Chronic diseases of the larynx. Foreign bodies of larynx, trachea, bronchi. esophagus. Intubation and Tracheostomy. Explain in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
tracheostomy procedure surgical anatomy
Searching Images
foreign body aspiration bronchoscopy airway
Searching Images
chronic laryngitis vocal cord nodule polyp laryngeal pathology
Searching Images
esophageal foreign body impaction X-ray endoscopy
I now have comprehensive material from multiple authoritative sources. Let me compose a detailed, well-structured response.
Chronic Diseases of the Larynx · Foreign Bodies of the Airway & Esophagus · Intubation & Tracheostomy
PART 1 — CHRONIC DISEASES OF THE LARYNX
1.1 Chronic Laryngitis
Definition: Persistent mucosal inflammation of the larynx lasting > 3 weeks.
Causes:
- Chronic voice abuse / vocal overuse (teachers, singers)
- Tobacco smoking and alcohol
- Laryngopharyngeal reflux (LPR) — the most common cause today
- Chronic sinusitis with postnasal drip
- Occupational exposure (dust, chemical fumes)
- Mouth breathing
Pathology: Squamous metaplasia of the respiratory epithelium, submucosal fibrosis, glandular atrophy. Reinke's edema (diffuse polypoid degeneration of the superficial lamina propria) develops with chronic smoking + voice abuse.
Clinical Features:
- Persistent hoarseness (dysphonia) — cardinal symptom
- Dry irritating cough
- Throat-clearing
- Globus sensation
- Vocal fatigue
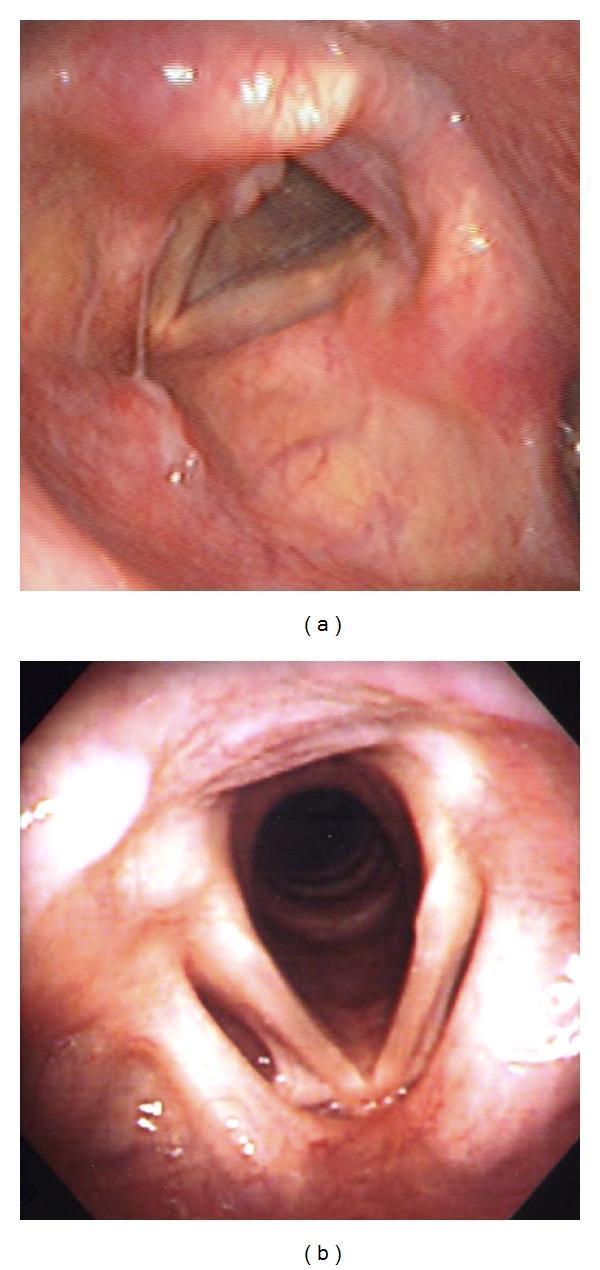
Laryngoscopy Findings:
- Diffuse mucosal erythema and edema
- Thickening of the vocal folds
- Interarytenoid congestion
- Posterior commissure hypertrophy (sign of LPR)
Management:
- Remove causative factors (stop smoking, voice rest)
- Proton pump inhibitors (PPIs) for LPR
- Voice therapy
- Steam inhalations, mucolytics
- Microlaryngoscopy + stripping for Reinke's edema if severe
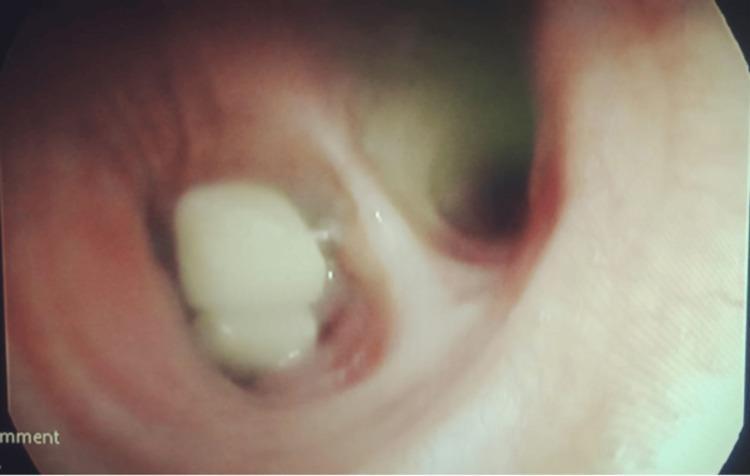
1.2 Vocal Fold Nodules ("Singer's Nodes")
Bilateral, symmetrical fibrous thickenings at the junction of the anterior 1/3 and posterior 2/3 of each vocal fold — the point of maximal vibration stress.
Cause: Chronic vocal abuse; most common in women and children.
Laryngoscopy: White, sessile, smooth nodules bilaterally, preventing complete glottic closure → air-waste hoarseness.
Management: Voice therapy first; microlaryngoscopic excision if persistent (3–6 months).
1.3 Vocal Fold Polyps
Unilateral, pedunculated or sessile lesions; may be haemorrhagic or myxoid.
Cause: Single episode of vocal strain, LPR, smoking.
Treatment: Microlaryngoscopic excision.
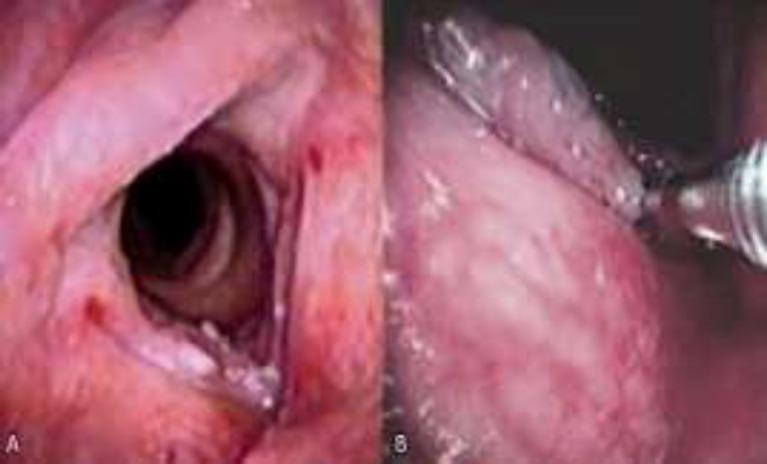
1.4 Laryngeal Leukoplakia & Keratosis
White patches on the vocal folds due to squamous hyperkeratosis.
- Risk of malignant transformation: 5–10%
- Mandatory biopsy to exclude dysplasia or carcinoma-in-situ.
- Management: cessation of smoking, microlaryngoscopic stripping, laser excision; close endoscopic surveillance.
1.5 Laryngeal Tuberculosis
Historically the most feared laryngeal disease; now rare in developed countries.
- Source: Almost always secondary to pulmonary TB via infected sputum.
- Sites: Posterior larynx (arytenoids, interarytenoid fold) > anterior larynx; contrast with syphilis which starts anteriorly.
- Symptoms: Hoarseness, odynophagia (severe, "can't swallow own saliva"), systemic TB symptoms.
- Laryngoscopy: Pale oedematous mucosa, "turban epiglottis," superficial ulceration, later scarring.
- Diagnosis: Laryngeal biopsy + AFB smear/culture; chest X-ray.
- Treatment: Standard anti-TB regimen (RHEZ for 2 months, then RH for 4 months).
1.6 Laryngeal Syphilis
Tertiary syphilis: gummatous lesions anteriorly → perichondritis → cartilage destruction → severe scarring and stenosis.
Diagnosis: serology (VDRL, TPHA); biopsy.
Treatment: Penicillin G.
1.7 Scleroma (Rhinoscleroma of the Larynx)
Caused by Klebsiella rhinoscleromatis; granulomatous infection starting in the nose, may involve the larynx causing hoarseness and subglottic stenosis.
Histology: Mikulicz cells (vacuolated macrophages containing organisms) + Russell bodies.
Treatment: Long-term tetracycline or ciprofloxacin; surgical dilation of stenosis.
1.8 Laryngeal Cancer
- The most important chronic laryngeal disease; squamous cell carcinoma (SCC) accounts for >95%.
- Risk factors: Tobacco (primary), alcohol (synergistic), HPV-16/18.
- Classification: Glottic (most common, best prognosis), supraglottic, subglottic.
- Symptoms: Progressive hoarseness (early in glottic tumours), dysphagia, dyspnoea, neck mass (nodal metastasis).
- Diagnosis: Laryngoscopy + biopsy; CT/MRI for staging.
- Treatment: Early disease — radiotherapy or endoscopic laser resection (voice-preserving). Advanced disease — total laryngectomy ± neck dissection ± chemoradiotherapy. Proximal risk factors include tobacco and alcohol. — Goldman-Cecil Medicine
PART 2 — FOREIGN BODIES OF THE LARYNX, TRACHEA & BRONCHI
2.1 Epidemiology & Types
- Most common in children < 5 years (peanuts, seeds, small toys) and elderly (poorly fitting dentures, meat bolus).
- Adults: unusual; consider in anyone presenting with sudden onset cough, wheeze, or stridor.
- Most common object in adults and children: organic (peanuts, sunflower seeds, beans); these swell with time and are more hazardous.
2.2 Anatomy of Lodgement
| Site | Reason |
|---|---|
| Larynx (subglottis) | Narrowest point in the paediatric airway |
| Right main bronchus | More vertical, wider calibre; foreign bodies go here preferentially |
| Trachea | Objects that pass the larynx but are too large for a bronchus |
2.3 Clinical Features
Three stages (classic):
- Initial (violent) stage — Sudden paroxysmal coughing, choking, gagging, stridor, cyanosis at the moment of aspiration. May be witnessed.
- Asymptomatic (latent) stage — Object lodges, symptoms quiet down. This stage can last hours to weeks. Dangerous: the problem may be forgotten.
- Symptomatic (complication) stage — Inflammation, infection, granulation tissue formation → recurrent pneumonia, atelectasis, bronchiectasis, abscess.
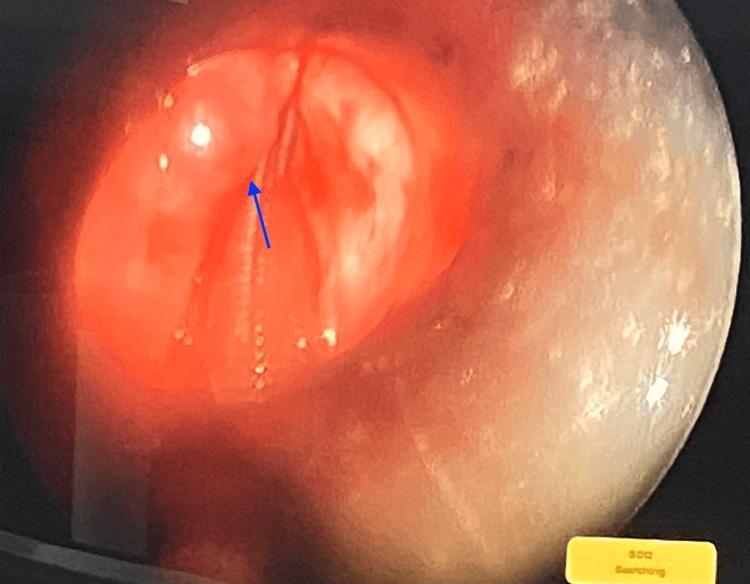
Laryngeal FB: Stridor, dysphonia or aphonia, severe respiratory distress, cyanosis — life-threatening emergency.
Tracheal FB: Audible "slap" on coughing (pathognomonic), bilateral wheezing, "asthmatoid wheeze."
Bronchial FB (most common site): Unilateral wheeze, persistent cough, recurrent pneumonia in the same lobe, atelectasis, obstructive emphysema (air-trapping on expiratory film).
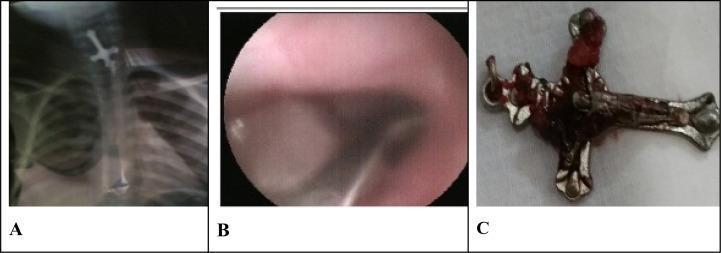
2.4 Radiology
- Plain X-ray (AP + lateral, including neck and chest):
- Radiopaque FBs (coins, metals) are directly visible.
- Most organic FBs are radiolucent — look for indirect signs: unilateral hyperlucency (obstructive emphysema), mediastinal shift away from the affected side on expiration, atelectasis, lobar consolidation.
- Expiratory film or fluoroscopy is essential — demonstrates air-trapping on the affected side (mediastinum shifts to the opposite side on expiration = positive finding).
- CT chest: Best for near-soft-tissue-density FBs; defines location precisely.
- Radiographs may be completely normal — a high index of suspicion is paramount. — Murray & Nadel's Textbook of Respiratory Medicine
2.5 Management
Immediate (pre-hospital):
- Conscious child: Heimlich manoeuvre (> 1 year) or back blows + chest thrusts (< 1 year).
- Unconscious: CPR protocol; finger-sweep only if FB is visible.
Definitive — Rigid Bronchoscopy (gold standard):
- Performed under general anaesthesia.
- Allows suction, forceps extraction, and ventilation simultaneously.
- Success rate: ~90% for flexible bronchoscopy, higher for rigid. — Murray & Nadel
Flexible Bronchoscopy:
- Preferred in adults, ICU patients on ventilators.
- Use retrieval forceps, baskets, balloon catheters.
Surgical (thoracotomy/bronchotomy):
- Reserved for failed endoscopy, impacted/deeply embedded FBs.
Key principle: Never delay — organic FBs absorb moisture, swell, and cause progressive inflammation and granulation tissue that makes extraction progressively more difficult.
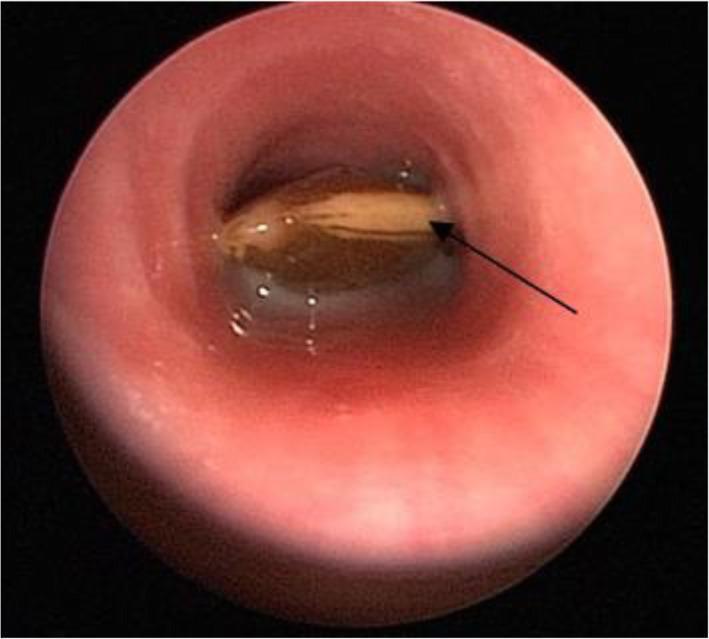
PART 3 — FOREIGN BODIES OF THE ESOPHAGUS
3.1 Sites of Lodgement
The esophagus has three anatomical narrowings where objects impact:
- Cricopharyngeus muscle (UES) — most common (C5–C6 level)
- Level of aortic arch — T4
- Diaphragmatic hiatus (LES) — least common
Spicules of bone (fish/chicken bones) most commonly lodge in the inferior tonsil, tongue base, or vallecula. Larger objects lodge at the cricopharyngeus. — Cummings Otolaryngology
3.2 Risk Groups
- Children (coins, toys, batteries)
- Elderly with loose dentures
- Psychiatric patients (intentional)
- Prisoners (deliberate ingestion)
- Patients with underlying esophageal pathology (stricture, ring, achalasia)
3.3 Clinical Features
- Dysphagia (solids > liquids)
- Odynophagia
- Hypersalivation ("drooling")
- Inability to swallow saliva (sign of complete obstruction)
- Chest/neck pain
- Regurgitation
Red flags: Fever, subcutaneous emphysema, mediastinal widening → perforation and mediastinitis.
3.4 Diagnosis
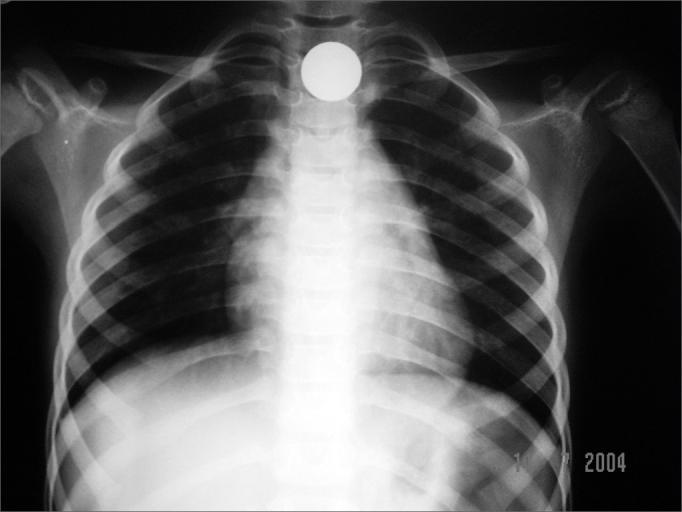
- Plain X-ray (lateral soft tissue neck + PA chest): Radiopaque FBs visible directly. Indirect signs of perforation: pneumomediastinum, prevertebral soft tissue swelling, gas in fascial planes.
- Important radiological point: A coin in the esophagus appears face-on (en face) on AP view (coronal orientation); a coin in the trachea appears on edge (sagittal) — because the tracheal rings hold it in a different plane.
- CT if radiographs are negative but clinical suspicion persists (superior for soft-tissue-density FBs like fish bones).
- Water-soluble contrast swallow if perforation suspected (not barium — barium causes mediastinal granuloma).
- Endoscopy is both diagnostic and therapeutic.

3.5 Management — by FB Type
| FB Type | Action |
|---|---|
| Food bolus (meat) | Urgent endoscopy within 12 hours; gentle push or piecemeal extraction |
| Small blunt (coin) | Endoscopic removal from esophagus; observation if below esophagus |
| Sharp/pointed | Emergency — remove regardless of location; grasp from blunt end |
| Long (>6 cm) | Emergency; cannot negotiate duodenal curve |
| Button battery | Absolute emergency (liquefactive necrosis within hours); remove immediately |
| Multiple magnets | Emergency; can create pressure necrosis and fistulas between bowel loops |
Any FB in the esophagus must be removed — pressure necrosis with perforation may otherwise occur. Sharp or long FBs carry perforation risk of 15–35%. — Cummings Otolaryngology
After removal: Assess esophagus for underlying pathology (present in ~90% of adult cases — stricture, ring, eosinophilic esophagitis). — Cummings Otolaryngology
PART 4 — ENDOTRACHEAL INTUBATION
4.1 Definition & Purpose
Placement of a tube through the mouth (orotracheal) or nose (nasotracheal) via the glottis into the trachea to:
- Secure and protect the airway
- Enable mechanical ventilation
- Facilitate suction of secretions
- Administer anaesthetic gases
4.2 Indications
- Respiratory failure (apnoea, severe hypoxia)
- Airway protection (GCS ≤ 8, risk of aspiration)
- Upper airway obstruction (angioedema, trauma, epiglottitis — use with caution)
- General anaesthesia
- Cardiorespiratory arrest
4.3 Technique (Rapid Sequence Intubation — RSI)
- Pre-oxygenation — 3–5 minutes of 100% O₂.
- Pre-medication — Atropine (children), lidocaine (raised ICP).
- Induction agent — Propofol, ketamine, or thiopentone.
- Paralytic agent — Succinylcholine (fastest onset, 1–2 min) or rocuronium.
- Cricoid pressure (Sellick's manoeuvre) — controversial but still used.
- Laryngoscopy — Direct (Macintosh blade) or video laryngoscopy.
- Tube placement — Cuffed ETT placed through cords; cuff inflated to 20–30 cmH₂O.
- Confirmation: Capnography (gold standard), bilateral air entry, chest rise, misting of tube, CXR.
4.4 Complications of Intubation
Immediate:
- Failed intubation / oesophageal intubation (must confirm immediately with ETCO₂)
- Laryngospasm, bronchospasm
- Dental injury
- Hypoxia during attempts
- Haemorrhage
- Arytenoid dislocation
Delayed:
- Subglottic stenosis (prolonged intubation > 2 weeks; incidence historically 3–12% after tracheostomy)
- Laryngeal granulomas
- Tracheomalacia
- Sinusitis (nasotracheal)
Anterior neck trauma or possible laryngotracheal injury is a relative contraindication to orotracheal intubation; tracheostomy is preferred in such cases. — Pfenninger and Fowler's Procedures for Primary Care
PART 5 — TRACHEOSTOMY
5.1 Definition
A surgical procedure in which an opening (stoma) is made through the anterior neck into the trachea and a tube is inserted to maintain a patent airway. — Gray's Anatomy for Students
5.2 Indications
Emergency:
- Upper airway obstruction from FB not amenable to intubation
- Severe laryngeal oedema (anaphylaxis, angioedema)
- Severe head/neck trauma with laryngeal fracture
- Failed intubation
Elective / Semi-elective:
- Prolonged mechanical ventilation (> 7–14 days)
- Bilateral vocal cord paralysis
- Laryngeal carcinoma (obstructing tumour)
- Obstructive sleep apnoea (severe, refractory)
- Neuromuscular diseases impairing airway protection (MND, Guillain–Barré)
- Post-laryngectomy (permanent stoma)
5.3 Types
| Type | Description |
|---|---|
| Surgical tracheostomy | Standard open procedure in theatre |
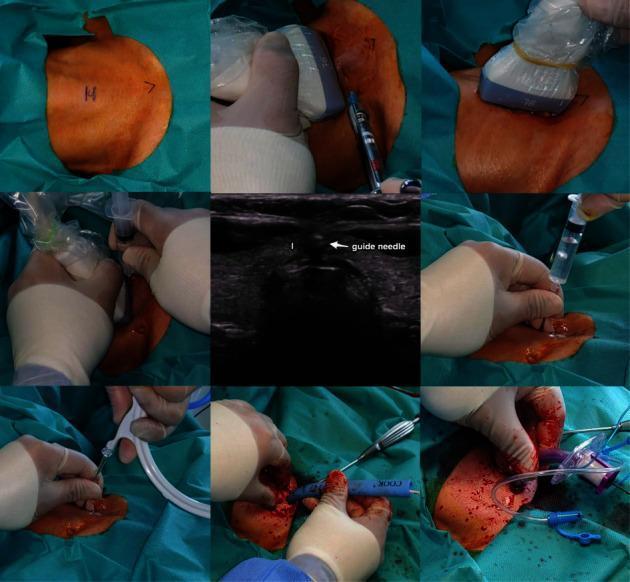
| Percutaneous dilatational tracheostomy (PDT) | Bedside procedure using Seldinger technique + serial dilation; preferred in ICU |
| Cricothyroidotomy | Emergency access through cricothyroid membrane; faster but limited to short-term use |
| Mini-tracheostomy | Small-bore tube for sputum clearance; does not facilitate IPPV |
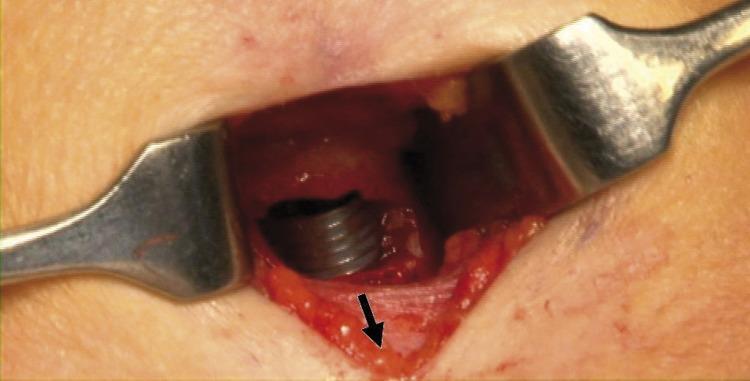
5.4 Surgical Technique (Standard Open)
- Position: Supine, neck extended (sandbag under shoulders).
- Incision: Transverse incision in the lower third of the neck anteriorly (2 cm above the sternal notch).
- Dissection: Strap muscles retracted laterally; thyroid isthmus divided if necessary.
- Tracheal opening: Incision through the 2nd and 3rd tracheal rings (never above the 1st ring — risk of subglottic stenosis).
- Tube insertion: Appropriate-sized cuffed tracheostomy tube inserted; cuff inflated.
- Securing: Tube tied with tapes; first tube change at 5–7 days (tract established). — Gray's Anatomy for Students
5.5 Complications
Early (0–48 h):
- Haemorrhage (most common early complication)
- False passage / tube displacement
- Subcutaneous emphysema / pneumothorax
- Apnoea (over-sedation)
- Tube blockage with mucus
Intermediate (days–weeks):
- Wound infection
- Tube displacement (life-threatening before tract is established)
- Tracheoinnominate artery fistula (rare, 0.3%; presents with herald bleed — surgical emergency)
- Aspiration / swallowing dysfunction
Late:
- Tracheal stenosis — historically 3–12% after tracheostomy; a common indication for tracheal reconstruction — Schwartz's Principles of Surgery
- Tracheomalacia
- Tracheo-oesophageal fistula
- Persistent stoma (>2 weeks after tube removed)
- Scarring / keloid
5.6 Decannulation
- Once the underlying problem resolves, the tracheostomy tube is simply removed.
- The stoma closes spontaneously without intervention in the vast majority of cases. — Gray's Anatomy for Students
- Progressive downsizing ("weaning") before decannulation.
- Patients with long-term tracheostomies cannot vocalise because no air passes through the vocal cords → a speaking valve (e.g., Passy-Muir valve) occludes the tube on expiration, directing airflow through the larynx.
Summary Table
| Topic | Key Fact |
|---|---|
| Chronic laryngitis | LPR is the most common current cause; PPIs are first-line |
| Vocal nodules | At junction of anterior 1/3 / posterior 2/3; voice therapy first |
| Laryngeal TB | Posterior larynx; secondary to pulmonary TB; "turban epiglottis" |
| Laryngeal SCC | Glottic tumours present earliest (hoarseness); tobacco + alcohol |
| FB in bronchi | Right main bronchus preferred; expiratory film shows air-trapping |
| FB in esophagus | UES most common site; button battery = absolute emergency |
| Intubation | Confirm with capnography; cuff pressure 20–30 cmH₂O |
| Tracheostomy | Incision through rings 2–3; tracheoinnominate fistula = rare but fatal |
Sources: Cummings Otolaryngology Head and Neck Surgery; Murray & Nadel's Textbook of Respiratory Medicine; Gray's Anatomy for Students; Schwartz's Principles of Surgery; Pfenninger and Fowler's Procedures for Primary Care; Goldman-Cecil Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.