Cardiovascular system examination
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive guide to the Cardiovascular System Examination, synthesized from Harrison's and Goldman-Cecil Medicine.
Cardiovascular System Examination
1. General Approach & Vital Signs
Before the focused cardiac exam, note:
- Pulse rate and rhythm — tachycardia, bradycardia, or irregularity
- Blood pressure (both arms) — a discrepancy suggests aortic dissection or atherosclerotic disease of the great vessels; if coarctation is suspected, measure in a leg as well
- Pulsus paradoxus — >10 mmHg drop in systolic BP on inspiration is typical of pericardial tamponade
- Respiratory rate — tachypnoea and laboured breathing suggest pulmonary oedema; Cheyne-Stokes respirations indicate advanced heart failure
General appearance may reveal clues: Marfan syndrome, Turner syndrome, Down syndrome, or systemic conditions like hyperthyroidism (exophthalmos), myotonic dystrophy (ptosis, AV block), or scleroderma.
2. Ophthalmologic Examination
| Finding | Association |
|---|---|
| Diabetic/hypertensive retinopathy | Diabetes, hypertension |
| Roth spots | Infective endocarditis |
| Retinal artery beading | Severe hypercholesterolaemia |
| Blue sclerae | Osteogenesis imperfecta → aortic dilation, MVP |
| Retinal artery occlusion | Left atrial thrombus, myxoma, atherosclerotic emboli |
| Exophthalmos | Hyperthyroidism |
3. Jugular Venous Pressure (JVP) & Waveform
The JVP is the single most important bedside measurement for estimating volume status. The internal jugular vein is preferred (the external jugular is valved and not directly in line with the SVC/RA). Venous pulsations above the clavicle in the sitting position are clearly abnormal (the clavicle-to-RA distance is ≥10 cm).
A distance >4.5 cm above the sternal angle (angle of Louis) at 30° elevation is considered elevated. Note: bedside estimates are in cmH₂O; convert to mmHg by dividing by 1.36.
JVP Waveform Components
| Component | Mechanism | Clinical pearl |
|---|---|---|
| a wave | Right atrial presystolic contraction (after P wave, before S1) | Absent in AF; cannon a wave = AV dissociation (VT vs SVT discriminator) |
| c wave | Tricuspid valve pushed into RA during early systole | Small, often not visible |
| x descent | Fall in RA pressure after tricuspid opens | Prominent in tamponade |
| v wave | Atrial filling during ventricular systole | Accentuated in tricuspid regurgitation |
| y descent | Tricuspid opens → ventricular filling | Rapid y descent in constrictive pericarditis; absent/blunted in tamponade |
Distinguishing venous from arterial pulsation: The venous waveform is usually biphasic (vs monophasic carotid), changes with posture and inspiration, and is obliterable with gentle pressure.
4. Arterial Pulse
Assess the carotid pulse for volume, contour, and timing:
| Pulse character | Significance |
|---|---|
| Pulsus bisferiens (double peak in systole) | Severe AR ± AS, HOCM |
| Pulsus alternans | Severe LV dysfunction |
| Pulsus paradoxus (>10 mmHg inspiratory drop) | Cardiac tamponade, severe asthma |
| Small, slow-rising (parvus et tardus) | Aortic stenosis |
| Bounding, collapsing | Aortic regurgitation, hyperdynamic states |
| Pulsus bigeminus | Bigeminal ectopy |
5. Precordial Inspection & Palpation
- Apex beat (Point of Maximal Impulse, PMI): Normally in the 5th intercostal space, mid-clavicular line. A laterally displaced impulse indicates LV dilatation; a sustained impulse suggests LV hypertrophy.
- Right ventricular heave/lift at the lower left sternal border suggests RV enlargement (e.g., pulmonary hypertension, RV failure).
- Thrills are palpable murmurs (grade ≥4/6) — felt over aortic/pulmonary areas or at the apex.
- A loud P2 that can be palpated at the 2nd left interspace suggests pulmonary hypertension.
6. Auscultation
Auscultatory Areas
- Aortic area — 2nd right intercostal space
- Pulmonary area — 2nd left intercostal space
- Tricuspid area — lower left sternal border
- Mitral area (apex) — 5th ICS, mid-clavicular line
First Heart Sound (S1)
- Caused by mitral (M1) and tricuspid (T1) valve closure
- Loud S1 → MS with pliable leaflets, hyperdynamic states
- Soft S1 → Long PR interval, severe MS with calcified leaflets, LV dysfunction
- Variable S1 → AF, complete heart block (cannon beat)
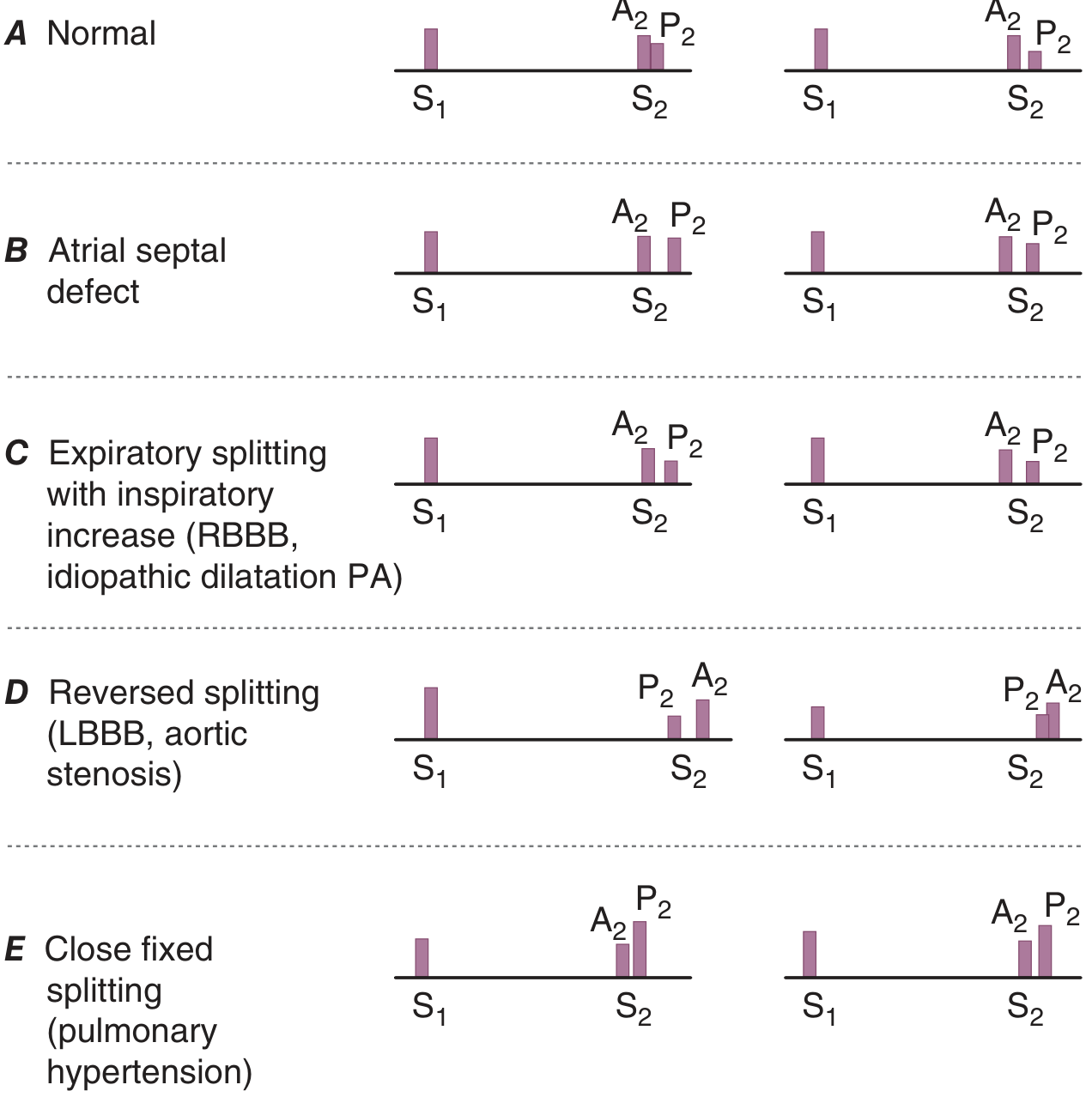
Second Heart Sound (S2)
- A2 (aortic closure) precedes P2 (pulmonary closure)
- Physiologic splitting: widens on inspiration (increased RV filling delays P2); narrows on expiration
| S2 Pattern | Cause |
|---|---|
| Fixed splitting | Atrial septal defect (ASD) |
| Wide splitting | RBBB, pulmonary stenosis |
| Reversed/paradoxical splitting | LBBB, RV pacing, severe AS, HOCM, acute ischaemia (components audible on expiration, narrow on inspiration) |
| Narrow/single S2 | Pulmonary hypertension (loud P2 ≥ A2) |
| Absent P2 | Severe pulmonary stenosis |
Added Sounds
Systolic:
- Ejection click (early systolic, high-pitched) → bicuspid aortic or pulmonary valve; pulmonic ejection sound is the only right-sided event that decreases with inspiration
- Non-ejection click (mid-systolic click) → MVP; click-murmur complex moves away from S1 on squatting (increased preload) and toward S1 on standing
Diastolic:
| Sound | Timing | Cause | Key feature |
|---|---|---|---|
| Opening snap (OS) | Early diastole, after S2 | Mitral stenosis | A2-OS interval inversely proportional to severity (shorter = higher LAP) |
| S3 (ventricular gallop) | Early diastole | Elevated LVEDP, severe LV dysfunction | Low-pitched, at apex; normal in young adults; correlated with poor prognosis |
| S4 (atrial gallop) | Late diastole (presystolic) | Reduced LV compliance (HTN, ischaemia) | Low-pitched; indicates diastolic dysfunction; absent in AF |
| Pericardial knock | Early diastole, after OS | Constrictive pericarditis | High-pitched; exaggerated y descent in JVP |
| Tumour plop | Diastolic | Atrial myxoma | Positional |
Heart Murmurs
Systolic murmurs:
| Murmur | Character | Best heard | Radiation | Dynamic clues |
|---|---|---|---|---|
| Aortic stenosis (AS) | Harsh, crescendo-decrescendo | 2nd RSB | Neck (carotids) | Louder with squatting; softer with Valsalva |
| HOCM | Crescendo-decrescendo | LLSB | — | Louder with Valsalva/standing; softer with squatting |
| Mitral regurgitation (MR) | Holosystolic, blowing | Apex | Axilla/back | — |
| Tricuspid regurgitation (TR) | Holosystolic | LLSB | — | Increases with inspiration (Carvallo's sign) |
| MVP | Late systolic ± click | Apex | — | Click moves to S1 on standing |
| VSD | Holosystolic, harsh | LLSB | — | — |
| Pulmonary stenosis | Ejection systolic | 2nd LSB | — | Ejection click that softens on inspiration |
Diastolic murmurs (always pathological):
| Murmur | Character | Best heard | Radiation | Dynamic clues |
|---|---|---|---|---|
| Aortic regurgitation (AR) | Early diastolic, blowing, decrescendo | 3rd LSB (leaning forward, expiration) | — | Austin Flint murmur at apex |
| Mitral stenosis (MS) | Mid-diastolic, low-pitched rumble | Apex (bell) | — | Louder with left lateral decubitus + exercise |
| Tricuspid stenosis (TS) | Mid-diastolic | LLSB | — | Increases with inspiration |
| Pulmonary regurgitation | Early diastolic | 2nd/3rd LSB | — | Graham Steell murmur in PAH |
Dynamic auscultation manoeuvres:
| Manoeuvre | Effect | Useful for |
|---|---|---|
| Valsalva (strain phase) | ↓ preload | HOCM louder; MVP click earlier; others softer |
| Squatting | ↑ preload + afterload | HOCM softer; MVP click later |
| Standing | ↓ preload | HOCM louder; MVP click earlier |
| Inspiration | ↑ RV filling | Right-sided murmurs louder (TR, TS, PS) |
| Leg raising | ↑ preload | Similar to squatting |
| Amyl nitrite | ↓ afterload | AS louder; AR softer |
| Handgrip | ↑ afterload | MR, AR, VSD louder; HOCM softer |
7. Peripheral Examination
Abdomen
- Hepatomegaly — right heart failure; an enlarged pulsatile liver = severe tricuspid regurgitation / markedly elevated right heart pressure
- Ascites — advanced right heart failure
- Abdominal aorta pulsation — screen for AAA in appropriate patients
Extremities
- Pitting oedema — dependent; graded 0–3+; from elevated right-sided filling pressures → increased hydrostatic pressure → transudation; must exclude other causes (calcium channel blockers, venous insufficiency, hypoproteinaemia)
- Cool extremities → low cardiac output or peripheral arterial disease
- Clubbing → cyanotic congenital heart disease, infective endocarditis
- Peripheral cyanosis → low cardiac output; central cyanosis (tongue) → right-to-left shunt, respiratory failure
- Splinter haemorrhages, Osler nodes, Janeway lesions → infective endocarditis
- Xanthelasma, corneal arcus → hyperlipidaemia
Summary: Structured Examination Sequence
- General appearance (dyspnoea, cyanosis, pallor, syndromic features)
- Vital signs (HR, BP both arms, RR, SpO₂)
- Hands (clubbing, cyanosis, splinters, peripheral pulses)
- Face/eyes (retinal changes, malar flush of MS, xanthelasma)
- Neck (JVP waveform and height, carotid pulse character)
- Precordium — inspect, palpate (apex, heaves, thrills), auscultate (S1, S2, added sounds, murmurs) with dynamic manoeuvres
- Lung bases (bibasal crepitations → pulmonary oedema; pleural effusion → heart failure)
- Abdomen (hepatomegaly, ascites, aortic pulsation)
- Legs (oedema, temperature, peripheral pulses)
- Completion: request BP lying/standing, 12-lead ECG, CXR, bedside echo
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 1904–1908; Goldman-Cecil Medicine, International Edition, p. 391
14 area where auscultation is proceed with idenfication of murmur
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching Images
cardiac auscultation areas precordium murmur locations diagram
Loading Image
Loading Image
Here is a comprehensive breakdown of the 14 areas of cardiac auscultation and the murmurs identified at each.
14 Areas of Cardiac Auscultation & Murmur Identification
The 14 Auscultatory Areas
Cardiac auscultation extends well beyond the classic 4 valve areas. The complete examination covers 14 zones across the precordium and beyond.
Zone Map (Anterior Chest)
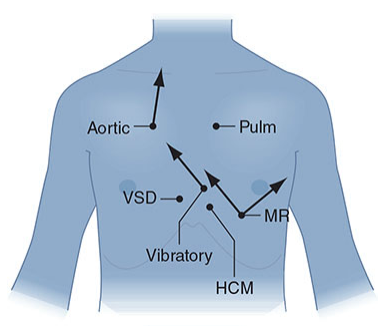
The 14 Areas: Location, Anatomy & Murmurs
| # | Area | Location | Valve/Structure | Key Murmurs Heard |
|---|---|---|---|---|
| 1 | Aortic area | 2nd right intercostal space (ICS), right sternal border | Aortic valve | AS (harsh ejection systolic, radiates to carotids); bicuspid aortic valve ejection click |
| 2 | Pulmonary area | 2nd left ICS, left sternal border | Pulmonary valve | PS (ejection systolic, click that softens on inspiration); PR (Graham Steell murmur — early diastolic in PAH) |
| 3 | Erb's point | 3rd left ICS, left sternal border | Aortic + pulmonary | AR best heard here (early diastolic, blowing, decrescendo — lean forward, hold expiration); also AS radiation |
| 4 | Tricuspid area | 4th–5th left ICS, lower left sternal border (LLSB) | Tricuspid valve | TR (holosystolic, increases with inspiration — Carvallo's sign); TS (mid-diastolic, increases with inspiration); VSD |
| 5 | Mitral area (Apex) | 5th left ICS, mid-clavicular line | Mitral valve | MR (holosystolic, blowing, radiates to axilla); MS (mid-diastolic rumble, low-pitched, best with bell in left lateral decubitus); S3, S4 gallops; MVP click |
| 6 | Left axilla | Mid-axillary line | — | Radiation of MR (posterior/anterior leaflet MR); differentiates MR from AS |
| 7 | Left infraclavicular area | Below left clavicle | Pulmonary artery | PDA murmur (continuous, machinery); radiation of PS |
| 8 | Right infraclavicular / right 1st ICS | Below right clavicle | Aorta | Aortic ejection click radiation; systemic arteriovenous fistula |
| 9 | Left sternal border (mid) | 3rd–4th left ICS | RVOT/LVOT | HOCM (crescendo-decrescendo, radiates to LLSB and apex, not to neck); differentiates from AS by manoeuvres |
| 10 | Right sternal border | Right 3rd–4th ICS | — | Dextrocardia murmurs; right-sided AS in dextrocardia; some aortic murmurs |
| 11 | Carotid arteries (neck) | Over carotid bifurcation | — | Radiation of AS; carotid bruits (arterial, systolic); distinguish from Gallavardin phenomenon (AS murmur at apex mimicking MR) |
| 12 | Back (interscapular) | Between scapulae, left > right | Aorta, coarctation | Coarctation of aorta (continuous murmur); PDA; collateral vessel bruits in coarctation |
| 13 | Epigastrium / xiphoid | Subxiphoid / epigastric | Tricuspid, RV | Tricuspid murmurs (TR/TS) in some patients; RVOT murmurs; aortic stenosis radiation in obese patients |
| 14 | Right 2nd ICS (sternal angle) | Upper right sternal border | Aortic root | Aortic stenosis (again, classical area); aortic sclerosis; aortic aneurysm flow murmur |
Many exam frameworks list 5 primary areas + accessory areas. The full 14-area system ensures no murmur is missed, particularly those with unusual radiation or right-sided pathology.
Murmur Timing Reference
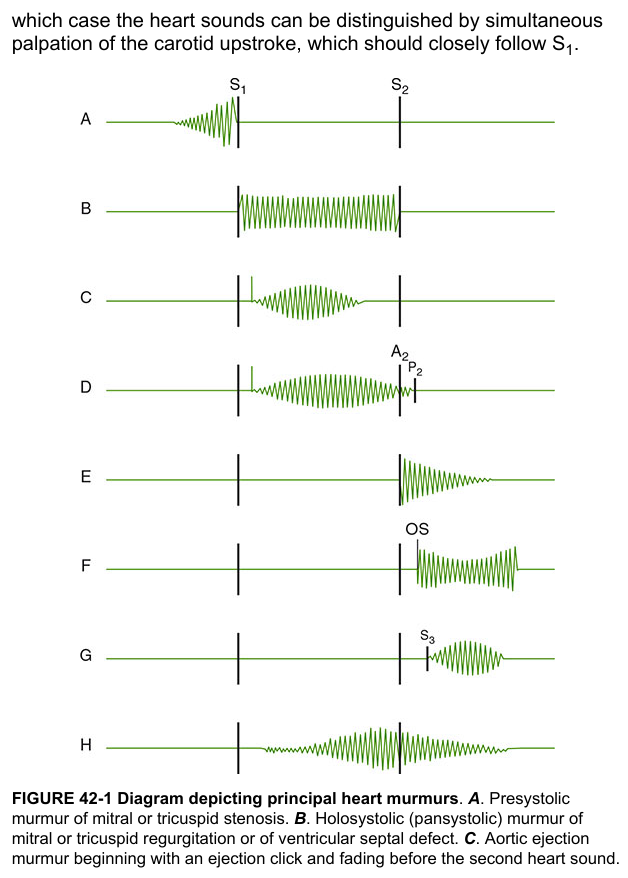
Murmur Identification by Timing
Systolic Murmurs
| Murmur | Timing | Quality | Location | Radiation | Manoeuvre |
|---|---|---|---|---|---|
| Aortic Stenosis (AS) | Mid-systolic (ejection) | Harsh, crescendo-decrescendo | 2nd RSB (Area 1) | Carotids (Area 11) | Louder squatting; softer Valsalva |
| Pulmonary Stenosis (PS) | Mid-systolic (ejection) | Soft-harsh | 2nd LSB (Area 2) | Left shoulder | Ejection click softens on inspiration |
| HOCM | Mid-systolic | Harsh | LLSB/apex (Area 9) | Apex, not carotids | Louder Valsalva/standing; softer squatting — key differentiator from AS |
| Mitral Regurgitation (MR) | Holosystolic | Blowing | Apex (Area 5) | Left axilla (Area 6) | — |
| Tricuspid Regurgitation (TR) | Holosystolic | Blowing | LLSB (Area 4) | — | Louder on inspiration (Carvallo's sign) |
| VSD | Holosystolic | Harsh | LLSB (Area 4) | — | — |
| MVP | Late systolic ± click | High-pitched | Apex (Area 5) | — | Click moves toward S1 on standing |
| Innocent/Still's murmur | Mid-systolic, vibratory | Musical, "twanging" | LLSB (Area 4) | — | Softer sitting/standing; no thrill |
| ASD | Mid-systolic | Soft | 2nd LSB (Area 2) | — | Fixed split S2 is the hallmark |
Diastolic Murmurs (always pathological)
| Murmur | Timing | Quality | Location | Radiation | Special Technique |
|---|---|---|---|---|---|
| Aortic Regurgitation (AR) | Early diastolic | Blowing, decrescendo | 3rd LSB / Erb's (Area 3) | — | Lean forward + hold expiration; Austin Flint murmur at apex |
| Pulmonary Regurgitation (PR) | Early diastolic | Blowing | 2nd LSB (Area 2) | — | Graham Steell murmur = PR in pulmonary hypertension |
| Mitral Stenosis (MS) | Mid-late diastolic (± presystolic accentuation) | Low-pitched rumble | Apex (Area 5) | — | Bell of stethoscope; left lateral decubitus; exercise |
| Tricuspid Stenosis (TS) | Mid-diastolic | Low-pitched | LLSB (Area 4) | — | Louder on inspiration; opening snap |
Continuous Murmurs
| Murmur | Location | Key Feature |
|---|---|---|
| PDA | Left infraclavicular / 2nd LSB (Area 7) | Machinery murmur, peaks at S2 |
| Coarctation of aorta | Back/interscapular (Area 12) | Also systolic murmur anteriorly; delayed femoral pulse |
| AV fistula / venous hum | Variable | Obliterated by compression |
Dynamic Manoeuvres Summary
| Manoeuvre | Preload | Afterload | Murmurs that increase |
|---|---|---|---|
| Valsalva (strain) | ↓↓ | ↓ | HOCM, MVP (click earlier) |
| Squatting | ↑↑ | ↑ | AS, MR, TR, VSD; HOCM softer, MVP click later |
| Standing | ↓ | — | HOCM, MVP |
| Inspiration | ↑ RV | — | TR, TS, PS, PR (all right-sided) |
| Handgrip | — | ↑↑ | MR, AR, VSD; HOCM softer |
| Amyl nitrite | ↑ | ↓↓ | AS, HOCM, TR, PS |
Grading of Murmur Intensity (Levine Scale)
| Grade | Description |
|---|---|
| 1/6 | Barely audible, requires concentration |
| 2/6 | Soft but readily heard |
| 3/6 | Moderately loud, no thrill |
| 4/6 | Loud + palpable thrill |
| 5/6 | Very loud, heard with stethoscope partially off chest |
| 6/6 | Heard without stethoscope |
Thrills are present at grade ≥ 4/6 and represent palpable turbulence.
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 1904–1912; Harrison's 21E, p. 1165–1168
This is a shared conversation. Sign in to Orris to start your own chat.