Ida vs megaloblastic anemia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have comprehensive textbook content and both peripheral smear images. Here is the full detailed comparison:
Iron Deficiency Anemia (IDA) vs. Megaloblastic Anemia
Core Mechanism - The Fundamental Difference
| IDA | Megaloblastic Anemia | |
|---|---|---|
| Core defect | Inadequate iron for hemoglobin synthesis | Impaired DNA synthesis (defective nuclear maturation) |
| Nutrient deficient | Iron | Vitamin B12 and/or Folate |
| RBC size | Microcytic (MCV < 80 fL) | Macrocytic (MCV > 100 fL) |
| RBC color | Hypochromic | Normochromic (appear hyperchromic but MCHC is not elevated) |
| Hematopoiesis problem | Reduced hemoglobin per cell | Ineffective hematopoiesis (apoptosis in marrow) |
Pathophysiology
IDA
Iron is required to synthesize hemoglobin. When iron is depleted, erythroid precursors undergo extra divisions trying to accumulate enough hemoglobin before maturing, producing small, pale cells. The sequence progresses through three stages:
- Storage iron depletion - Serum ferritin falls (below 12 µg/L), marrow iron disappears
- Iron-deficient erythropoiesis - Serum iron falls, TIBC rises, transferrin saturation drops below 15%
- Iron deficiency anemia - Hemoglobin and hematocrit fall; microcytic, hypochromic cells appear in peripheral blood
Hepcidin, the master regulator of iron homeostasis, falls in IDA (allowing maximum iron absorption), in contrast to anemia of chronic inflammation where hepcidin rises and traps iron in macrophages. - Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 613-615
Megaloblastic Anemia
B12 and folate are both cofactors for thymidine synthesis. Deficiency causes impaired DNA production, but cytoplasmic/RNA maturation continues normally - creating nuclear-to-cytoplasmic asynchrony. Cells grow large but cannot divide efficiently, undergo intramedullary apoptosis, and cause pancytopenia. The key biochemical pathway:
B12 deficiency → N5-methyl FH4 "trap" → FH4 deficit → impaired dUMP-to-dTMP conversion → defective DNA synthesis
B12 deficiency also impairs methylmalonyl-CoA → succinyl-CoA conversion, elevating methylmalonic acid - this distinguishes B12 deficiency from folate deficiency. - Robbins, Cotran & Kumar, p. 609
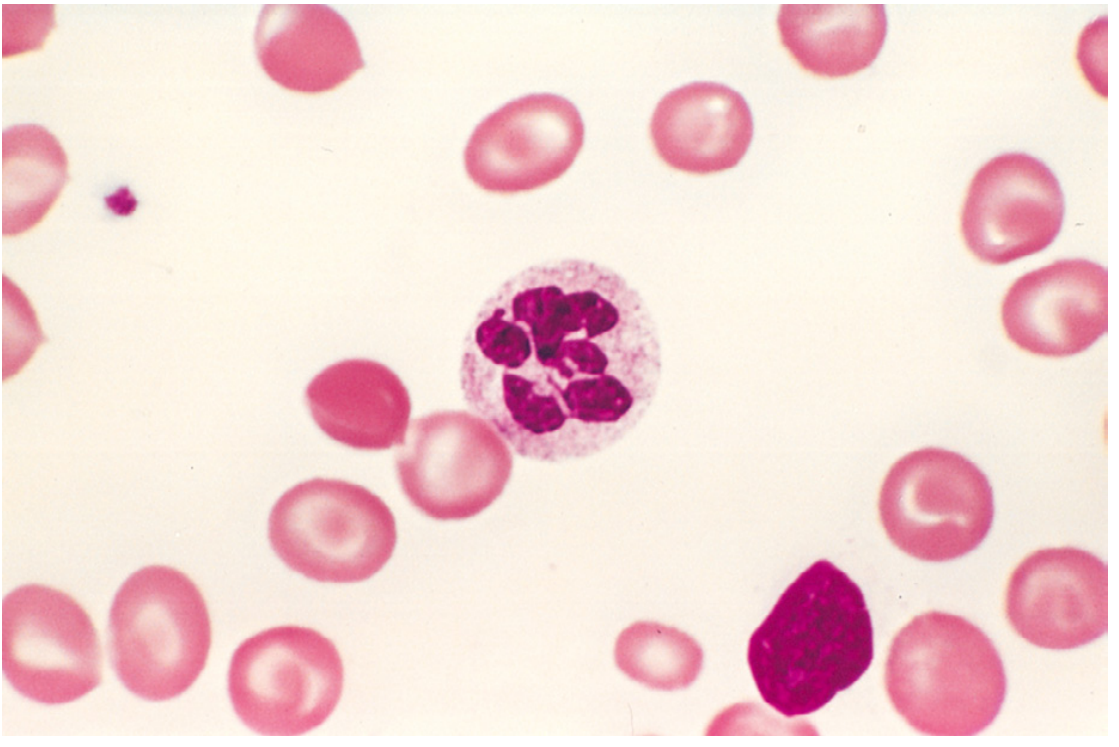
Peripheral Blood Smear
IDA Smear

Megaloblastic Anemia Smear
Clinical Features Compared
| Feature | IDA | Megaloblastic Anemia |
|---|---|---|
| Fatigue, pallor | Yes | Yes |
| Glossitis | Atrophic glossitis | Beefy red (Hunter's glossitis) |
| Nails | Koilonychia (spoon nails) | Normal |
| Pica | Yes (pagophagia, geophagia) | No |
| Neurological symptoms | Rare (restless legs) | Yes - in B12 deficiency only: subacute combined degeneration of spinal cord (posterior + lateral columns); paresthesias, ataxia |
| Plummer-Vinson syndrome | Yes (esophageal webs + IDA + atrophic glossitis) | No |
| GI symptoms | Usually related to the source of bleeding | Nausea, diarrhea |
| Jaundice | No | Mild (from ineffective erythropoiesis) |
Laboratory Findings
| Test | IDA | Megaloblastic Anemia |
|---|---|---|
| MCV | Low (< 80 fL) - microcytic | High (> 100 fL) - macrocytic |
| MCH/MCHC | Low (hypochromic) | Normal (MCHC not elevated despite hyperchromic appearance) |
| Peripheral smear | Microcytic, hypochromic; pencil cells, target cells | Macro-ovalocytes, hypersegmented neutrophils (≥5 lobes) |
| Reticulocyte count | Low | Low |
| Serum iron | Low | Normal/High |
| TIBC | High (elevated transferrin) | Normal |
| Transferrin saturation | < 15% | Normal |
| Serum ferritin | Low (< 12 µg/L) | Normal/High |
| Serum B12 | Normal | Low (if B12 deficiency) |
| Serum folate / RBC folate | Normal | Low (if folate deficiency) |
| Serum homocysteine | Normal | Elevated (both B12 and folate deficiency) |
| Methylmalonic acid (MMA) | Normal | Elevated in B12 deficiency only; normal in folate deficiency |
| Bone marrow | Depleted iron stores; micronormoblasts | Hypercellular; megaloblasts with nuclear-cytoplasmic asynchrony; giant metamyelocytes |
| CBC | Usually isolated anemia | Pancytopenia (anemia + leukopenia + thrombocytopenia) |
| LDH / bilirubin | Normal | Elevated (ineffective erythropoiesis) |
| Hepcidin | Low | Normal |
Etiology
IDA Causes (4 categories)
- Dietary lack - poverty, infants (breast milk is iron-poor), strict vegetarianism, elderly
- Impaired absorption - celiac disease, post-gastrectomy, H. pylori gastritis, proton pump inhibitors
- Increased demand - pregnancy, infancy, adolescence (especially females)
- Chronic blood loss (most common in adults) - GI bleeding (peptic ulcer, colorectal cancer, hookworm), menorrhagia
Megaloblastic Causes
B12 deficiency:
- Pernicious anemia (autoimmune destruction of gastric parietal cells → no intrinsic factor)
- Strict vegetarianism/veganism (B12 only in animal products)
- Gastrectomy, ileal resection, ileitis
- Fish tapeworm (Diphyllobothrium latum - competitive uptake)
- Bacterial overgrowth (blind loop syndrome)
Folate deficiency:
- Poor diet, alcoholism (most common)
- Pregnancy (increased demand)
- Malabsorption (celiac, tropical sprue)
- Drugs: methotrexate, phenytoin, oral contraceptives, trimethoprim
- Hemodialysis (folate loss)
Key Distinguishing Points (Memory Aids)
- MMA elevated = B12 deficiency (not folate) - the single most specific test to separate the two
- Neurological features = B12 deficiency only - folate does NOT cause subacute combined degeneration
- Folate treats the anemia of B12 deficiency but worsens the neuropathy - always rule out B12 deficiency before giving folate alone
- Schilling test (now largely historical) - differentiated pernicious anemia from other B12 malabsorption causes
- Anti-intrinsic factor antibodies - highly specific for pernicious anemia
- Hypersegmented neutrophil (≥5 lobes or ≥1 cell with 6+ lobes) - pathognomonic for megaloblastic process
Treatment
| IDA | Megaloblastic Anemia | |
|---|---|---|
| First-line | Oral ferrous sulfate (ferrous salts) 3-6 months; address underlying cause | IM/oral B12 (cyanocobalamin or hydroxocobalamin) for B12 deficiency; oral folic acid 1-5 mg/day for folate deficiency |
| Response monitoring | Reticulocytosis in 5-7 days; Hb normalizes in 6-8 weeks | Reticulocytosis within 5-7 days of treatment |
| Pernicious anemia | N/A | IM B12 lifelong (absorption is the problem) |
| Caution | Rule out underlying GI malignancy in adults | Never treat with folate alone without excluding B12 deficiency |
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.), Chapter 14, p. 608-615
This is a shared conversation. Sign in to Orris to start your own chat.