jvp graph with pictures of every wave
Reading File
Finding Sources
Searching Images
jugular venous pulse JVP waveform a c v waves
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive breakdown of the Jugular Venous Pulse (JVP) waveform with images from multiple authoritative sources.
The JVP Waveform
The JVP reflects pressure changes in the right atrium and has 3 peaks (a, c, v) and 2 descents (x, y):
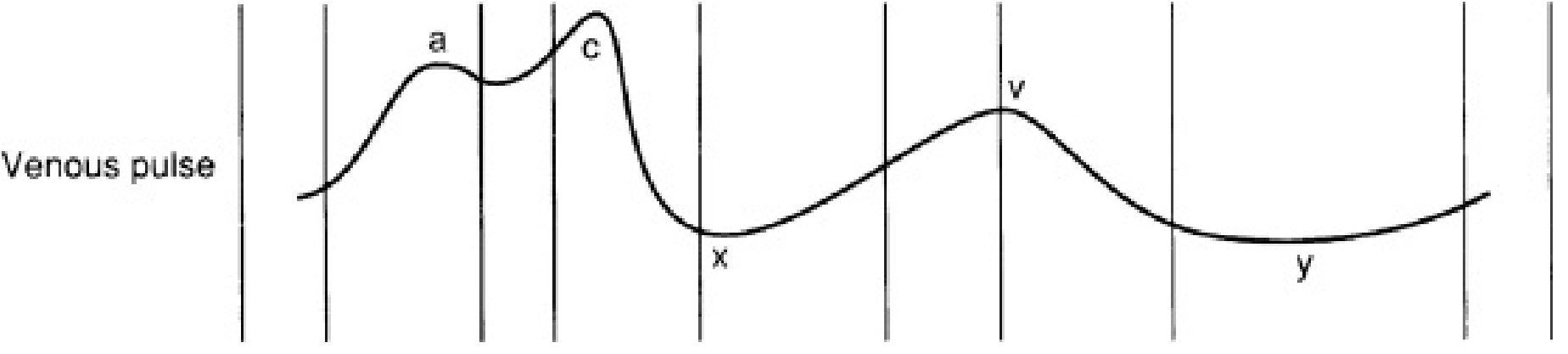
Each Component
🔺 a wave
- Cause: Right atrial presystolic contraction
- Timing: Just after the ECG P wave; precedes S1
- Normal a > v
- Absent in atrial fibrillation
- Prominent in: reduced RV compliance (e.g. pulmonary hypertension, pulmonary stenosis, RV hypertrophy)
- Cannon a waves: RA contracts against a closed tricuspid valve → seen in AV dissociation (ventricular tachycardia)
🔻 x descent
- Cause: Two overlapping events:
- Atrial relaxation (atrial diastole)
- Apical displacement of the tricuspid annulus during ventricular systole
- Interrupted mid-way by the c wave
- Prominent in: cardiac tamponade (preserved x, lost y)
- Absent in: tricuspid regurgitation (replaced by a positive deflection)
🔺 c wave
- Cause: Tricuspid valve bulging back into the right atrium during early isovolumetric ventricular systole (+ contiguous carotid pulsation artifact)
- Small and often not visible clinically — interrupts the x descent
🔺 v wave
- Cause: Venous return to the RA while the tricuspid valve is closed during ventricular systole (atrial diastole / passive filling)
- Peaks at S2
- Prominent (large v wave): Tricuspid regurgitation — v merges with c as TR worsens → "ventricullarized" waveform
🔻 y descent
- Cause: Tricuspid valve opens → rapid early diastolic filling of the RV
- Steep/rapid y: Tricuspid regurgitation, constrictive pericarditis (prominent x AND y → "W" or "M" pattern)
- Slow/blunted y: Tricuspid stenosis, cardiac tamponade
JVP with ECG Correlation & Pathological Variants
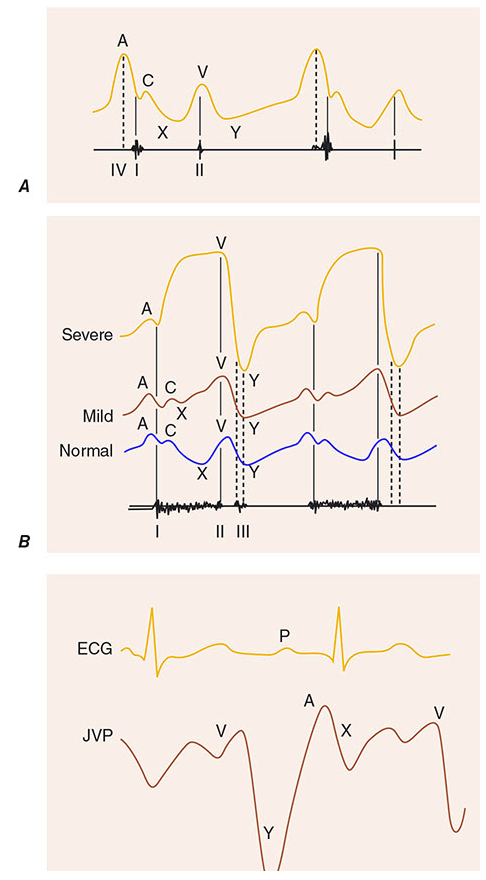
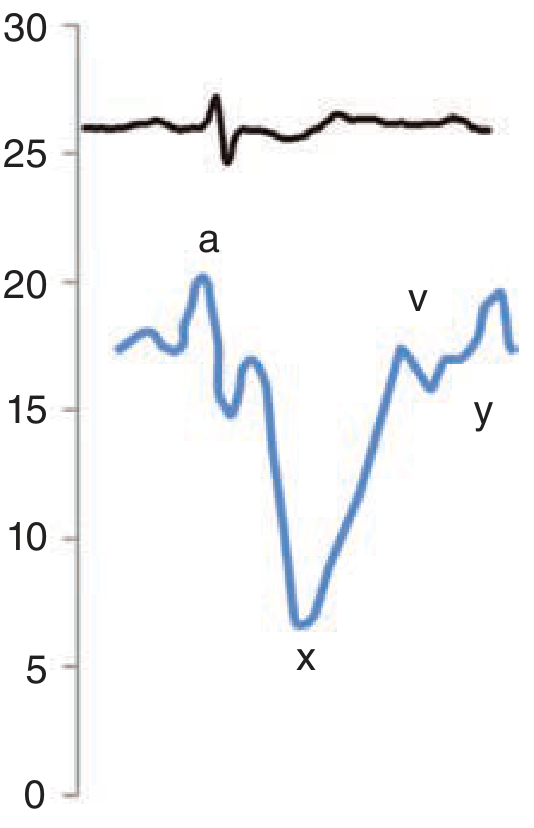
Normal JVP Waveform (Real-world tracing)
Quick Reference Table
| Component | Mechanism | Timing | Abnormalities |
|---|---|---|---|
| a wave | RA contraction | After P wave, before S1 | ↑ in PS, PHT, RVH; absent in AF; cannon waves in VT/AV dissociation |
| c wave | Tricuspid valve bulge into RA | After S1 | Often not clinically visible |
| x descent | Atrial relaxation + tricuspid annulus descent | Systole | Preserved (prominent) in tamponade; absent in TR |
| v wave | Passive RA filling during systole | Peaks at S2 | ↑↑ in tricuspid regurgitation; merges with c in severe TR |
| y descent | Tricuspid valve opens → RV fills | Early diastole | Steep in TR/constrictive pericarditis; slow/absent in TS/tamponade |
Key clinical rules:
- Tamponade → prominent x, absent y
- Constrictive pericarditis → prominent x AND y (Friedreich's sign)
- Tricuspid regurgitation → giant cv wave, steep y, absent x
- Tricuspid stenosis → giant a wave, slow y
- Atrial fibrillation → absent a wave
- Kussmaul's sign → JVP rises (or fails to fall) with inspiration → constrictive pericarditis, RV infarct, restrictive cardiomyopathy
— Fuster & Hurst's The Heart 15e, p. 85; Harrison's 22e, p. 1904; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.