Nephrotic syndrome
Reading File
Finding Sources
Searching Images
nephrotic syndrome pathology histology
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive information to provide a thorough answer. Let me compile it.
Nephrotic Syndrome
Definition
Nephrotic syndrome is a clinical syndrome characterized by the tetrad of:
- Proteinuria ≥ 3.5 g/day (in children: >50 mg/kg/24 h)
- Hypoalbuminemia (serum albumin < 3 g/dL)
- Generalized edema
- Hyperlipidemia and lipiduria
"Nephrotic syndrome classically presents with heavy proteinuria, minimal hematuria, hypoalbuminemia, hypercholesterolemia, edema, and hypertension." — Harrison's Principles of Internal Medicine, 22nd Ed.
Pathophysiology
The glomerular capillary wall (endothelium + GBM + podocytes) acts as both a size and charge barrier. Disruption of this barrier — whether structural or physicochemical — leads to protein leak into urine.
Cascade of consequences:
| Primary Event | Consequence |
|---|---|
| Glomerular barrier damage | Massive proteinuria |
| Loss of albumin faster than hepatic synthesis | Hypoalbuminemia |
| Reduced plasma oncotic pressure | Edema (underfill mechanism) |
| Primary renal sodium retention | Edema (overfill mechanism) |
| Hepatic lipoprotein overproduction + reduced catabolism | Hyperlipidemia |
| Lipoproteins crossing glomerular wall | Lipiduria (oval fat bodies, fatty casts) |
| Loss of immunoglobulins | Increased susceptibility to Streptococcus, Staphylococcus |
| Loss of antithrombin III and other anticoagulants | Hypercoagulable state → thromboembolism |
Patients with minimal change disease often have contracted plasma volume and stimulated RAAS, whereas other causes typically show expanded plasma volume and suppressed RAAS.
— Brenner and Rector's The Kidney, 2-Volume Set
Causes
Etiological Classification
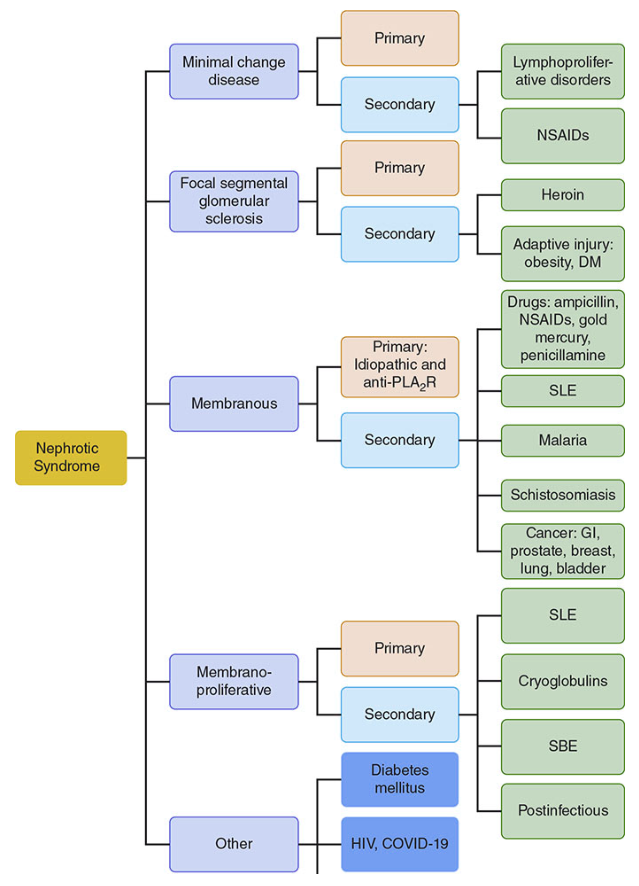
The relative frequency of causes differs by age:
| Age Group | Most Common Cause |
|---|---|
| Children (<17 yrs, North America) | Minimal change disease (70–90%) |
| Adults (United States) | FSGS (most common overall, esp. Hispanic and African descent) |
| Adults (global) | Membranous nephropathy (~25%) |
Major Histological Subtypes
1. Minimal Change Disease (MCD)
- Biopsy: Normal by light microscopy; no immune deposits on immunofluorescence
- EM: Diffuse effacement of podocyte foot processes — the hallmark
- Pathogenesis: Immune dysfunction (T-cell derived permeability factors — IL-13, IL-4); possible role for B-cell dysfunction (anti-nephrin antibodies); recent evidence for CD80 upregulation on podocytes
- Clinical: Abrupt onset of edema; average urine protein ~10 g/day; acellular urinary sediment
- Secondary causes: Hodgkin lymphoma, NSAIDs, lithium, viral infections
- Treatment: Highly steroid-responsive; second-line: cyclophosphamide, cyclosporine, rituximab
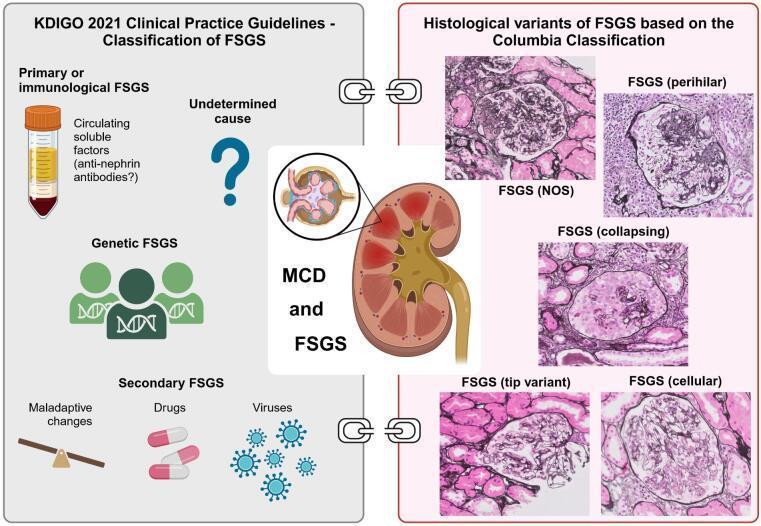
2. Focal Segmental Glomerulosclerosis (FSGS)
- Biopsy: Sclerosis affecting only a segment of only a subset of glomeruli (by definition)
- Pathogenesis: Primary diffuse podocytopathy; circulating permeability factor (recurs post-transplant in 30%)
- Primary FSGS: Circulating permeability factor
- Secondary FSGS: HIV, SARS-CoV-2, heroin, obesity/diabetes (adaptive hyperfiltration injury)
- Genetic FSGS: Mutations in podocin (NPHS2), nephrin (NPHS1), others
- Treatment: Steroids for primary; treat underlying cause in secondary/genetic forms; plasmapheresis for recurrent post-transplant FSGS
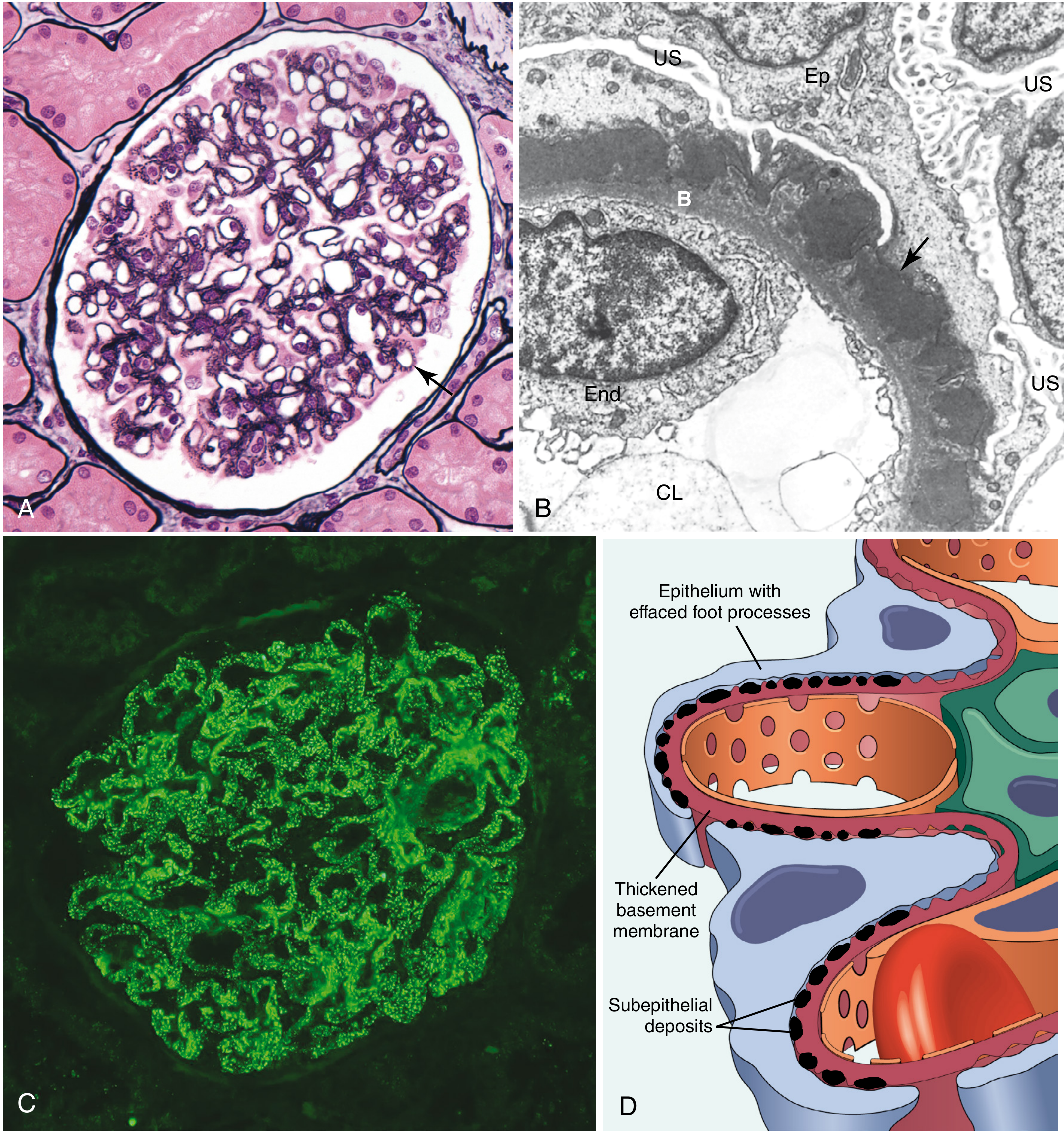
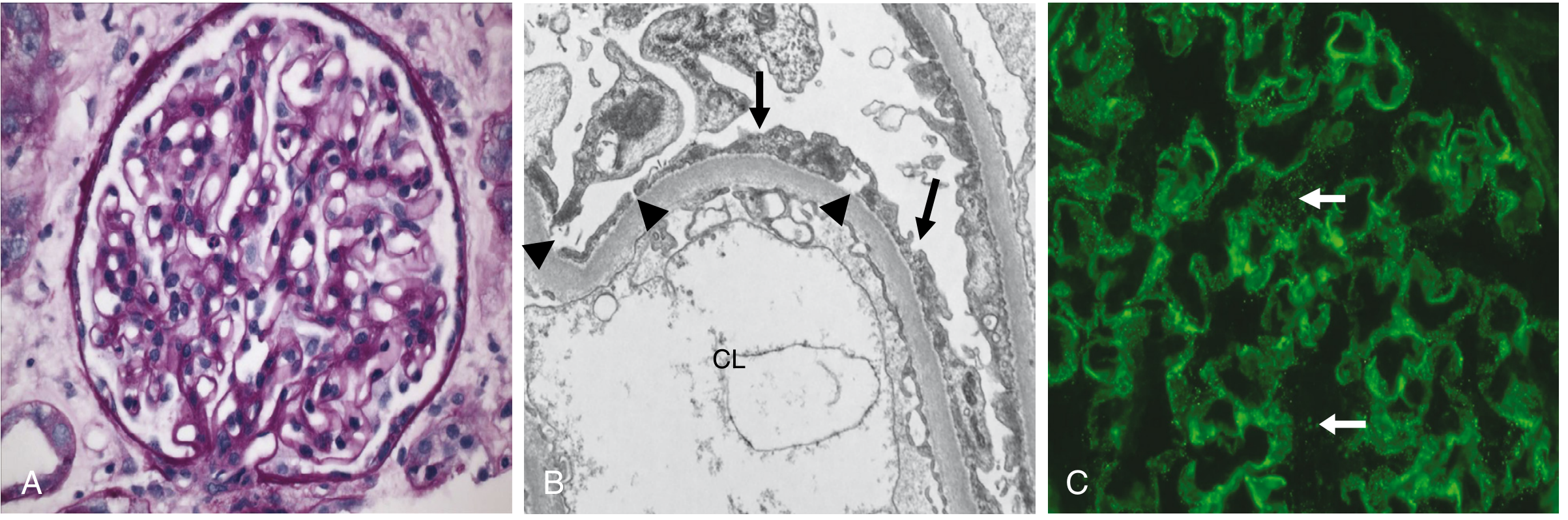
3. Membranous Nephropathy (MGN)
- Biopsy:
- Light microscopy: Uniform thickening of peripheral capillary loops; "spikes" on silver stain
- Immunofluorescence: Diffuse granular IgG + C3 deposits
- EM: Subepithelial electron-dense deposits
- Pathogenesis (primary): IgG₄ autoantibodies against M-type phospholipase A₂ receptor (PLA₂R) on podocytes in 70–80% of primary cases; anti-PLA₂R positivity + normal creatinine may now obviate biopsy
- Secondary causes: Malignancy (GI, lung, breast), hepatitis B, syphilis, malaria, SLE, drugs (gold, penicillamine, NSAIDs)
- Prognosis: 20–33% spontaneous remission; ~1/3 maintain stable function with relapsing nephrotic syndrome; ~1/3 develop kidney failure
- Worst prognosis: Male gender, older age, hypertension, persistent nephrotic-range proteinuria
- Highest incidence of renal vein thrombosis and pulmonary embolism among nephrotic syndromes
- Treatment: RAS inhibition + SGLT2i; immunosuppression (steroids + cyclophosphamide, CNIs, or rituximab) for persistent proteinuria
4. Membranoproliferative GN (MPGN)
- Secondary to SLE, cryoglobulins, subacute bacterial endocarditis (SBE), or primary
Clinical Features
| Feature | Detail |
|---|---|
| Edema | Soft, pitting; periorbital (especially in morning), dependent — can progress to anasarca, pleural effusions, ascites |
| Proteinuria | ≥3.5 g/day; dipstick 3–4+ |
| Hypoalbuminemia | < 3 g/dL |
| Hyperlipidemia | Elevated cholesterol, TG, VLDL, LDL, Lp(a); reduced HDL |
| Lipiduria | Oval fat bodies, fatty casts ("Maltese cross" appearance) |
| Hypertension | Frequently present |
| Hypercoagulability | Due to loss of antithrombin III, protein C, protein S |
| Infections | Loss of IgG → susceptibility to encapsulated organisms |
Complications
- Thromboembolism: Renal vein thrombosis, DVT, pulmonary embolism — driven by urinary loss of antithrombin III, protein C, protein S
- Infections: Especially pneumococcal peritonitis and staphylococcal infections (loss of IgG); children should receive pneumococcal (23-valent) vaccine in remission
- Cardiovascular disease: Accelerated atherosclerosis from prolonged hyperlipidemia
- Progressive renal failure: Higher 24-h urine protein → faster GFR decline
- Endocrine/metabolic: Loss of thyroid-binding globulin → altered TFTs; loss of vitamin D–binding protein → vitamin D deficiency
Diagnosis
Laboratory workup:
- Urinalysis: Proteinuria (dipstick + 24-h collection or protein:creatinine ratio), lipiduria
- Serum: Albumin, lipids, creatinine, electrolytes, complement levels (C3/C4), ANA, hepatitis B/C serology, ANCA, anti-PLA₂R
- CBC, coagulation studies
Biopsy indications:
- Adults: Almost always indicated (to guide specific therapy)
- Children: Not needed at first episode (assume MCD, treat empirically with steroids)
- Early biopsy in children if: age <1 yr, steroid resistance, hematuria, hypocomplementemia, elevated creatinine
Management
Supportive (all patients)
| Intervention | Rationale |
|---|---|
| Sodium restriction (<2 g/day) | Reduce edema |
| Loop diuretics (furosemide) | Treat edema; caution with hypoalbuminemia (altered pharmacokinetics) |
| ACE inhibitor / ARB | Reduce proteinuria, slow GFR decline |
| SGLT2 inhibitors | Reduce proteinuria, cardio-renoprotection (newer evidence) |
| Statins | Treat hyperlipidemia; reduce cardiovascular risk |
| Anticoagulation | Consider in high-risk patients (low albumin, membranous nephropathy) |
Disease-specific (immunosuppressive)
| Cause | First-Line | Second-Line |
|---|---|---|
| MCD | Prednisone 1 mg/kg/day | Cyclophosphamide, cyclosporine, tacrolimus, rituximab |
| Primary FSGS | Steroids ± CNI | Mycophenolate, rituximab |
| Primary MGN | Rituximab or steroids + cyclophosphamide | CNIs (cyclosporine/tacrolimus) |
| Secondary causes | Treat underlying disease | RAS inhibition |
Steroid dosing (pediatric): Prednisone 2 mg/kg/day (max 60 mg/day) or 60 mg/m²/day; continue for weeks to months per guidelines.
Key Differentiators: Nephrotic vs. Nephritic
| Feature | Nephrotic | Nephritic |
|---|---|---|
| Proteinuria | Massive (>3.5 g/day) | Mild–moderate |
| Hematuria | Minimal/absent | Prominent (RBC casts) |
| Hypertension | Variable | Common |
| Edema | Prominent | Present |
| GFR | Often preserved initially | Often reduced |
| Pathology | Podocyte injury dominant | Inflammatory/proliferative |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine, 22nd Ed.; Brenner and Rector's The Kidney; Tintinalli's Emergency Medicine; Swanson's Family Medicine Review
Also add histological and immunochemical pictures
Searching Images
minimal change disease light microscopy electron microscopy foot process effacement
Searching Images
focal segmental glomerulosclerosis FSGS histology light microscopy
Searching Images
membranous nephropathy silver stain spikes immunofluorescence IgG
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Great addition. Here are histologic and immunochemical images you can append directly to your nephrotic syndrome notes.
Histological and Immunochemical Pictures
1) Membranous nephropathy (classic pathology set)
- Silver stain: capillary wall thickening and spikes
- EM: subepithelial electron-dense deposits
- IF: granular capillary loop IgG pattern
2) Minimal change disease (MCD)
- Light microscopy: often near-normal glomerulus
- EM: diffuse podocyte foot process effacement (key lesion)
- IF: typically negative or minimal nonspecific staining
3) FSGS histologic variants (Columbia classification)
- NOS, perihilar, collapsing, tip, cellular variants
4) Primary membranous nephropathy immunochemistry
- Co-localization of PLA2R (red) with IgG/IgG subclasses (green), merged yellow signal along glomerular capillary loops
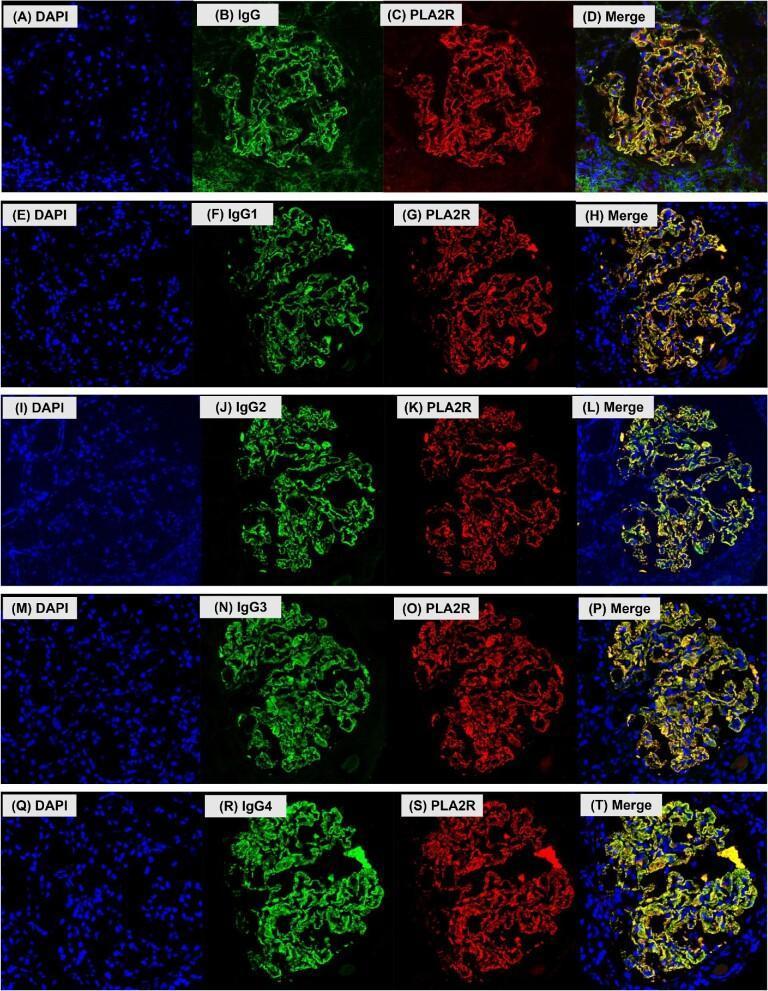
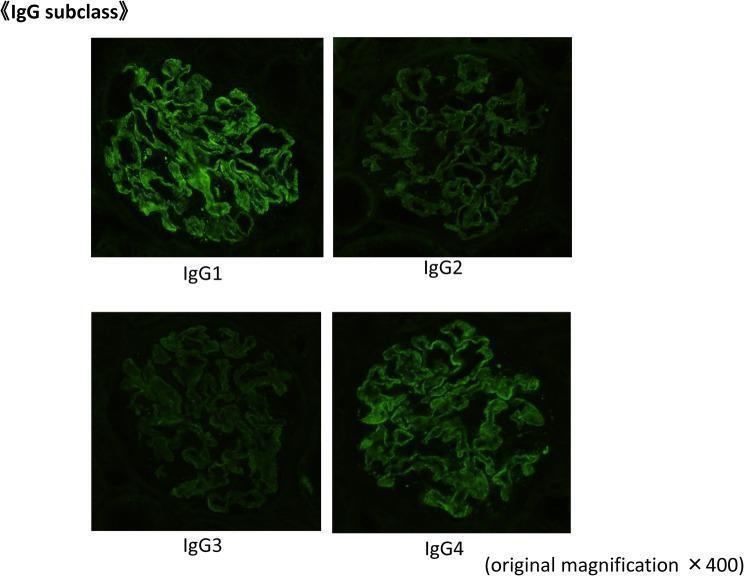
5) IgG subclass immunofluorescence panel
- Shows subclass distribution (IgG1–IgG4) in glomerular deposits
- Useful when distinguishing primary vs secondary membranous patterns
If you want, I can now create a clean one-page “pathology atlas” layout (MCD vs FSGS vs membranous) with captions under each image for exam prep.
Also add histological and immunochemical pictures
Histological pictures
Membranous nephropathy (LM + EM + IF)
Minimal change disease (LM near-normal, EM foot process effacement)
FSGS histologic variants (Columbia classification)
Immunochemical pictures
PLA2R and IgG subclass co-localization in membranous nephropathy
IgG subclass immunofluorescence panel (IgG1–IgG4)
If you want, I can next label each image with a short “what to look for” line for quick viva/exam recall.
Sure and integrate it with each type of nephrotic syndrome
Nephrotic syndrome types integrated with histology and immunochemistry
1) Minimal Change Disease (MCD)
What to look for
- LM: glomeruli usually look normal or near-normal
- EM: diffuse podocyte foot process effacement (most important finding)
- IF: typically negative or only minimal nonspecific staining
Quick recall
- Most common nephrotic syndrome in children
- Steroid responsive in many cases
2) Focal Segmental Glomerulosclerosis (FSGS)
What to look for
- LM: sclerosis in some glomeruli (focal) and part of tuft (segmental)
- Histologic variants: NOS, perihilar, collapsing, tip, cellular
- EM: variable foot process effacement (often extensive in primary FSGS)
- IF: often nonspecific IgM/C3 trapping in sclerotic segments
Quick recall
- Common adult cause (especially in some populations)
- Can be primary, secondary, or genetic
- More steroid resistance than MCD
3) Membranous Nephropathy (MN)
What to look for
- LM (silver stain): diffuse capillary wall thickening with spikes
- EM: subepithelial electron-dense deposits
- IF: granular capillary loop IgG/C3 pattern
Immunochemical hallmark (primary MN)
- PLA2R-associated immune deposits
- IgG subclass pattern often IgG4-dominant in primary disease
Quick recall
- Common adult nephrotic syndrome
- Primary (PLA2R/THSD7A-related) or secondary (SLE, infection, malignancy, drugs)
One-line exam map
- MCD = normal LM + foot process effacement on EM + usually negative IF
- FSGS = focal/segmental sclerosis on LM + variable IF trapping (IgM/C3)
- MN = spike-and-dome pattern (LM/EM) + granular IgG/C3 IF + PLA2R association in primary MN
If you want, I can convert this into a single high-yield comparison table (clinical + LM + EM + IF + key marker + treatment response).
This is a shared conversation. Sign in to Orris to start your own chat.