hypertension for bds 2nd year pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive BDS 2nd year pathology answer on hypertension. Let me compile the full response.
Hypertension - Pathology (BDS 2nd Year)
Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
Definition
Hypertension is a sustained elevation of blood pressure. By current criteria, diastolic pressure >80 mm Hg or systolic pressure >120 mm Hg constitutes hypertension. About 40-50% of adults in the general population are affected.
Classification / Types
| Type | Frequency | Details |
|---|---|---|
| Primary (Essential) Hypertension | 90-95% of cases | No identifiable single cause; multifactorial |
| Secondary Hypertension | 5-10% | Due to identifiable cause |
Causes of Secondary Hypertension
Renal:
- Acute glomerulonephritis
- Chronic renal disease
- Polycystic kidney disease
- Renal artery stenosis
- Renin-producing tumors
Endocrine:
- Cushing syndrome, primary aldosteronism, congenital adrenal hyperplasia
- Pheochromocytoma
- Acromegaly
- Hypothyroidism (myxedema) / Hyperthyroidism
- Pregnancy-induced (preeclampsia)
- Exogenous hormones (glucocorticoids, oral contraceptives)
Cardiovascular:
- Coarctation of the aorta
- Polyarteritis nodosa
Neurologic:
- Increased intracranial pressure
- Obstructive sleep apnea
(Robbins & Kumar Basic Pathology, Table 8.1)
Blood Pressure Regulation (Normal Physiology)
Blood pressure = Cardiac output × Peripheral vascular resistance
- Cardiac output is determined by heart rate + stroke volume (which depends on blood volume)
- Vascular resistance is regulated at the arteriolar level via neural and hormonal inputs
- Kidney is the key regulator through sodium excretion and the RAAS (Renin-Angiotensin-Aldosterone System)
RAAS Pathway:
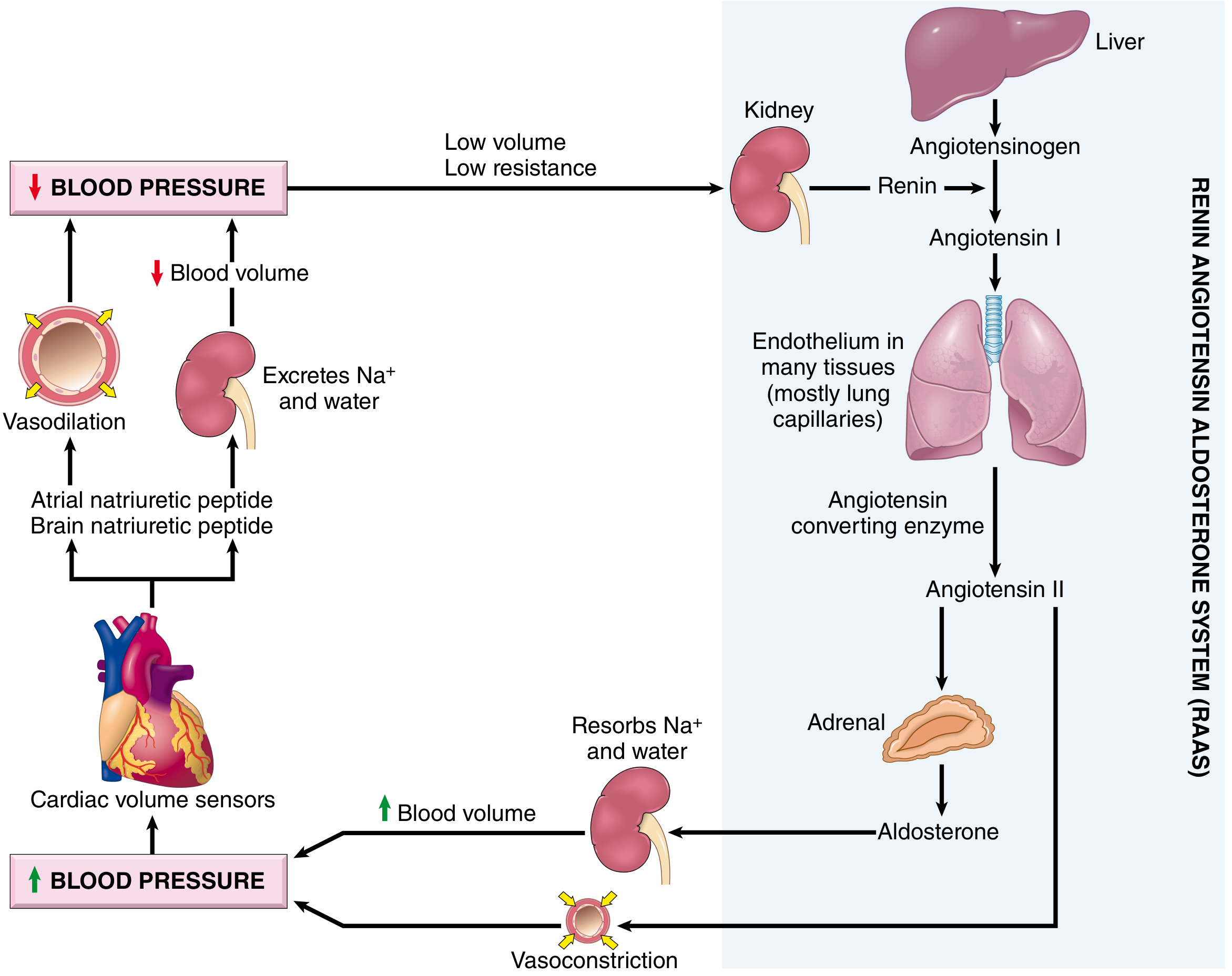
Fig: The Renin-Angiotensin-Aldosterone System and its role in blood pressure homeostasis - Robbins, Cotran & Kumar Pathologic Basis of Disease, Fig. 11.4
Pathogenesis of Primary (Essential) Hypertension
Primary hypertension results from complex interplay of genetic and environmental factors that increase blood volume and/or peripheral resistance.
Two Key Mechanisms:
1. Reduced renal sodium excretion:
- Reduced Na+ excretion at normal arterial pressure is a key initiating event
- This causes obligatory fluid volume expansion → ↑ cardiac output → ↑ BP
- The kidney then excretes Na+ at the new higher pressure ("resetting of pressure natriuresis")
- A new steady state is achieved but at the expense of elevated BP
2. Increased vascular resistance:
- May result from vasoconstriction or structural thickening of vessel walls
- Chronic vasoconstriction can cause permanent wall thickening
Genetic Factors:
- Familial clustering and twin studies confirm genetic role
- Susceptibility genes influence renal sodium resorption, endogenous pressor production, and smooth muscle cell (SMC) growth
- Angiotensinogen polymorphisms and angiotensin II receptor variants are implicated in some cases
- Single-gene disorders causing rare forms: gene defects in aldosterone metabolism (aldosterone synthase, 11β-hydroxylase, 17α-hydroxylase) → increased aldosterone secretion
- Liddle syndrome: mutations in epithelial Na+ channel (ENaC-γ) → exaggerated distal tubular Na+ reabsorption
Environmental Factors:
- Stress, obesity, smoking, physical inactivity
- High dietary sodium intake - strongest environmental link
- Lack of access to healthcare
(Robbins & Kumar Basic Pathology, p. 311)
Morphology (Pathological Changes)
Hypertension causes two main forms of arteriolosclerosis (small vessel disease):
1. Hyaline Arteriolosclerosis
- Associated with benign/primary hypertension
- Gross/Histology: Thickening of arteriolar walls with deposition of homogeneous, pink hyaline material; loss of underlying structural detail; luminal narrowing
- Mechanism: Plasma protein leakage across injured endothelial cells (ECs) into vessel walls + increased extracellular matrix (ECM) production by SMCs in response to chronic hemodynamic stress
- Important: Also seen in normotensive elderly individuals and in diabetic microangiopathy (due to hyperglycemia-associated EC dysfunction), but more generalized and severe in hypertension
- Kidney effect: Arteriolar narrowing → nephrosclerosis (glomerular scarring)
2. Hyperplastic Arteriolosclerosis ("Onion-Skinning")
- Typical of severe/malignant hypertension
- Histology: Concentric, laminated thickening of arteriolar walls with luminal narrowing - resembles concentric rings of an onion
- The laminations consist of SMCs with thickened, reduplicated basement membrane
- In malignant hypertension: accompanied by fibrinoid necrosis (especially prominent in kidneys) - called necrotizing arteriolitis
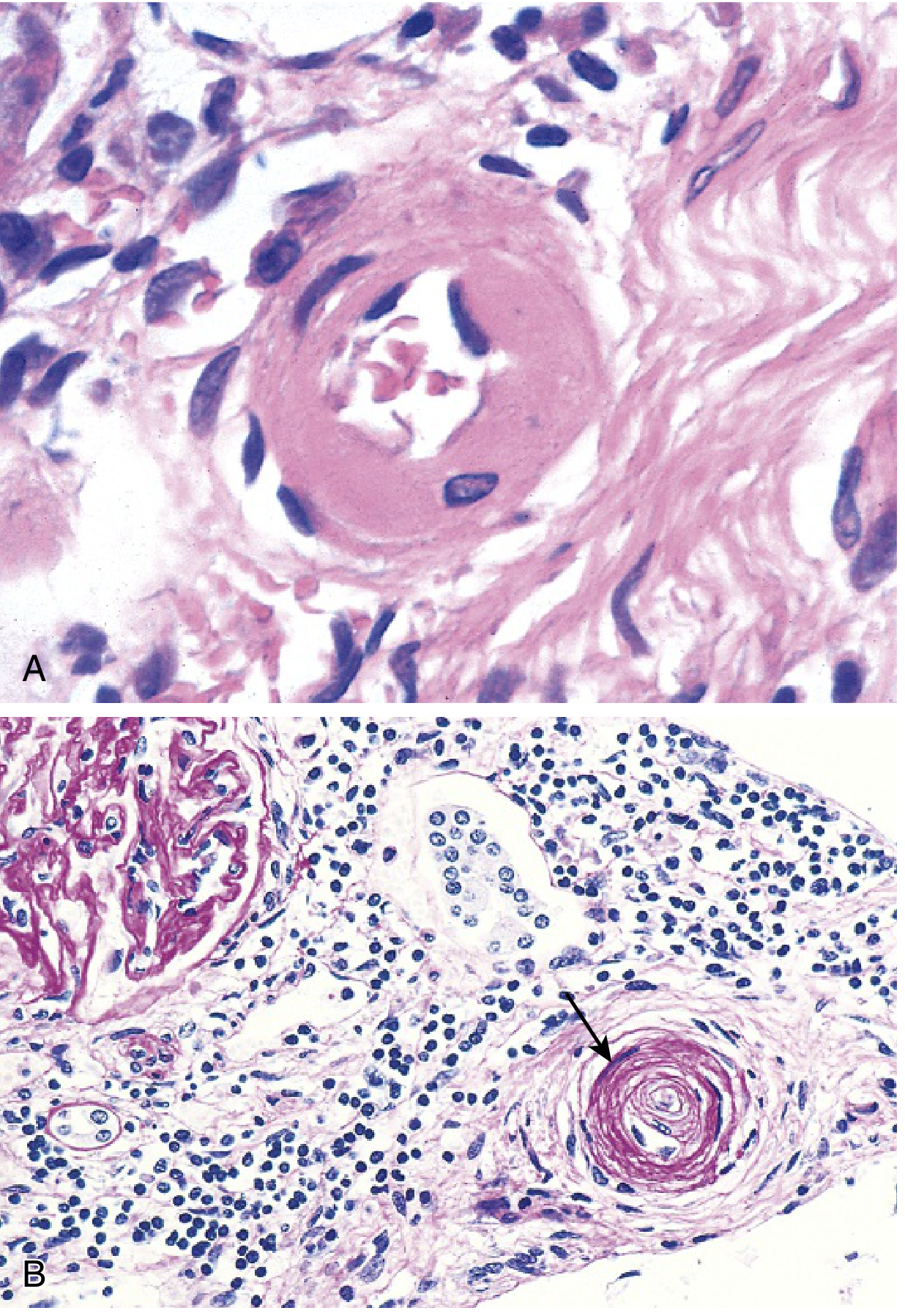
Fig 8.4: (A) Hyaline arteriolosclerosis - pink homogeneous wall thickening, narrow lumen. (B) Hyperplastic arteriolosclerosis - onion-skin concentric laminations, obliterated lumen (PAS stain) - Robbins & Kumar Basic Pathology
Malignant Hypertension
- Approximately 5% of hypertensive patients
- Systolic >180 mm Hg or diastolic >120 mm Hg
- If untreated: death within 1-2 years
- Associated with: renal failure, retinal hemorrhages, papilledema
- May arise de novo or be superimposed on pre-existing hypertension
- Morphologically: hyperplastic arteriolosclerosis + fibrinoid necrosis
Consequences / Complications of Hypertension
Hypertension is a major risk factor for:
| Organ | Consequence |
|---|---|
| Heart | Ischemic heart disease (IHD), congestive heart failure (most common cause of death - ~50%) |
| Brain | Stroke (cerebrovascular hemorrhage) - accounts for ~1/3 of deaths |
| Kidney | Nephrosclerosis (glomerular scarring due to arteriolar narrowing), renal failure |
| Eyes | Retinal hemorrhages, papilledema (in malignant HTN) |
| Aorta | Aortic dissection |
| Vessels | Accelerates atherosclerosis in large and medium arteries |
(Robbins & Kumar Basic Pathology, p. 310-312)
Summary Table: Hyaline vs. Hyperplastic Arteriolosclerosis
| Feature | Hyaline Arteriolosclerosis | Hyperplastic Arteriolosclerosis |
|---|---|---|
| Associated with | Benign/mild hypertension, diabetes, old age | Severe/malignant hypertension |
| Histology | Homogeneous pink hyaline material | Concentric laminated "onion skin" |
| Composition | Plasma proteins + SMC-derived ECM | SMCs + reduplicated basement membrane |
| Lumen | Narrowed | Markedly narrowed/obliterated |
| Additional lesion in malignant HTN | - | Fibrinoid necrosis (necrotizing arteriolitis) |
Key Concepts Summary (Robbins Key Concepts)
- Hypertension affects roughly half of adults; major risk factor for atherosclerosis, congestive heart failure, and renal failure
- Essential hypertension (90-95%) is multifactorial - involves environmental influences + genetic variants affecting sodium resorption, aldosterone, and the RAAS
- Secondary hypertension - caused by single-gene disorders or diseases of kidney, adrenal, or other endocrine organs
- Sustained hypertension = increased blood volume + increased peripheral resistance, both from increased renal sodium resorption
- Histologically: hyaline arteriolosclerosis (mild HTN) and hyperplastic arteriolosclerosis (severe HTN)
Sources: Robbins & Kumar Basic Pathology (9780323790185), pp. 310-312 | Robbins, Cotran & Kumar Pathologic Basis of Disease (9780443264528), pp. 463-465
This is a shared conversation. Sign in to Orris to start your own chat.