11 Injuries of the Thoracic Organs (Classification. Methods of examination of patients with chest and abdominal trauma. Clinical presentation and diagnosis. Modern treatment methods. Use of advanced technologies in the treatment of chest and abdominal injuries.)
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, rich content from multiple authoritative sources. Let me compile this into a complete, well-organized response.
Injuries of the Thoracic Organs
1. Classification
Thoracic injuries are broadly divided by mechanism and anatomical location:
By Mechanism
| Type | Description |
|---|---|
| Blunt | Deceleration (MVCs), falls, crush injuries, blast waves |
| Penetrating | Stab wounds (low-velocity), gunshot wounds (high-velocity) |
| Barotrauma/Blast | Explosion in air or water; high-energy shock waves |
By Anatomical Structure
- Chest wall injuries: Rib fractures, sternal fractures, flail chest
- Pleural space injuries: Pneumothorax (simple, tension, open, occult), hemothorax, hemopneumothorax
- Pulmonary injuries: Pulmonary contusion, laceration, traumatic pneumatocele
- Tracheobronchial injuries: Tracheal or bronchial disruption
- Cardiac injuries: Blunt cardiac injury (myocardial contusion), penetrating cardiac injury, cardiac tamponade
- Great vessel injuries: Blunt thoracic aortic injury (BTAI), subclavian vessel injury
- Esophageal injuries: Penetrating esophageal trauma
- Diaphragmatic injuries: Rupture from blunt or penetrating forces
Chest wall injuries are the most common thoracic injury — approximately 10% of all trauma admissions sustain at least one rib fracture; nearly 50% of multiply injured patients will have a rib fracture. Mortality in the multiply injured with chest wall injuries is 6–12%.
2. Methods of Examination
Primary Survey (ATLS Framework)
- Airway, Breathing, Circulation assessed immediately
- e-FAST (Extended Focused Assessment with Sonography in Trauma): rapid bedside ultrasound to detect hemothorax, pneumothorax, and pericardial tamponade; superior sensitivity for pneumothorax compared to plain chest radiograph
Imaging
Chest X-Ray (CXR)
- First-line; upright full-inspiratory film preferred
- Pneumothorax: peripheral lucency beyond lung markings
- Hemothorax: dependent opacification, blunting of costophrenic angle; ~200 mL required for detection on upright CXR, but as little as 5 mL detectable on decubitus film
- An air-fluid level indicates hemopneumothorax
- Detects only ~30% of rib fractures
CT Scan (Gold Standard)
- Highly sensitive for rib fractures, flail segments, occult pneumothorax, pulmonary contusion, aortic injury
- Occult pneumothorax: visible on CT but absent on CXR — diagnosed more frequently with increased CT use
- Contusion appears as higher-density tissue due to air-space hemorrhage and edema; typically worsens at 24–48 hours
- Differentiation tip: atelectasis does not cross pulmonary fissures; contusion does
Ultrasound (POCUS/e-FAST)
- Detects pneumothorax, hemothorax, pericardial effusion within the first minutes of arrival
- Loss of "lung sliding" sign = pneumothorax
- Critical in unstable polytrauma patients
Multi-Detector CT Angiography (MDCTA)
- Gold standard for evaluation of great vessel and aortic injury
- Standard catheter-based angiography (DSA) used if artifact-producing foreign bodies are present
Bronchoscopy / Esophagoscopy
- Bronchoscopy: evaluates trachea and proximal airways for injury
- Esophagoscopy + contrast esophagography: sensitivity approaches 100% when both are combined
ECG / Echocardiography
- For suspected blunt cardiac injury and pericardial tamponade
- Transesophageal echocardiography useful for thoracic aortic dissection
3. Clinical Presentation & Diagnosis of Specific Injuries
Rib Fractures
- Most common thoracic injury
- Ribs 4–9 most commonly fractured (structurally weakest at the posterior angle)
- Ribs 1–3: protected — fracture indicates severe force
- Ribs 9–11: associated with intra-abdominal injury (hepatic on right, splenic on left)
- Clinical findings: point tenderness, bony crepitus, ecchymosis, muscle spasm; barrel compression test (bimanual compression remote from injury site) reproduces pain at fracture site
- Risk stratification: 2+ rib fractures → higher incidence of internal injury; elderly patients (>65) with multiple rib fractures → higher pneumonia rates and mortality
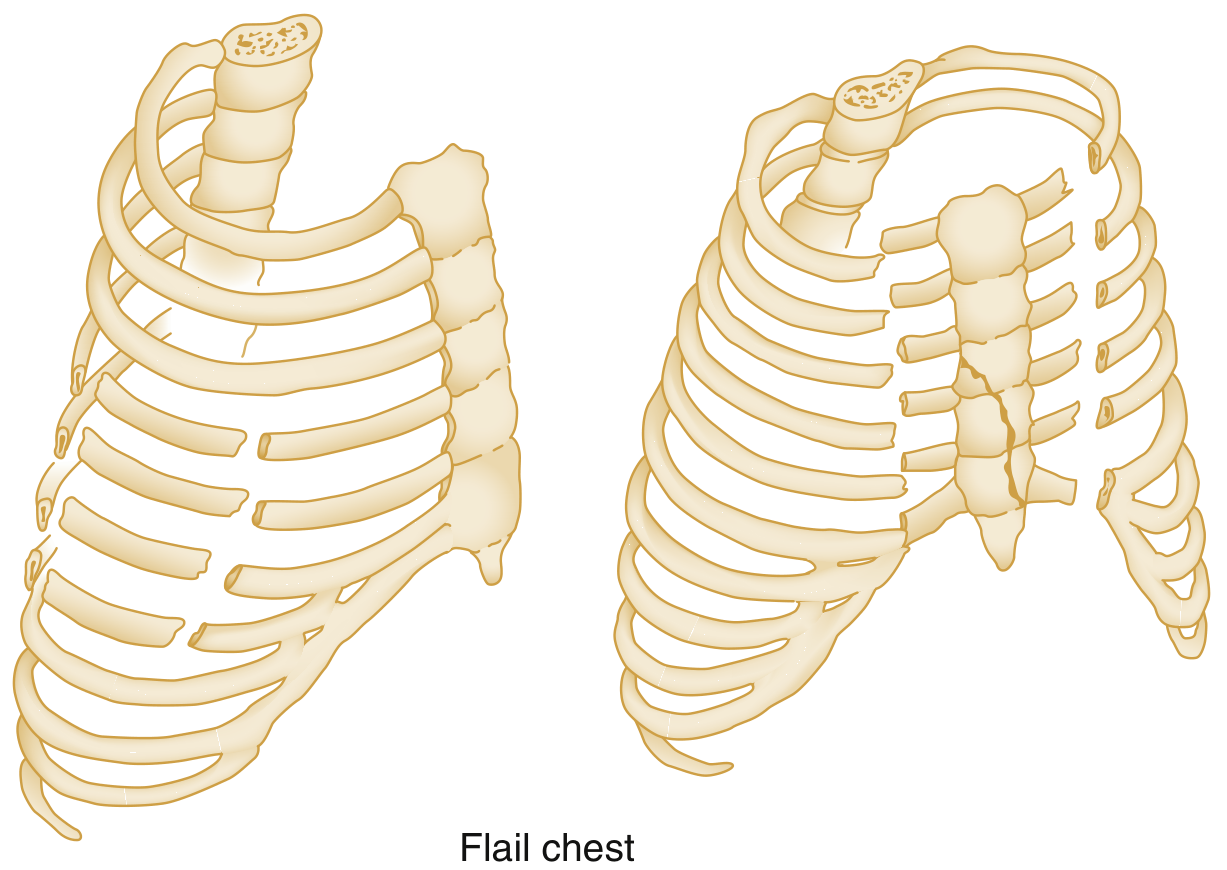
Flail Chest
- Defined as ≥3 adjacent ribs fractured at ≥2 points, creating a free segment
- Also occurs with costochondral separation or vertical sternal fracture + rib fractures
- Paradoxical motion: flail segment moves inward on inspiration, outward on expiration
- Paradoxical motion is obscured by positive-pressure ventilation
- Underlying pulmonary contusion is the major driver of respiratory insufficiency — not the mechanical instability alone
- Associated injuries: hemopneumothorax, liver/spleen lacerations, mediastinal injury
Pneumothorax
| Type | Features |
|---|---|
| Simple | Air in pleural space, no mediastinal shift |
| Tension | One-way valve: air enters but cannot exit; mediastinal shift, vena caval compression, reduced venous return, diminished cardiac output → life-threatening |
| Open ("sucking chest wound") | Communication between pleural space and atmosphere |
| Occult | Seen on CT, not on CXR |
Tension pneumothorax on CXR: complete ipsilateral lung collapse, ipsilateral hemidiaphragm depression/flattening, contralateral mediastinal shift.
Treatment:
- Clinical suspicion of tension PTX = immediate tube thoracostomy — do not delay for imaging
- Asymptomatic occult PTX (CT radial diameter ≤35 mm, no respiratory compromise) → observation + repeat CXR in 12–24 hours

Hemothorax
- CXR-visible hemothorax ≈ 400–500 mL → tube thoracostomy recommended
- Retained hemothorax increases morbidity (empyema, fibrothorax risk)
- Massive hemothorax: typically >1,500 mL initial output → thoracotomy consideration
Pulmonary Contusion
- Present in up to 75% of significant blunt chest trauma patients (most commonly MVCs with rapid deceleration)
- Also caused by high-velocity missiles and blast shock waves
- Pathophysiology: alveolar edema and hemorrhage without laceration → physiologic shunt → hypoxemia
- Clinical features: dyspnea, tachypnea, cyanosis, tachycardia, hypotension, chest wall bruising, hemoptysis, moist rales; may be absent on initial CXR but worsens at 24–48 hours
- Young patients (more elastic chest wall) may have severe contusions without rib fractures
- Complications: ARDS, pneumonia, respiratory failure

Cardiac Injuries
Penetrating Cardiac Injury
- Occurs in <1% of penetrating trauma overall; ~10% of penetrating chest trauma
-
90% of penetrating cardiac injuries are immediately lethal pre-hospital
- "Cardiac box": bounded by sternal notch (superior), costal margin (inferior), nipples bilaterally — high-risk zone
- Injury to right ventricle (most anterior structure) is most common
- Beck's Triad (tamponade): hypotension + muffled heart sounds + jugular venous distension
Blunt Cardiac Injury (Myocardial Contusion)
- Wide spectrum: asymptomatic ECG changes → free wall rupture
- Screen with ECG; echocardiography for structural assessment
Blunt Thoracic Aortic Injury (BTAI)
- One of the most common and deadly injuries in trauma patients
- Most commonly from high-speed deceleration
- Invasive aortography has been replaced by MDCTA, transesophageal echocardiography, and MRI
- CT is preferred in emergency settings due to speed and availability
Tracheobronchial Injuries
- Usually result from blunt deceleration or penetrating neck/chest trauma
- Suspect with massive air leak, persistent pneumothorax after tube thoracostomy, subcutaneous emphysema
- Diagnosed with bronchoscopy
Diaphragmatic Injuries
- Can occur from blunt or penetrating mechanisms
- Left side more commonly diagnosed (liver masks right-sided injuries)
- May present acutely with respiratory compromise or delayed with visceral herniation
4. Modern Treatment Methods
Chest Tube (Tube Thoracostomy)
Technique — "Triangle of Safety":
- Bordered by: nipple/inframammary fold (inferior), midaxillary line (posterior), lateral edge of pectoralis major (medial)
- Insertion at 4th–5th intercostal space, just above the rib (avoid neurovascular bundle inferiorly)
- Traditional size: 32–36 Fr; current evidence supports 14-Fr percutaneous catheters with equivalent success and lower morbidity for hemothorax drainage
- Connected to ~20 cmH₂O suction
Indications for Tube Thoracostomy:
- All pneumothoraces and hemothoraces visible on CXR
- Tension pneumothorax (clinical suspicion alone is sufficient)
- Hemodynamic instability with suspected pleural injury
Rib Fracture Management
- Single fracture, no complications: outpatient management with analgesia
- Multiple rib fractures / flail chest: multimodal analgesia (NSAIDS, opioids, nerve blocks — including epidural, paravertebral, or serratus anterior plane blocks), pulmonary hygiene, respiratory physiotherapy
- Surgical rib fixation (SSRF): indicated for flail chest with respiratory failure, displaced fractures with severe pain, chest wall deformity
Pulmonary Contusion Management
- Supportive: pulmonary hygiene, multimodal pain control, fluid restriction
- Monitor for respiratory decompensation: hypoxemia, increased work of breathing, agitation
- Mechanical ventilation (lung-protective strategy — low tidal volumes, permissive hypercapnia)
- ECMO for refractory respiratory failure; ELSO registry data shows 61% survival-to-discharge in trauma patients requiring ECMO cannulation
- Murray Lung Injury Score quantifies severity in mechanically ventilated patients and helps predict ECMO need
Indications for Emergency Thoracotomy
-
1,500 mL blood on initial chest tube insertion
- 200 mL/h drainage for ≥4 consecutive hours
- Persistent hemodynamic instability with ongoing transfusion requirement
- Massive air leak with persistent pneumothorax
- Drainage of esophageal or gastric contents from the chest tube (Note: these are traditional Vietnam War-era thresholds; clinical context and resuscitation response guide the decision more than absolute volumes)
Surgical Approaches for Thoracotomy
| Approach | Best Exposure |
|---|---|
| Left posterolateral thoracotomy (5th ICS) | Distal esophagus, left lung, left ventricle, descending aorta, left subclavian artery |
| Right posterolateral thoracotomy (5th ICS) | Proximal/mid-esophagus, trachea, bilateral mainstem bronchi |
| Median sternotomy | Right heart, ascending aorta, aortic arch, right arch vessels, pulmonary vasculature |
Penetrating Cardiac Injury
- Immediate pericardiocentesis or pericardial window for tamponade
- Operative repair of cardiac laceration
Damage Control Surgery in the Chest
- Thoracic packing with laparotomy sponges + temporary closure over chest tubes
- Unlike abdominal packing: chest packs must occupy minimal space to allow maximal lung expansion
5. Advanced Technologies in Thoracic Trauma
VATS (Video-Assisted Thoracoscopic Surgery)
- Increasingly used for retained hemothorax, empyema drainage, diaphragm repair, persistent air leaks
- Recent trials show: thoracic cavity irrigation immediately after tube insertion reduces retained hemothorax incidence and reduces need for VATS interventions
- Less morbidity than open thoracotomy
Endovascular / Interventional Radiology
- Endovascular stenting for BTAI: has largely replaced open aortic repair — significantly lower morbidity
- Embolization: for hemorrhage from pulmonary vasculature or intercostal vessels; less morbid alternative to surgery
ECMO (Extracorporeal Membrane Oxygenation)
- Used for refractory hypoxemia from severe pulmonary contusion / ARDS
- Allows lung-protective ventilation while maintaining oxygenation
- ELSO registry: 61% survival in trauma patients
Percutaneous/Minimally Invasive Techniques
- 14-Fr percutaneous chest catheters = equivalent efficacy to large-bore tubes for hemothorax drainage with reduced morbidity
- Ultrasound-guided insertion improves accuracy
Point-of-Care Ultrasound (POCUS / e-FAST)
- Detects pneumothorax, hemothorax, tamponade within minutes
- Integrated into the primary trauma survey
- Superior sensitivity for pneumothorax versus plain CXR
- Guides procedures in real-time (chest tube insertion, pericardiocentesis)
Surgical Lung-Sparing Techniques
- Stapled tractotomy: exposes injured vessels and bronchi for ligation without major resection
- Wedge resection: for peripheral lung injuries
- Lobectomy/pneumonectomy: reserved for massive destruction; trauma pneumonectomy carries >50% mortality
Summary of Key Decision Points
| Clinical Scenario | Action |
|---|---|
| Clinical tension PTX | Immediate tube thoracostomy — no imaging delay |
| Hemothorax visible on CXR | Tube thoracostomy |
| Occult PTX on CT, asymptomatic, ≤35 mm | Observation + repeat CXR in 12–24 h |
| Flail chest with respiratory failure | Intubation, lung-protective ventilation, consider SSRF |
| >1,500 mL initial chest tube output | Consider thoracotomy |
| Penetrating "cardiac box" injury | Immediate FAST, OR if effusion confirmed or hemodynamically unstable |
| BTAI | MDCTA → endovascular repair |
| Refractory ARDS from contusion | ECMO cannulation |
Sources: Sabiston Textbook of Surgery, 21e; Rosen's Emergency Medicine, 10e; Current Surgical Therapy, 14e; Murray & Nadel's Textbook of Respiratory Medicine; Mulholland and Greenfield's Surgery, 7e
This is a shared conversation. Sign in to Orris to start your own chat.