What is fever , classification of fever
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have all the material needed for a thorough answer.
Fever: Definition, Pathogenesis & Classification
Definition
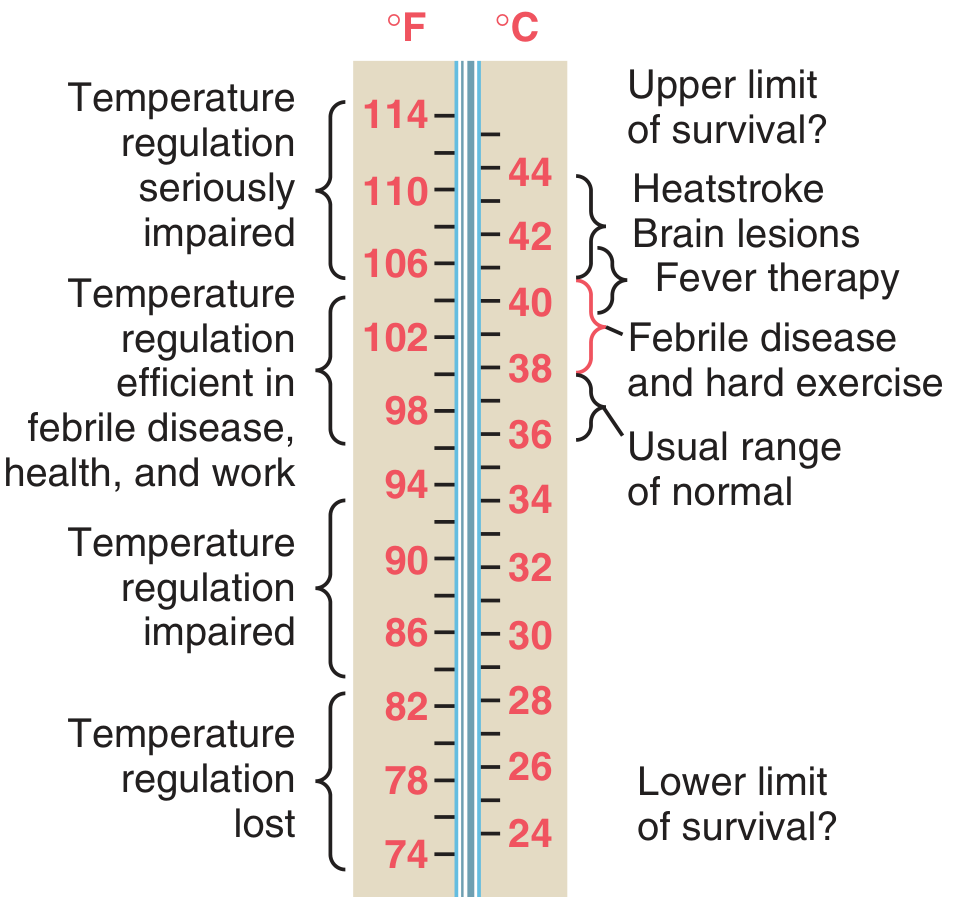
Fever is an abnormal elevation of body temperature above the usual range of normal, caused by a resetting of the hypothalamic thermostat to a higher set-point. It is distinct from hyperthermia, where body temperature rises without a change in the set-point.
- Normal body temperature: 36–37.5°C (96.8–99.5°F)
- Fever is generally defined as a core temperature > 38°C (100.4°F)
— Guyton and Hall Textbook of Medical Physiology, p. 900
Pathogenesis
1. Pyrogens
Substances that raise the hypothalamic set-point are called pyrogens. They are of two types:
| Type | Examples |
|---|---|
| Exogenous pyrogens | Bacterial lipopolysaccharide (LPS/endotoxin), viral particles, fungal antigens |
| Endogenous pyrogens | Cytokines released by leukocytes/macrophages (IL-1, IL-6, TNF-α, IFN-γ) |
2. Mechanism (Step-by-step)
- Bacteria/debris are phagocytized by macrophages, leukocytes, and killer lymphocytes
- These cells release interleukin-1 (IL-1) — also called leukocyte pyrogen / endogenous pyrogen
- IL-1 reaches the anterior hypothalamus and stimulates synthesis of prostaglandin E₂ (PGE₂)
- PGE₂ raises the hypothalamic set-point temperature
- The hypothalamus now perceives normal body temperature as "too low" → activates heat conservation (vasoconstriction, piloerection) and heat production (shivering)
- Body temperature rises to match the new set-point → fever
As little as one ten-millionth of a gram of LPS endotoxin, acting via leukocytes, can cause fever through nanogram amounts of IL-1. — Guyton and Hall, p. 900
Why Aspirin Reduces Fever
Aspirin inhibits cyclooxygenase (COX), blocking prostaglandin synthesis → set-point falls → hypothalamus triggers heat-dissipating mechanisms (vasodilation, sweating).
Body Temperature Ranges
Classification of Fever
A. By Temperature Grade
| Grade | Temperature | Examples |
|---|---|---|
| Low-grade (Subfever) | 37.5–38°C | Viral URTIs, early TB |
| Mild fever | 38–39°C | Many bacterial/viral infections |
| Moderate fever | 39–40°C | Pneumonia, UTI, malaria |
| High fever | 40–41°C | Typhoid, severe sepsis |
| Hyperpyrexia | > 41°C (>106°F) | CNS infections, malignant hyperthermia, heatstroke |
B. By Duration
| Type | Duration | Examples |
|---|---|---|
| Acute fever | < 2 weeks | Most common infections |
| Subacute fever | 2–6 weeks | Endocarditis, deep abscess |
| Chronic/Prolonged fever | > 6 weeks | Tuberculosis, malignancy, connective tissue disease |
| Fever of Unknown Origin (FUO) | > 3 weeks with no diagnosis after 1 week of investigation | ~30% infections, ~30% neoplasms, ~15% collagen-vascular disease |
C. By Fever Pattern (Pyrexia Patterns)
| Pattern | Description | Associated Conditions |
|---|---|---|
| Continuous (Sustained) | Temperature remains elevated with < 1°C diurnal variation; does not touch normal | Lobar pneumonia, typhoid, brucellosis, UTI |
| Remittent | Daily fluctuations > 1°C but temperature does not touch normal | Most febrile illnesses (infective endocarditis, typhoid in 2nd week) |
| Intermittent | Temperature returns to normal between spikes; exaggerated diurnal variation | Malaria (quotidian, tertian, quartan), pyogenic abscess, septicemia |
| Hectic (Septic) | Wide swings (>5°C) with sweating; marked peaks and deep troughs | Septicemia, pyemia, hepatic abscess |
| Relapsing (Undulant) | Periods of fever alternating with periods of normal temperature lasting days | Brucellosis, Borrelia (relapsing fever), Hodgkin lymphoma (Pel-Ebstein fever) |
| Pel-Ebstein fever | Regular, recurring cycles of fever and afebrile periods | Hodgkin lymphoma |
| Inverse (Reversed diurnal) | Higher in morning than evening | Miliary TB, liver abscess |
D. By Etiology
| Category | Examples |
|---|---|
| Infectious | Bacterial, viral, fungal, parasitic |
| Non-infectious inflammatory | Rheumatoid arthritis, SLE, vasculitis |
| Neoplastic | Lymphomas, renal cell carcinoma, hepatocellular carcinoma |
| Drug fever | Antibiotics (β-lactams), phenytoin, allopurinol |
| Neurogenic | Hypothalamic lesions, brain tumors, encephalitis |
| Factitious | Self-induced fever |
| Physiologic | Ovulation (slight rise), hard exercise |
Postoperative fever is classically remembered by the "Five Ws": Wind (atelectasis/pneumonia), Water (UTI), Wound (surgical site infection), Walking (DVT), Wonder drugs (drug fever). — Tintinalli's Emergency Medicine, p. 597
E. By Pathophysiology (Mediator Type)
| Type | Mechanism |
|---|---|
| Exogenous pyrogen-mediated | Direct LPS action on hypothalamus |
| Endogenous cytokine-mediated | IL-1, IL-6, TNF-α → PGE₂ |
| Neurogenic | Direct CNS lesions raising the set-point |
Fever vs. Hyperthermia
| Feature | Fever | Hyperthermia |
|---|---|---|
| Hypothalamic set-point | Elevated | Normal |
| Cause | Pyrogens/cytokines | Excessive heat gain or impaired dissipation |
| Response to antipyretics | Yes | No |
| Examples | Infections, malignancy | Heatstroke, malignant hyperthermia, NMS |
— Costanzo Physiology 7th Edition, p. 183–184
Key takeaway: Fever is a regulated, pyrogen-mediated upward shift of the hypothalamic set-point, primarily via IL-1 → PGE₂. It is classified by grade, duration, pattern, and etiology — each providing important diagnostic clues in clinical practice.
What is thermostat. Classification of fever according to Harrison, Davidson
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
I now have comprehensive content from Harrison's 22nd edition. Davidson's Principles & Practice of Medicine is not in the library, so I'll note that and provide the classification based on Harrison's (which is the standard reference for this topic) along with what Davidson's classifies fever patterns as (which I can provide from general medical knowledge, clearly labelled).
Hypothalamic Thermostat & Classification of Fever
Part 1 — The Hypothalamic Thermostat
What is the Thermostat?
The hypothalamic thermostat (thermoregulatory center) is the body's temperature-control mechanism, analogous to a home thermostat — it maintains core body temperature at a fixed set point (~37°C). It is located in the anterior hypothalamus, particularly around the organum vasculosum of the lamina terminalis (OVLT) — networks of enlarged capillaries surrounding the hypothalamic regulatory centers.
"This shift of the set point from 'normothermic' to febrile levels very much resembles the resetting of the home thermostat to a higher level in order to raise the ambient temperature in a room." — Harrison's Principles of Internal Medicine 22E, p. 178
Normal Set-Point: ~37°C (98.6°F)
The thermostat continuously balances:
- Heat production (metabolism, shivering, non-shivering thermogenesis in liver)
- Heat loss (vasodilation, sweating, radiation, respiration)
How the Thermostat is Reset in Fever
| Step | Event |
|---|---|
| 1 | Exogenous pyrogens (e.g., LPS endotoxin, microbial toxins) enter tissues |
| 2 | Myeloid & endothelial cells release pyrogenic cytokines: IL-1, IL-6, TNF, IFN-α |
| 3 | Cytokines interact with endothelium of hypothalamic capillaries (OVLT) |
| 4 | PGE₂ is synthesized locally in hypothalamic tissue (via COX enzyme) |
| 5 | PGE₂ raises the hypothalamic set point to a new, higher level |
| 6 | Hypothalamus now perceives normal body temperature as "too cold" |
| 7 | Activates vasoconstriction (hands/feet feel cold) + shivering → body temperature rises |
| 8 | Once blood temperature matches the new set point → fever is sustained |
| 9 | When pyrogens clear (or antipyretics given) → set point falls → vasodilation + sweating → defervescence |
— Harrison's Principles of Internal Medicine 22E, pp. 178–179
Pyrogens (Harrison's Classification)
Exogenous pyrogens — from outside the patient:
- Lipopolysaccharide (LPS/endotoxin) of gram-negative bacteria — most potent (2–3 ng/kg causes fever in humans)
- Cell-wall components of gram-positive bacteria
- Superantigens: S. aureus TSST-1, staphylococcal enterotoxins, streptococcal pyrogenic exotoxins (fever at 1–10 μg/kg)
Endogenous pyrogenic cytokines — from host cells:
- IL-1 (fever at 10–100 ng/kg)
- IL-6 (fever at 1–10 μg/kg — requires higher dose)
- TNF-α (fever at 10–100 ng/kg)
- Ciliary neurotropic factor (IL-6 family)
- IFN-α (fever as side effect of therapy)
Antipyretic Mechanism
NSAIDs/aspirin inhibit cyclooxygenase (COX) → block PGE₂ synthesis → set point falls → hypothalamus triggers sweating and vasodilation → temperature normalises.
Part 2 — Fever vs. Hyperthermia (Harrison's)
| Feature | Fever | Hyperthermia |
|---|---|---|
| Hypothalamic set point | Raised | Normal (unchanged) |
| Mechanism | Pyrogen → PGE₂ → set-point elevation | Excessive heat gain or failure of heat dissipation |
| Body's response | Purposeful (shivering, vasoconstriction to reach new set point) | Uncontrolled rise, body cannot dissipate heat |
| Response to antipyretics | Yes | No |
| Examples | Infections, autoimmune disease, malignancy | Heatstroke, malignant hyperthermia, NMS, serotonin syndrome |
"Hyperthermia is characterized by an uncontrolled increase in body temperature that exceeds the body's ability to lose heat. The setting of the hypothalamic thermoregulatory center is unchanged." — Harrison's 22E, p. 178
Hyperpyrexia: Fever > 41.5°C (> 106.7°F) — occurs in severe infections or, most commonly, in CNS hemorrhage. — Harrison's 22E, p. 178
Part 3 — Classification of Fever
A. Harrison's Classification (by Etiology / Disease Category)
Harrison's groups fever-presenting diseases into the following categories (Table 20-1, p. 179):
| Category | Examples |
|---|---|
| Infectious diseases | Bacterial, viral, fungal, parasitic |
| Autoimmune & non-infectious inflammatory disorders | SLE, RA, adult Still disease, pericarditis, gout |
| Cancer | Lymphomas (Hodgkin's), RCC, hepatoma |
| Medication-related | Vaccines, drug fever |
| Endocrine disorders | Hyperthyroidism, thyroid storm |
| Intrinsic hypothalamic malfunction | Hypothalamic tumour, trauma, hemorrhage |
B. Harrison's — Fever Patterns (by Periodicity)
Harrison's explicitly describes the following fever patterns (p. 179):
| Pattern | Description | Classic Association |
|---|---|---|
| Tertian fever | Fever every 3rd day | Plasmodium vivax malaria |
| Quartan fever | Fever every 4th day | Plasmodium malariae malaria |
| Relapsing fever | Days of fever → several afebrile days → relapse | Borrelia infection |
| Pel-Ebstein fever | Fever lasting 3–10 days followed by afebrile period of 3–10 days | Hodgkin lymphoma (classic); other lymphomas |
| Cyclic neutropenia fever | Fever every 21 days with neutropenia | Cyclic neutropenia |
| Periodic fever syndromes | Varying periodicity | Familial Mediterranean fever (FMF), TRAPS |
C. Davidson's Classification of Fever
(Davidson's Principles & Practice of Medicine is not in the current library, but its fever classification is well-established as follows:)
Davidson's classifies fever primarily by temperature pattern (pyrexia patterns):
| Pattern | Definition | Diseases |
|---|---|---|
| Continuous (Sustained) | Temp remains elevated; diurnal variation < 1°C; never touches normal | Lobar pneumonia, typhoid (1st week), UTI, gram-negative sepsis |
| Remittent | Daily fluctuations > 1°C but does not touch normal | Typhoid (2nd week), infective endocarditis, most bacterial fevers |
| Intermittent | Temp returns to normal between spikes (exaggerated diurnal variation) | Malaria, pyogenic abscess, septicemia |
| Hectic (Septic/Swinging) | Wide swings (>5°C); spiking peaks with profuse sweating; troughs near/at normal | Pyemia, empyema, septicemia, hepatic abscess |
| Undulant (Relapsing) | Waves of fever alternating with days of normal temperature | Brucellosis, Borrelia relapsing fever |
| Inverse (Reversed diurnal) | Higher in morning than evening (reverse of normal) | Miliary TB, hepatic abscess |
| Pel-Ebstein | Regular cycles of fever (3–10 days) and apyrexia | Hodgkin lymphoma |
Davidson's also classifies by duration:
- Acute — < 2 weeks
- Chronic — > 2 weeks (raises suspicion for TB, endocarditis, malignancy, connective tissue disease)
- Pyrexia of Unknown Origin (PUO) — fever > 38.3°C on multiple occasions, > 3 weeks duration, no diagnosis after 1 week of investigation
Key Takeaways
- The hypothalamic thermostat works exactly like a room thermostat — fever is simply its set point being deliberately raised by PGE₂
- Harrison's classifies fever by etiology (infection, malignancy, autoimmune, drug, endocrine, hypothalamic) and periodicity (tertian, quartan, Pel-Ebstein, relapsing)
- Davidson's emphasises fever patterns (continuous, remittent, intermittent, hectic, undulant, inverse) as clinical diagnostic tools
- Fever responds to antipyretics; true hyperthermia does not — a critical bedside distinction
Difference between sepsis and septic shock
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Harrison's 22E and Clinical Anesthesia. I have everything needed for a thorough answer.
Sepsis vs. Septic Shock
Historical Context & Evolution of Definitions
The definition of sepsis has evolved through three consensus conferences:
- Sepsis-1 (1992): Sepsis = suspected infection + ≥2 SIRS criteria; Septic shock = sepsis-induced hypotension (SBP < 90 mmHg) despite adequate fluids
- Sepsis-2 (2003): Expanded clinical/laboratory criteria
- Sepsis-3 (2016): Current standard — abandoned SIRS criteria entirely, replaced by organ dysfunction scoring
"Sir William Osler opined: 'except on few occasions, the patient appears to die from the body's response to infection rather than from it.'" — Harrison's Principles of Internal Medicine 22E, p. 2360
Current Definitions (Sepsis-3, 2016)
Sepsis
Life-threatening organ dysfunction caused by a dysregulated host response to infection Operationally defined as: acute increase in SOFA score ≥ 2 points due to infection — Barash Clinical Anesthesia 9E; Goldman-Cecil Medicine
Septic Shock
A subset of sepsis with underlying circulatory, cellular, and metabolic abnormalities so severe that the risk of death is substantially higher than sepsis alone Operationally defined as:
- Vasopressor requirement to maintain MAP ≥ 65 mmHg PLUS
- Serum lactate > 2 mmol/L (>18 mg/dL) despite adequate volume resuscitation — Goldman-Cecil Medicine, p. 1090; Barash Clinical Anesthesia 9E, p. 4829
Key Differences at a Glance
| Feature | Sepsis | Septic Shock |
|---|---|---|
| Definition | Dysregulated host response to infection + organ dysfunction | Sepsis + refractory circulatory failure |
| Diagnostic criterion | SOFA score ↑ ≥ 2 | Vasopressors needed for MAP ≥65 mmHg AND lactate > 2 mmol/L |
| Hypotension | May or may not be present | Present and refractory to fluid resuscitation |
| Lactate | May be elevated | > 2 mmol/L despite adequate resuscitation |
| Vasopressor need | Not required | Required (norepinephrine, vasopressin, etc.) |
| Organ dysfunction | Present (SOFA ≥ 2) | Present + cardiovascular collapse |
| Mortality | ~10–26% | 40–60% (substantially higher) |
| Severity | Severe | Most severe (end of spectrum) |
SOFA Score (Sequential Organ Failure Assessment)
Used to diagnose sepsis — a ≥2-point acute rise indicates organ dysfunction:
| System | Parameter | Scoring 0→4 (worse) |
|---|---|---|
| Respiratory | PaO₂/FiO₂ | ≥400 → <100 |
| Coagulation | Platelets ×10³/μL | ≥150 → <20 |
| Liver | Bilirubin mg/dL | <1.2 → >12 |
| Cardiovascular | MAP / vasopressors | MAP ≥70 → Dopamine >15 or Epi >0.1 μg/kg/min |
| CNS | Glasgow Coma Scale | 15 → <6 |
| Renal | Creatinine / urine output | <1.2 → >5 mg/dL or UO <200 mL/d |
Quick SOFA (qSOFA) — bedside screening tool (1 point each):
- Respiratory rate ≥ 22/min
- Altered mental status (GCS < 15)
- Systolic BP ≤ 100 mmHg
Score ≥ 2 = suspect sepsis, escalate evaluation.
— Goldman-Cecil Medicine, p. 1090
Pathophysiology
Common to Both — Dysregulated Host Immune Response
- PAMPs (Pathogen-Associated Molecular Patterns — e.g., LPS from gram-negative bacteria, cell-wall components of gram-positives) and DAMPs (Damage-Associated Molecular Patterns — histones, HMGB1, ATP) are released
- Recognised by Pattern Recognition Receptors (PRRs): Toll-like receptors (TLRs), NOD receptors, RAGE, RIG-I
- Triggers massive release of pro-inflammatory cytokines (IL-1, IL-6, TNF-α) and chemokines
- Neutrophils activate → form NETs (Neutrophil Extracellular Traps) → microvascular thromboses
- Endothelial dysfunction → capillary leak → oedema, hypotension
— Harrison's 22E, p. 2361
What Distinguishes Septic Shock
In septic shock, the above cascade leads to:
| Mechanism | Consequence |
|---|---|
| Massive vasodilation (↓ SVR) | Refractory hypotension |
| Myocardial depression (↓ LVEF) | ↓ Cardiac output despite hyperdynamic state early on |
| Relative hypovolaemia | Tissue hypoperfusion |
| Impaired cellular O₂ extraction | Lactic acidosis even with normal O₂ delivery |
| Maldistribution of blood flow | Multi-organ dysfunction |
"Even in the case of normal or seemingly adequate CO and oxygen delivery, metabolic needs are increased during sepsis, and the ability of the tissues to extract and utilise oxygen may be impaired. Thus, metabolic acidosis may be present despite normal levels of oxygen transport." — Barash Clinical Anesthesia 9E, p. 4829
Organ Complications (Harrison's, p. 2365)
| Organ | Frequency | Key Finding |
|---|---|---|
| Kidney (AKI) | 67% of septic patients | Oliguria, ↑ creatinine |
| Neurological (encephalopathy) | 54% | Delirium → coma |
| Cardiovascular (shock) | 25% develop shock; 50% have myocardial dysfunction | Tachycardia, hypotension, mottling |
| Respiratory (ARDS) | 7% | Bilateral infiltrates, ↓ PaO₂/FiO₂ |
Management Principles (Surviving Sepsis Campaign)
| Intervention | Sepsis | Septic Shock |
|---|---|---|
| Blood cultures before antibiotics | ✓ | ✓ |
| Broad-spectrum antibiotics within 1 hour | ✓ | ✓ (urgent) |
| IV fluid resuscitation (balanced crystalloid 30 mL/kg) | ✓ | ✓ |
| Vasopressors (norepinephrine 1st, vasopressin 2nd, epinephrine 3rd) | Only if hypotension persists | Required |
| Hydrocortisone 200 mg/day | Not routine | If ongoing vasopressor requirement |
| Dobutamine / Epinephrine | Consider in ↓ LVEF | Consider in mixed septic-cardiogenic shock |
| Source control | ✓ | ✓ |
— Barash Clinical Anesthesia 9E, p. 4830; Harrison's 22E, p. 2365
Summary Spectrum
Infection
↓
Sepsis (infection + SOFA ↑≥2)
↓
Septic Shock (sepsis + vasopressor needed + lactate >2 mmol/L)
↓
Multi-Organ Dysfunction Syndrome (MODS) → Death
The core distinction: Sepsis is organ dysfunction from dysregulated host response; septic shock is sepsis with circulatory and metabolic failure so severe that vasopressors are required and tissue hypoperfusion (elevated lactate) persists despite resuscitation — carrying a mortality of 40–60%.
This is a shared conversation. Sign in to Orris to start your own chat.