Pleural effusion
Reading File
Finding Sources
Searching Images
pleural effusion chest X-ray and anatomy
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of pleural effusion drawn from Murray & Nadel's Textbook of Respiratory Medicine, Grainger & Allison's Diagnostic Radiology, Harrison's Principles of Internal Medicine, and Tintinalli's Emergency Medicine.
Pleural Effusion
Definition
Accumulation of excess fluid in the pleural space. The type of fluid determines its classification: transudate, exudate, blood (haemothorax), chyle (chylothorax), or rarely bile, CSF, or iatrogenic fluids. All types are radiographically identical, though clinical and biochemical features narrow the differential.
Pathophysiology & Classification
Transudates
Caused by imbalanced hydrostatic/oncotic forces — fluid leaks across intact membranes:
- Heart failure (most common cause overall): elevated pulmonary venous pressure overwhelms parietal pleural lymphatic drainage
- Nephrotic syndrome
- Cirrhosis / hepatic hydrothorax (5–10% of cirrhotic patients): small diaphragmatic defects allow ascitic fluid into the pleural space; 85% are right-sided
- Myxoedema: borderline transudate/exudate
Exudates
Caused by inflammation, infection, or malignancy — "leaks in the system":
- Parapneumonic effusion — most common exudative cause in the US; seen in up to 50% of community-acquired pneumonia
- Malignancy (2nd most common exudate) — lung, breast, lymphoma account for ~75% of malignant effusions
- Tuberculosis, pulmonary embolism, pancreatitis, rheumatoid disease, SLE, oesophageal rupture, post-cardiac injury syndrome, aortic dissection
Laterality clues
| Side | Associated causes |
|---|---|
| Right | Heart failure, ascites, liver abscess |
| Left | Pancreatitis, pericarditis, oesophageal rupture, aortic dissection |
| Bilateral | Usually transudates (heart failure, nephrotic, cirrhosis); bilateral exudates in metastases, lymphoma, SLE, pulmonary embolism |
| Massive | Malignancy (lung/breast mets), heart failure, cirrhosis, TB, empyema, trauma |
Clinical Features
- May be clinically silent or present with dyspnoea, cough, pleuritic chest pain
- Percussion dullness and decreased breath sounds at the lung base
- Absence of mediastinal shift despite a large effusion: suggests ipsilateral lung collapse or extensive pleural malignancy (e.g., mesothelioma)
Imaging
Chest X-ray (PA erect)
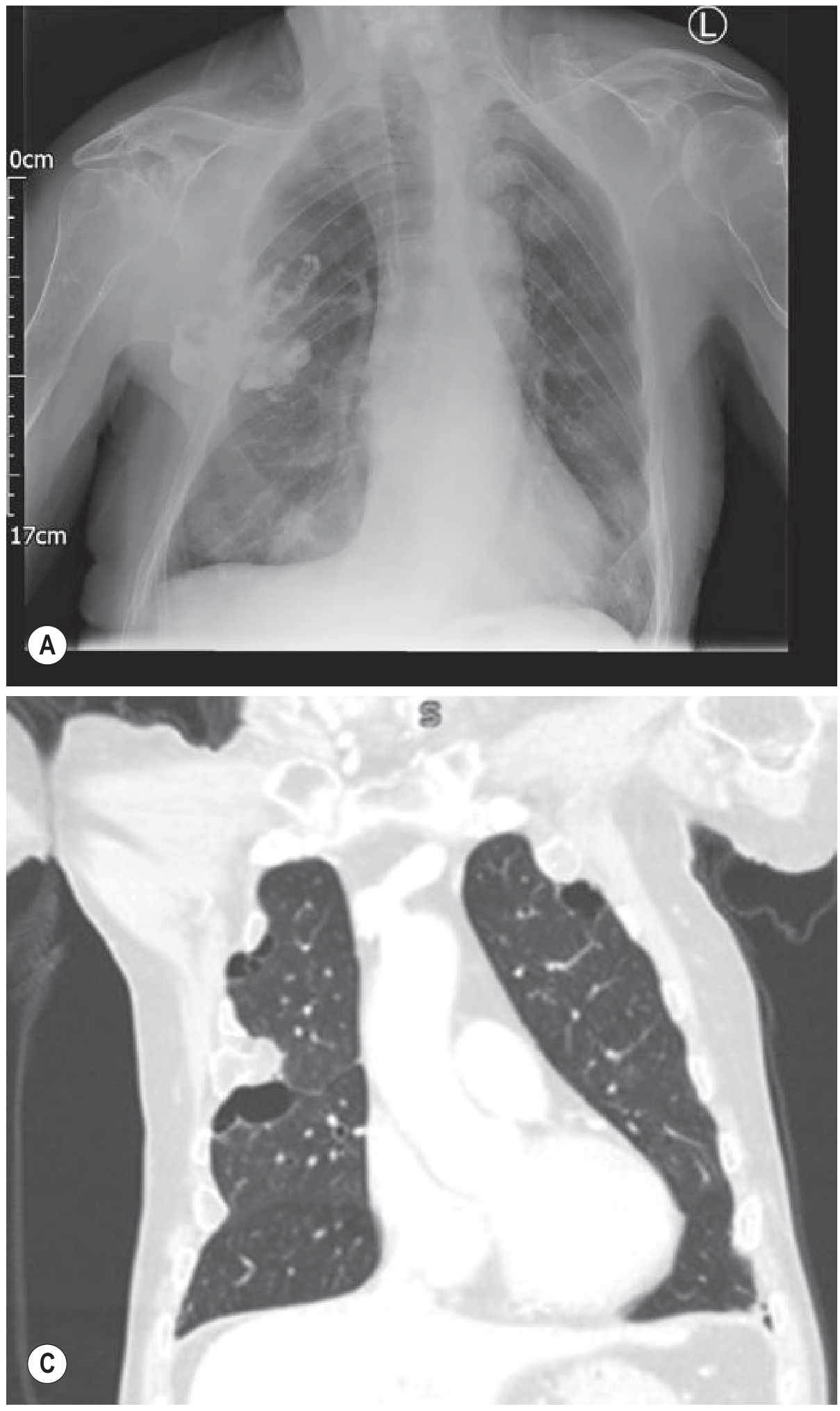
- Small effusion (<200–500 mL): initially subpulmonary/invisible; first sign is blunting of the posterior then lateral costophrenic angle
- Moderate effusion: homogeneous opacity with obliteration of the costophrenic angle and hemidiaphragm; meniscus sign (concave upper border, higher laterally)
- ~1000 mL: reaches the level of the 4th anterior rib
- Massive effusion: dense opacification with contralateral mediastinal shift
- Lateral decubitus view: fluid layers and the lung floats — increases sensitivity for small effusions
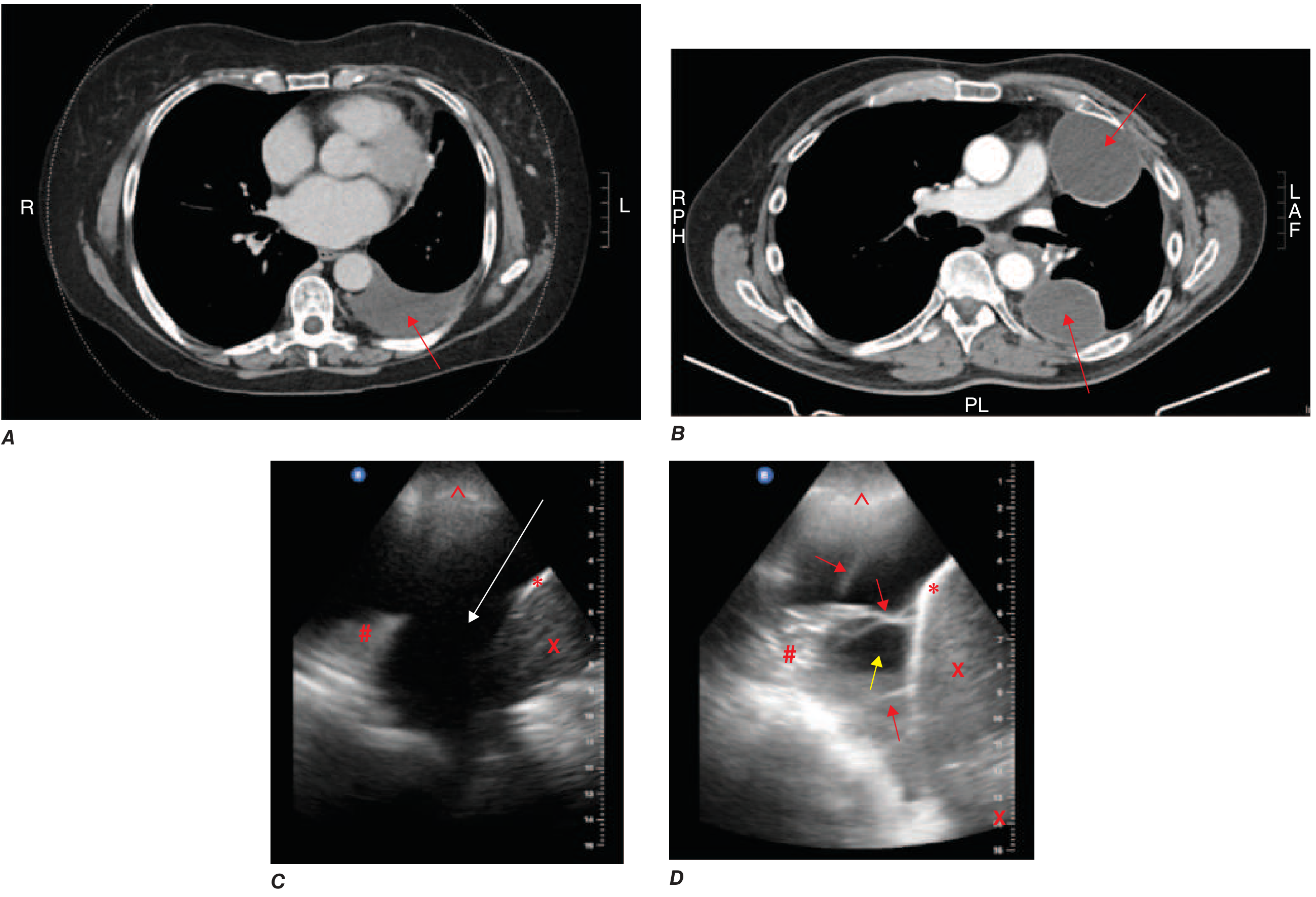
CT
- Distinguishes free vs. loculated fluid; identifies underlying lung/pleural pathology
- Split-pleura sign (parietal + visceral pleural enhancement): highly indicative of exudate (infection or malignancy)
- Cannot reliably distinguish transudate from exudate by CT number alone
Ultrasound
- Most sensitive bedside tool for small effusions
- Simple effusion: anechoic; complex/exudative: echogenic with mobile strands or septations
- Guides safe thoracentesis
Pleural Fluid Analysis (Thoracentesis)
Light's Criteria (sensitivity 98–99%, specificity 65–86%)
Fluid is an exudate if ≥1 of the following is present:
| Criterion | Threshold |
|---|---|
| Pleural fluid/serum protein ratio | >0.5 |
| Pleural fluid/serum LDH ratio | >0.6 |
| Pleural fluid LDH | >⅔ upper limit of normal serum LDH |
Diuresis caveat: Diuretics concentrate pleural protein, potentially misclassifying a transudate as exudate. Use the serum-to-pleural albumin gradient >1.2 g/dL in this setting (though sensitivity drops >10%).
Additional Tests
| Test | Clinical relevance |
|---|---|
| Cell count — neutrophils | Parapneumonic, PE, pancreatitis |
| Cell count — lymphocytes | Malignancy, TB, post-cardiac surgery |
| Glucose | Low in parapneumonic, malignant, TB, rheumatoid arthritis |
| pH | <7.20 → need for drainage; <7.10 → empyema likely |
| Amylase | Elevated in pancreatitis, oesophageal rupture |
| Cytology | Highest yield in adenocarcinoma; low in squamous cell, lymphoma, mesothelioma |
| NT-proBNP >1500 pg/mL | Suggests heart-failure-related effusion |
| Adenosine deaminase / IFN-γ / PCR | Tuberculosis |
| AFB smear/culture | Positive in only 25–30% of tuberculous effusions |
Parapneumonic Effusion — Indications for Evacuation
- Loculated pleural fluid
- Pleural fluid pH <7.20
- Pleural fluid glucose <3.3 mmol/L (<60 mg/dL)
- Positive Gram stain or culture
- Grossly purulent fluid (empyema)
- Elevated LDH >900 IU/L
Management
General
- Therapeutic thoracentesis: indicated for dyspnoea at rest; drain 1.0–1.5 L; avoid >1.5 L acutely to prevent re-expansion pulmonary oedema
- Treat the underlying cause
Heart Failure
- Diuresis and optimisation of cardiac therapy resolves >80% within 2 weeks
- Diagnostic thoracentesis warranted if: unilateral, patient is febrile, or pleuritic pain present
Empyema
- Chest tube drainage mandatory
- Fibrinopurulent phase: consider intrapleural tPA (10 mg) + DNase (5 mg) if incomplete drainage
- Thoracoscopy with adhesion breakdown, or surgical decortication if above fails
Malignant Effusion
- Primarily symptomatic (disease is usually disseminated, not curable)
- Options: repeated thoracentesis, indwelling pleural catheter, pleurodesis
Hepatic Hydrothorax (Cirrhosis)
- Sodium restriction + diuretics (first-line)
- TIPS: initial response rate 70–80%, limited by long-term complications
- Video-assisted thoracoscopic surgery (VATS) for diaphragmatic repair + pleurodesis in refractory cases
- Indwelling pleural catheter as bridge to liver transplant or for palliation
Trapped Lung
- Fibrous visceral peel prevents re-expansion
- Suspected when: thick pleural rind on imaging, pneumothorax ex vacuo after thoracentesis, rapid recurrence
- Definitive treatment: surgical decortication
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Grainger & Allison's Diagnostic Radiology | Harrison's Principles of Internal Medicine 22e | Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.