Chronic diseases of the larynx. Foreign bodies of larynx. trachea. bronchi. esophagus. Intubation and 'T'rachcostomy.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile the full response.
Chronic Diseases of the Larynx — Foreign Bodies of the Larynx, Trachea, Bronchi, Esophagus — Intubation and Tracheostomy
PART 1: CHRONIC DISEASES OF THE LARYNX
1. Chronic Laryngitis
Definition: Chronic laryngitis is diagnosed after >3 weeks of continuous symptoms. It is not a single entity but a spectrum of conditions from persistent mucosal inflammation to structural vocal fold changes.
Causes:
- Gastroesophageal/laryngopharyngeal reflux (most common chronic cause)
- Voice overuse, misuse, or abuse (phonotrauma)
- Tobacco smoke, dust, and polluted air
- Thermal and chemical irritants
- Chronic allergic reactions
- Prolonged use of inhaled corticosteroids (risk for fungal laryngitis)
Clinical features: Hoarseness, globus sensation, excessive throat clearing, vocal fatigue, chronic cough. More than 60% of patients with reflux laryngitis do not have classic heartburn.
Management: Treat the underlying cause — voice therapy, proton pump inhibitors for reflux, avoidance of irritants. Symptoms persisting >2 weeks or in immunocompromised patients warrant otolaryngology referral.
— Rosen's Emergency Medicine, p. 959; Cummings Otolaryngology, p. 1144; Histology: A Text and Atlas, p. 1776
2. Chronic Bacterial Laryngitis
Rare but potentially severe. Superinfection may complicate intubation injuries or underlying disease (e.g. relapsing polychondritis). Staphylococcus aureus is the most common pathogen, causing purulent chondritis with prolonged hoarseness and stridor lasting >1 month. Treatment requires surgical drainage plus prolonged antibiotics.
— Cummings Otolaryngology, p. 1144
3. Chronic Fungal Laryngitis
Candidal laryngitis: The most common fungal infection of the larynx. Characteristic finding is diffuse whitish speckling of the vocal folds (similar to oropharyngeal thrush). Risk factors: inhaled corticosteroids, broad-spectrum antibiotics, immunosuppression.
- The differential for white vocal fold lesions includes hyperkeratosis, thick mucus, malignancy, and Candida.
- Treatment: fluconazole (systemic for laryngeal involvement); itraconazole for resistant strains.
Other endemic fungi causing chronic laryngeal disease:
| Organism | Epidemiology | Key Feature | Treatment |
|---|---|---|---|
| Blastomyces | Southern USA | Broad-based budding yeast; mimics carcinoma | Amphotericin B, itraconazole |
| Paracoccidioides | South America | Ulcerative/exophytic lesions | Systemic antifungals |
| Histoplasma | Ohio/Mississippi valleys | Rare; mostly immunocompromised | Amphotericin B |
Note: All fungal laryngeal lesions can mimic squamous cell carcinoma — biopsy with fungal stains is essential.
— Cummings Otolaryngology, pp. 1143–1145
4. Laryngeal Tuberculosis
Patients with or without disseminated TB may develop laryngeal disease. Histology shows classic caseating/non-caseating granuloma formation.
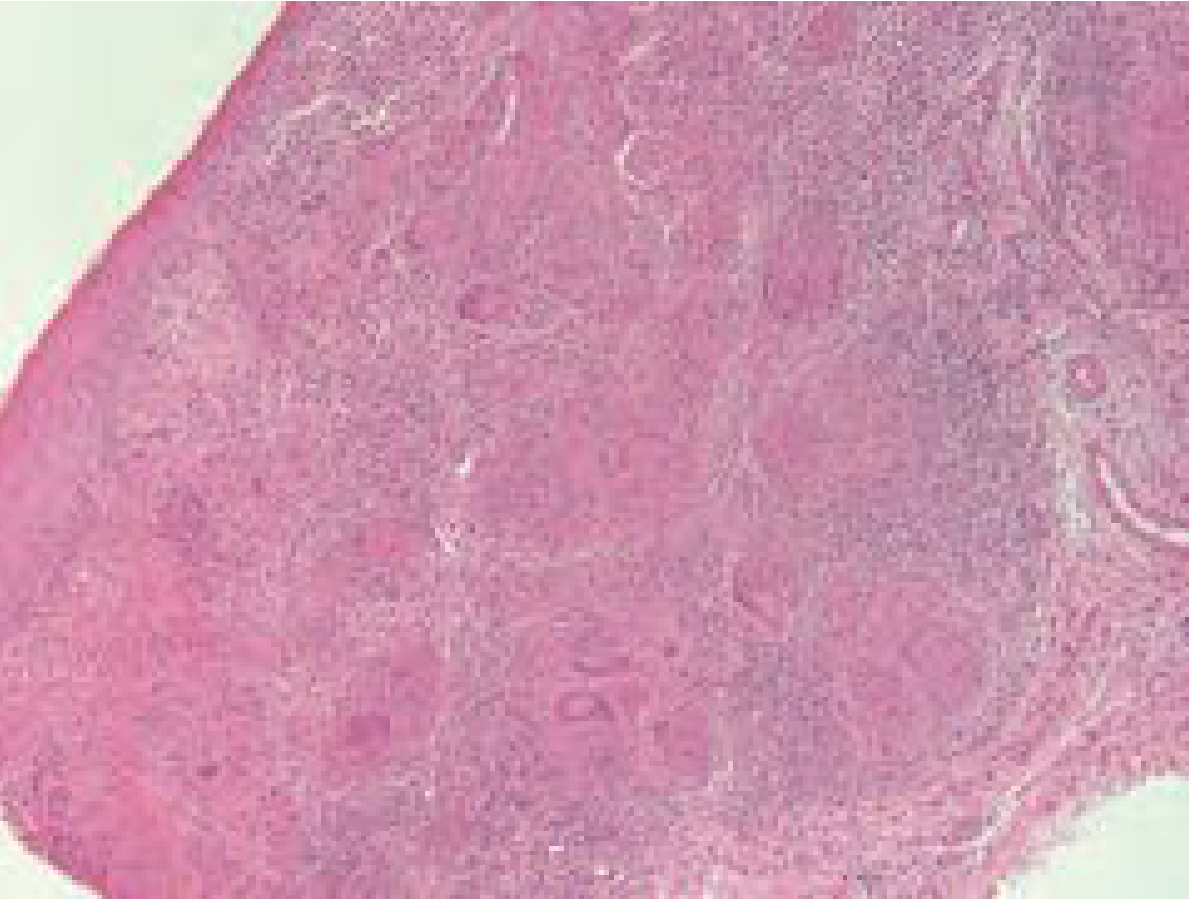
H&E stain of laryngeal tuberculosis showing granuloma formation — Cummings Otolaryngology
- Presentation: hoarseness, dysphagia, odynophagia, stridor
- Diagnosis: laryngoscopy + biopsy + AFB staining/culture
- Treatment: standard anti-TB therapy (isoniazid, rifampicin, pyrazinamide, ethambutol)
5. Autoimmune and Systemic Inflammatory Diseases of the Larynx
Granulomatosis with Polyangiitis (GPA / Wegener's)
- Small- and medium-vessel vasculitis; autoantibodies against proteinase 3 (c-ANCA)
- 90% have head and neck manifestations; subglottic stenosis is the most common laryngeal manifestation (20%)
- Treatment: endoscopic dilation or open resection + immunosuppression
Relapsing Polychondritis
- Autoimmune; autoantibodies against type II collagen
- 25–50% have laryngeal symptoms (hoarseness, cough, pain, potentially fatal airway obstruction)
- Treatment: medical and surgical combination
Pemphigus Vulgaris / Pemphigoid
- Up to 80% of pemphigus patients have ORL symptoms; 40% laryngeal
- Severe epithelial loss from intraepithelial (pemphigus) or subepithelial (pemphigoid) autoantibodies
- Treatment: high-dose corticosteroids + immunosuppressives
Sarcoidosis
- Laryngeal involvement in <1% of cases; usually supraglottic and glottic edema
- Diagnosis by histology (non-caseating granulomas)
- Treatment: systemic corticosteroids
— Cummings Otolaryngology, pp. 1146–1147
6. Iatrogenic Laryngeal Injury (Intubation Granuloma / Stenosis)
Acute injuries: edema, granulation tissue, ulceration, arytenoid dislocation
Chronic injuries: fibrotic scar, granulation tissue, arytenoid fixation, subglottic stenosis
Emergency cricothyroidotomy and high tracheotomy are particularly associated with severe subglottic stenosis, especially in children.
7. Laryngocele
- Formed by increased intraglottic pressure (horn players, glass blowers) or obstruction of the laryngeal ventricle
- Internal laryngocele: tracks within the paralaryngeal fat, may be air- or fluid-filled
- External (mixed) laryngocele: extends through thyrohyoid membrane → presents as neck mass
- CT appearance: air- or fluid-containing structure within or adjacent to the larynx
8. Recurrent Respiratory Papillomatosis (RRP)
- Caused by HPV (types 6 and 11)
- Warty growths on the laryngeal mucosa
- Managed with endoscopic debridement; adjuncts include cidofovir, indole-3-carbinol
- Annual biopsies to rule out malignant transformation
- Quadrivalent and 9-valent HPV vaccines have decreased the incidence of RRP
9. Paradoxical Vocal Fold Movement
- Vocal fold adduction on inspiration, abduction on expiration (opposite of normal)
- More common in females with social stressors; often misdiagnosed as asthma
- Associated with laryngopharyngeal reflux
- Diagnosis: flexible nasopharyngoscopy (may require exercise testing)
- Treatment: panting exercises, PPI, voice therapy, biofeedback; severe cases — heliox, botox, anticholinergics
— K.J. Lee's Essential Otolaryngology, pp. 1032–1033
PART 2: FOREIGN BODIES OF THE LARYNX, TRACHEA, BRONCHI, AND ESOPHAGUS
Epidemiology and General Principles
Foreign bodies of the aerodigestive tract occur predominantly in toddlers (the most common age group). The inherent curiosity of young children and their exploration of objects by mouth place them at risk.
- 80–90% of airway foreign bodies are found in the bronchi
- Tracheal or laryngeal foreign bodies are less common but more immediately dangerous
- A tracheal foreign body is more likely to cause complete airway obstruction and requires more urgent intervention than a bronchial foreign body
— Cummings Otolaryngology, p. 3982
Foreign Body Aspiration (Larynx, Trachea, Bronchi)
Common objects: Peanuts (most common aspirated FB), popcorn, seeds, small plastic parts
Pathophysiology:
- Peanut oil is chemically irritating → causes chemical bronchitis and pneumonia
- Vegetable/organic matter is associated with higher complication rates due to swelling and inflammatory response
- Solid foreign body causes air trapping → hyperlucency of affected lobe (especially on expiration)
Anatomic predilection: Right main stem bronchus or right lower lobe (due to more vertical orientation)
Clinical presentation:
- Initial cough or choking episode while eating, often followed by an asymptomatic interval
- Unilateral wheeze on auscultation (often misdiagnosed as asthma)
- Total respiratory obstruction if in trachea (rare but emergent)
Investigations:
- CXR: radiopaque FB seen directly; for radiolucent FB (nuts, seeds, plastic) → hyperexpansion of affected lobe on expiratory film or fluoroscopy
- CT chest (if diagnosis uncertain)
- Rigid bronchoscopy = gold standard for diagnosis and treatment
Treatment:
- Rigid bronchoscopy with optical forceps — may be simple or very difficult
- Epinephrine injection into mucosa if foreign body has been present long term (minimizes bleeding)
- Rarely: bronchiectasis from repeated infection may require partial/total lobe resection
Complications of bronchoscopy: Failure to remove, laryngeal edema, pneumothorax, pneumomediastinum, subcutaneous emphysema. Mortality: 0.2–1.0%.
— Schwartz's Principles of Surgery, p. 1743; Cummings Otolaryngology, p. 3981–3982
Foreign Bodies of the Esophagus
Most common objects:
- Coins (most common in children)
- Small toy parts
- Fish bones, meat boluses (adults)
Sites of lodgement — 4 areas of physiological narrowing:
- Upper esophageal sphincter (cricopharyngeus) — most common
- Level of the aortic arch
- Level of the left main bronchus
- Lower esophageal sphincter (gastroesophageal junction)
Clinical presentation:
- Often asymptomatic period after ingestion initially
- GI symptoms: dysphagia, drooling, dehydration
- Respiratory symptoms (if prolonged): cough, stridor, wheezing — may mimic upper respiratory infection
Investigations:
- CXR: diagnostic for coins (coronal plane — coin faces forward in esophagus vs. sagittal in trachea)
- Contrast swallow or esophagoscopy for non-radiopaque FB
Management:
| Situation | Management |
|---|---|
| Asymptomatic, healthy child, mid/distal FB, <24 hours | Observe 8–16 hours for spontaneous passage |
| Young child, FB >24 hours, symptomatic, sharp/caustic FB | Urgent endoscopic removal |
| Upper esophagus, <24 hours | Magill forceps during direct laryngoscopy |
| All other situations | Esophagoscopy (rigid or flexible) |
| Retained button battery | Surgical emergency (direct tissue necrosis, risk of TE fistula, aortic erosion, mediastinitis) |
| Spontaneous passage failure | Esophagotomy, gastrotomy, jejunotomy |
Coin spontaneous passage rate: 25–30% in asymptomatic children with recent ingestion (<24 hours) and no esophageal pathology.
Special hazard — Button batteries: The negative pole directly damages surrounding tissue through electrical current and chemical reaction; can cause tracheoesophageal fistula, aortic exsanguination, and mediastinitis. Treat as a surgical emergency.
— Cummings Otolaryngology, pp. 3982–3984; Schwartz's Principles of Surgery, p. 1744
PART 3: INTUBATION
Endotracheal Intubation — Complications
Acute complications:
- Pharyngeal or laryngeal lacerations
- Cricoarytenoid joint dislocation
- Neuropraxia of lingual, hypoglossal, and laryngeal nerves
- Arytenoid dislocation
Chronic complications:
- Granulation tissue, fibrotic scar
- Arytenoid fixation
- Subglottic stenosis — particularly dangerous in children; there is no duration of intubation below which this cannot occur
— Cummings Otolaryngology, p. 2901; K.J. Lee's Essential Otolaryngology, p. 1032
PART 4: TRACHEOSTOMY
Definition and Indication Categories
Tracheostomy is the most common surgical procedure in critically ill patients requiring prolonged mechanical ventilation. Indications fall into three broad categories:
- Upper airway obstruction (difficult airway, maxillofacial trauma, angioedema, tumors)
- Prolonged mechanical ventilation
- Neurologic condition preventing safe extubation (brain injury, spinal cord injury, severe agitation, altered mental status)
Indications and Contraindications
| INDICATIONS | CONTRAINDICATIONS (mostly relative) |
|---|---|
| Upper airway obstruction | Recent anterior neck surgery (<7 days) |
| Difficult airway | High ventilator settings (FiO₂ >50%, PEEP >10 cmH₂O) |
| Significant maxillofacial trauma | Elevated intracranial pressure |
| Angioedema | Hemodynamic instability |
| Upper airway tumors | Significant bleeding risk |
| Brain injury (acute or progressive) | Local infection or malignancy at proposed site |
| Spinal cord injury | Predicted early mortality |
| Prolonged mechanical ventilation |
Techniques
1. Open (Surgical) Tracheostomy
- Performed in the operating room
- Standard technique with direct visualization
2. Percutaneous Dilatational Tracheostomy (PDT)
- First described by Ciaglia (1985)
- Now widely performed at the bedside in the ICU
- Compared to open tracheostomy: decreased wound infection and clinically relevant bleeding; more cost-effective
- Periprocedural mortality: <0.2%
- Major complication rate: 0.15%
- Safety confirmed in >3000 consecutive procedures
- Guidance: bronchoscopic or semi-open technique with blunt dissection — both minimize loss of airway
Timing
- Controversial in predicted prolonged ventilation
- Most studies show no mortality difference between early (<7 days) vs. late (>7 days)
- One RCT showed significant benefit of early tracheostomy at 48h vs. 14–16 days (↓ mortality 32% vs. 62%, ↓ pneumonia)
- The largest RCT (TracMan, UK; >900 patients) showed no mortality difference between early (within 4 days) vs. late (after 10 days); >50% of late group never needed tracheostomy
Complications of Tracheostomy
Perioperative:
- Peristomal bleeding (anterior jugular veins or thyroid isthmus)
- Posterior tracheal wall laceration or esophageal injury
- Extraluminal placement (false tract)
- Loss of airway
Long-term:
- Tracheal stenosis (especially after emergency cricothyroidotomy in children)
- Tracheomalacia
- Persistent stoma
Tracheostomy Tube Sizing (Jackson Scale)
| Jackson Size | Inner diameter with inner cannula (mm) | Outer diameter (mm) |
|---|---|---|
| 4 | 5.0 | 9.4 |
| 6 | 6.4 | 10.8 |
| 8 | 7.6 | 12.2 |
| 10 | 8.9 | 13.8 |
Special Considerations
- COVID-19: Aerosol-generating procedure — airborne/droplet precautions required. Timing after 10–14 days of ventilation associated with shorter ventilation and ICU stay.
- ECMO patients: Tracheostomy can be safely performed, but complications (mostly bleeding) are higher; no difference between open and percutaneous technique.
— Sabiston Textbook of Surgery, pp. 960–962
Summary Table: Foreign Body Management
| Location | Most common FB | Key symptoms | Diagnosis | Treatment |
|---|---|---|---|---|
| Larynx | Food bolus, small objects | Sudden stridor, choking, aphonia | Direct laryngoscopy | Magill forceps / urgent removal |
| Trachea | Various | Respiratory distress, biphasic stridor | CXR + bronchoscopy | Rigid bronchoscopy (urgent) |
| Bronchus (right > left) | Peanuts, seeds | Unilateral wheeze, cough, asymp. interval | CXR (expiratory), bronchoscopy | Rigid bronchoscopy |
| Esophagus | Coin (children), meat (adults) | Dysphagia, drooling, cough | CXR, contrast swallow, endoscopy | Endoscopic removal; observe if asymptomatic <24h |
This is a shared conversation. Sign in to Orris to start your own chat.