Why posterior relation of kidney is surgically important
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to give a thorough answer. Here is the full explanation:
Posterior Relations of the Kidney — Surgical Importance
Overview of Posterior Relations
The kidney lies retroperitoneally at the level of T12–L2/L3 vertebral bodies, with the upper pole more medial and posterior than the lower pole. Its posterior surface is in contact with several important structures that surgeons must navigate carefully.
From medial to lateral, the posterior relations are:
| Structure | Level | Relation |
|---|---|---|
| Diaphragm | Upper pole | Both kidneys, more on the left |
| Psoas major muscle | Medially | Both kidneys |
| Quadratus lumborum | Laterally | Both kidneys |
| Transversus abdominis (aponeurosis) | Lateral margin | Both kidneys |
| 12th rib | Upper pole | Both kidneys (left kidney also contacts 11th rib) |
| Subcostal nerve (T12) | Behind lower pole | Both kidneys |
| Iliohypogastric nerve (L1) | Behind lower pole | Both kidneys |
| Ilioinguinal nerve (L1) | Behind lower pole | Both kidneys |
Why Each Structure is Surgically Important
1. Diaphragm
- The upper pole of each kidney lies behind the diaphragm.
- During posterior or loin approach surgery (e.g., nephrectomy), the pleura may be inadvertently breached, causing a pneumothorax.
- Intercostal access above the 12th rib (required for upper-pole access in PCNL or partial nephrectomy) risks the posterior pleural reflection, which lies at the level of the 11th–12th rib.
- "Part of either kidney will lie above the eleventh/twelfth rib, especially the left kidney, and upper pole access may require an intercostal entry, placing the intercostal artery or pleura at risk." — Grainger & Allison's Diagnostic Radiology
2. 12th Rib (and 11th Rib for left kidney)
- The ribs form the posterosuperior boundary. The left kidney is in contact with both the 11th and 12th ribs; the right kidney only with the 12th.
- Surgical incisions (loin or posterior approach) are made along or below the 12th rib to access the kidney.
- A subcostal incision below the 12th rib avoids the pleura.
- Resection of the 12th rib gives wider access but requires careful pleural protection.
3. Subcostal Nerve (T12)
- Runs behind the kidney, just below the 12th rib.
- At risk of damage during posterior surgical approaches, causing denervation of the anterior abdominal wall muscles, leading to a visible bulge (pseudohernia) in the flank postoperatively.
- Must be identified and protected during loin incisions.
4. Iliohypogastric (L1) and Ilioinguinal (L1) Nerves
- These emerge from the lateral border of psoas major and course behind the lower pole.
- Injury during loin or flank dissection can cause sensory loss over the groin, scrotum/labia, and upper medial thigh, or contribute to post-surgical groin pain.
5. Psoas Major Muscle
- The medial part of the posterior surface of each kidney lies on the psoas muscle.
- When the kidney is adherent to psoas (e.g., due to fibrosis, perinephric infection), psoas fascia may be included in the dissection — this is a recognised manoeuvre in difficult nephrectomies.
- The psoas also guides the approach during retroperitoneoscopic surgery.
6. Quadratus Lumborum and Lumbodorsal (Thoracolumbar) Fascia
- The lateral posterior surface of the kidney rests on quadratus lumborum.
- The lumbodorsal fascia covers these posterior muscles and is a key anatomical layer in posterior/retroperitoneal surgical access.
- A lumbodorsal incision allows the kidney to be reached without incising muscle, reducing morbidity — a key advantage of the posterior retroperitoneal approach.
- The transversalis fascia fuses with the posterior lamina of Gerota's fascia medially, creating the boundary of the posterior pararenal space; this fascia must be incised to reach the renal hilum during retroperitoneal dissection.
Fascial Anatomy — Critical for Retroperitoneal Surgery
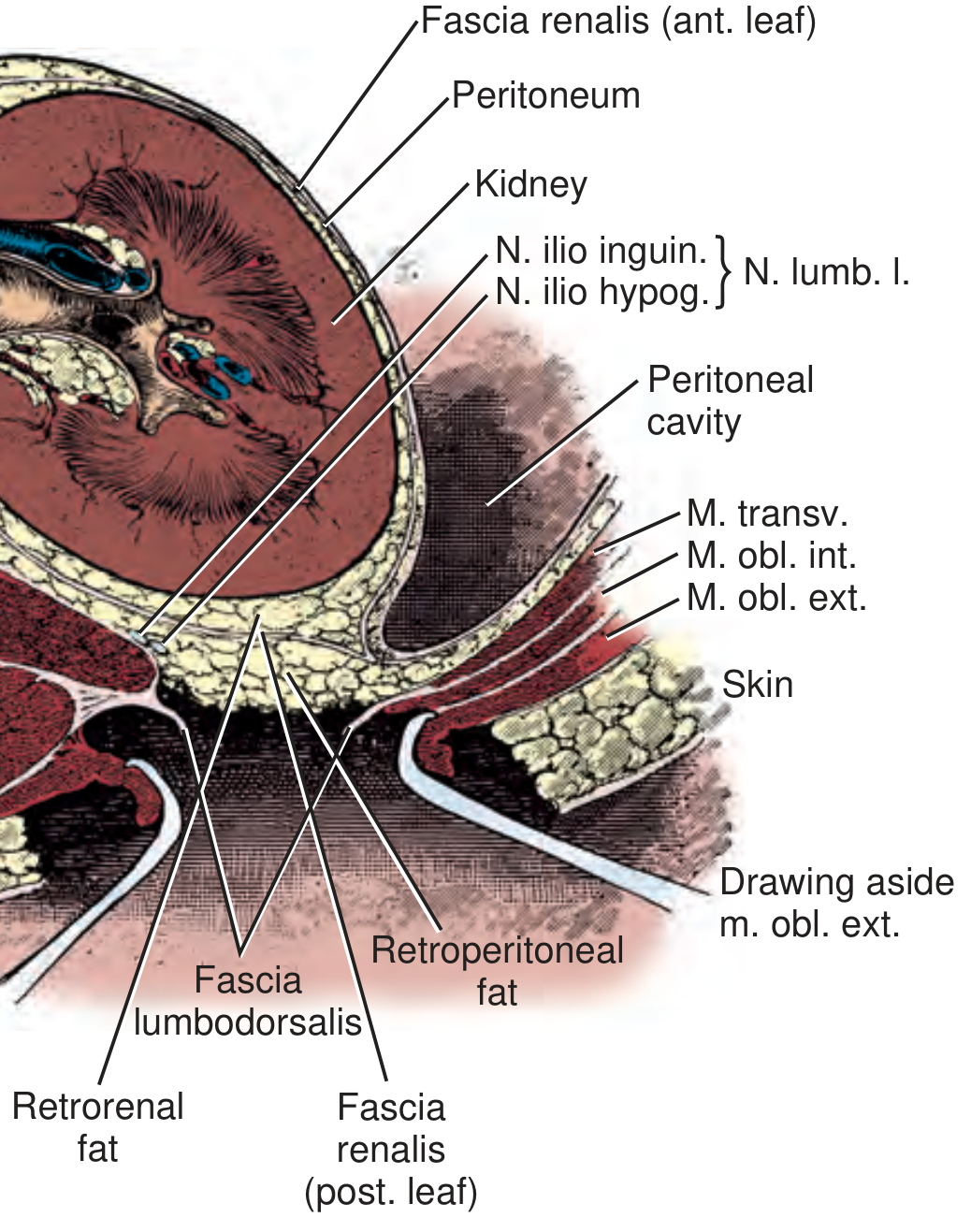
Transverse section through the kidney and posterior abdominal wall — showing fascial layers and posterior muscular relations. — Campbell-Walsh-Wein Urology
Gerota's fascia (renal fascia) has:
- An anterior lamina (fascia of Toldt) — thin, fuses with posterior peritoneum.
- A posterior lamina (fascia of Zückerkandl) — thicker, lies between the kidney and posterior abdominal wall.
These laminae enclose the perirenal space, which contains the kidney, adrenal, ureter, perinephric fat, and renal vessels. Surgeons must understand these layers to avoid entering the wrong space and to control bleeding.
Practical Surgical Summary
| Risk | Structure Involved | Consequence |
|---|---|---|
| Pleural tear | Diaphragm / 11th–12th rib | Pneumothorax, hydrothorax |
| Subcostal nerve damage | Subcostal nerve (T12) | Flank/abdominal wall bulge |
| Iliohypogastric/ilioinguinal nerve damage | L1 nerves | Groin/scrotal sensory loss |
| Bleeding from intercostal artery | Inferior rib groove | Haemothorax |
| Wrong fascial plane entry | Gerota's / transversalis fascia | Difficulty reaching hilum |
| Psoas adherence | Psoas major | Difficult plane, psoas fascia inclusion needed |
Sources:
- Campbell-Walsh-Wein Urology (Retroperitoneal anatomy chapter)
- Grainger & Allison's Diagnostic Radiology (Percutaneous renal access — anatomical factors)
This is a shared conversation. Sign in to Orris to start your own chat.