (~40–55 days)."
))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("F. Central (Secondary/Tertiary) Hypothyroidism", h2_style))
for pt in [
"Monitor with free T4, not TSH (pituitary TSH secretion is abnormal)",
"Goal: maintain free T4 in upper third of reference range",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(warning_box(
"Always exclude coexisting central adrenal insufficiency BEFORE starting levothyroxine. "
"Starting T4 without cortisol replacement can precipitate an adrenal crisis."
))
story.append(Spacer(1, 0.25*cm))
story.append(Paragraph("G. Thyroid Cancer (TSH Suppression)", h2_style))
story.append(simple_table(
["Risk Category", "TSH Target"],
[
["Low-risk / no persistent disease", "Low-normal TSH"],
["High recurrence risk", "~0.1 mU/L"],
["Persistent disease", "<0.1 mU/L"],
],
col_widths=[W*0.5, W*0.5]
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 8 ──
story.append(h1_block("8. Combination T4 + T3 Therapy"))
story.append(Spacer(1, 0.2*cm))
story.append(Paragraph(
b("ATA/ETA position: ") + "Routine combination levothyroxine + liothyronine is "
+ b("not recommended") + " as standard care.",
body_style
))
story.append(Paragraph(b("Why combination is not routine:"), h3_style))
for pt in [
"No long-acting T3 formulation exists — causes peaks and troughs",
"Existing trials show no consistent superiority over T4 alone",
"No T4/T3 preparation matches the thyroid's natural ~11:1 ratio",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Paragraph(b("Where combination may be considered:"), h3_style))
for pt in [
"Patients persistently symptomatic despite normal TSH/free T4 on levothyroxine",
"Possible Dio2 Thr92Ala polymorphism carriers (impaired intracellular T4→T3 conversion)",
"Desiccated thyroid extract (DTE): some patient preference data (crossover studies show weight benefit)",
]:
story.append(Paragraph(f"• {pt}", bullet_style))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 9 ──
story.append(h1_block("9. Drug Interactions with Levothyroxine"))
story.append(Spacer(1, 0.2*cm))
story.append(simple_table(
["Interacting Drug / Substance", "Effect"],
[
["Calcium carbonate, iron salts, PPIs, antacids, sucralfate", "Reduced T4 absorption (separate by ≥4 h)"],
["Cholestyramine, colestipol", "Binds T4 in gut, reduces absorption"],
["Rifampin, phenytoin, carbamazepine", "Increased hepatic T4 metabolism → higher dose needed"],
["Estrogen / oral contraceptives", "Increase TBG → may increase dose requirement"],
["Amiodarone", "Inhibits T4→T3 conversion (can cause hypo- or hyperthyroidism)"],
["Warfarin", "T4 potentiates anticoagulant effect"],
["Soy, bran, coffee", "Reduce gastrointestinal absorption"],
],
col_widths=[W*0.50, W*0.50]
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 10 ──
story.append(h1_block("10. Toxicity from Overtreatment"))
story.append(Spacer(1, 0.2*cm))
story.append(simple_table(
["Adults", "Children"],
[
["Nervousness, heat intolerance", "Restlessness, insomnia"],
["Palpitations, tachycardia", "Accelerated bone maturation"],
["Unexplained weight loss", "Premature craniosynostosis"],
["Atrial fibrillation (especially elderly)", "Accelerated linear growth"],
["Accelerated osteoporosis", ""],
],
col_widths=[W*0.5, W*0.5]
))
story.append(Spacer(1, 0.15*cm))
story.append(note_box(
"Monitor TSH and free T4 when toxicity symptoms arise. "
"Stop or reduce dose immediately if angina or arrhythmia develops in cardiac patients."
))
story.append(Spacer(1, 0.3*cm))
# ── SECTION 11 ──
story.append(h1_block("11. Recent Evidence (2025–2026)"))
story.append(Spacer(1, 0.2*cm))
story.append(simple_table(
["Study", "Finding"],
[
["Network meta-analysis, J Clin Endocrinol Metab 2025 (PMID 39290156)",
"Examined treatment preferences; evidence for benefit of non-levothyroxine-alone regimens in patient-reported outcomes"],
["Meta-analysis, J Clin Endocrinol Metab 2026 (PMID 40579157)",
"Liothyronine-containing regimens associated with REDUCED RISK of dementia and mortality vs levothyroxine monotherapy"],
],
col_widths=[W*0.42, W*0.58]
))
story.append(Spacer(1, 0.15*cm))
story.append(note_box(
"Current ATA/ETA guidelines still recommend T4 monotherapy as first-line. "
"The 2026 findings may prompt future guideline revision, particularly for symptomatic patients on T4 alone."
))
story.append(Spacer(1, 0.4*cm))
# ── SOURCES ──
story.append(HRFlowable(width=W, thickness=0.5, color=GRAY_LINE))
story.append(Spacer(1, 0.15*cm))
story.append(Paragraph(
"Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed. | "
"Goodman & Gilman's The Pharmacological Basis of Therapeutics | "
"Tietz Textbook of Laboratory Medicine, 7th Ed.",
source_style
))
# ── BUILD ──────────────────────────────────────────────────────────────────
doc.build(story)
print(f"PDF saved to: {OUTPUT}")
python3 /home/daytona/workspace/hypothyroidism-pdf/generate_pdf.py
ls -lh /home/daytona/workspace/hypothyroidism-pdf/Pharmacotherapy_of_Hypothyroidism.pdf
Pharmacotherapy of Hypothyroidism
PDF Document · PDF
- Therapeutic preparations table (Levothyroxine, Liothyronine, DTE)
- Why levothyroxine is the drug of choice
- Pharmacokinetics table
- Dosing - standard adult, age-specific, and initiation approach tables
- Monitoring targets and timing
- Administration pearls + substances reducing absorption
- Special situations - SCH, pregnancy, myxedema coma (with emergency dosing table), congenital hypothyroidism, drug-induced, central hypothyroidism, thyroid cancer
- Combination T4+T3 therapy guidance
- Drug interactions table
- Toxicity / overtreatment signs
- Recent 2025–2026 evidence with PubMed references