Giddiness history
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive guide to taking a history of giddiness (dizziness/vertigo):
History Taking for Giddiness
1. Define the Symptom First
Never accept "dizziness" or "giddiness" as a final descriptor. Ask the patient to characterise it into one of three categories:
| Category | Description |
|---|---|
| Vertigo | Sensation of movement of self or surroundings (spinning) |
| Pre-syncope / Lightheadedness | Feeling faint, "about to pass out" |
| Disequilibrium / Imbalance | Unsteadiness without abnormal head sensation |
Caution: patient descriptions can be unreliable and overlapping — timing and triggers are often more diagnostically useful than symptom type alone.
— Bradley and Daroff's Neurology in Clinical Practice
2. Key History Questions
Onset & Timing
- When did it first start?
- Continuous or episodic?
- Duration of each episode (seconds / minutes–hours / days)?
- Frequency? Last episode?
- Do symptoms fully resolve between episodes?
Triggers
- Positional changes (rolling in bed → BPPV)?
- Standing up (orthostatic hypotension)?
- Head movements?
- Sound or pressure changes (perilymph fistula)?
- Salty food intake (Menière's disease)?
- Stress, exercise, excitement (familial ataxia)?
- Migraine triggers (light, stress)?
Mitigating / Exacerbating Factors
- What makes it better or worse?
- Does visual fixation suppress it?
Severity
- Does it limit daily activities or cause falls?
3. Associated Symptoms
Ear (Labyrinthine) Symptoms
- Hearing loss (unilateral or bilateral, fluctuating?)
- Tinnitus (pulsatile or ringing?)
- Aural fullness
- Autophony
- Otorrhoea / otalgia
- Nausea, vomiting, sweating, diarrhea (autonomic features of true labyrinthine vertigo)
Neurological Symptoms (should NOT be present with pure labyrinthine vertigo — their presence points to a central cause)
- Extremity weakness or numbness
- Cranial nerve deficits (diplopia, facial weakness, dysphagia)
- Headache / visual aura / photophobia / phonophobia
- Memory loss or personality change
- Ataxia
Cardiovascular
- Palpitations (arrhythmia)
- Chest pain
- Syncope
4. Medication History
- Current medications (aminoglycosides, loop diuretics, antihypertensives, antiepileptics — all ototoxic or vestibulotoxic)
- Polypharmacy in the elderly is a major cause of chronic dizziness
5. Past Medical & Surgical History
- Prior ear infections, ear surgery, head trauma
- Hypertension, diabetes, cardiovascular disease
- Autoimmune disease (relevant for immune-mediated labyrinthitis)
- Migraines
6. Family History
- Hereditary hearing loss or vestibular disorders
- Familial ataxia syndromes
7. Social History
- Noise exposure (occupational or recreational)
- Tobacco and alcohol use
- Caffeine/stimulant intake (can exacerbate tinnitus and dizziness)
8. Differential Diagnosis by Duration — Key Pointer
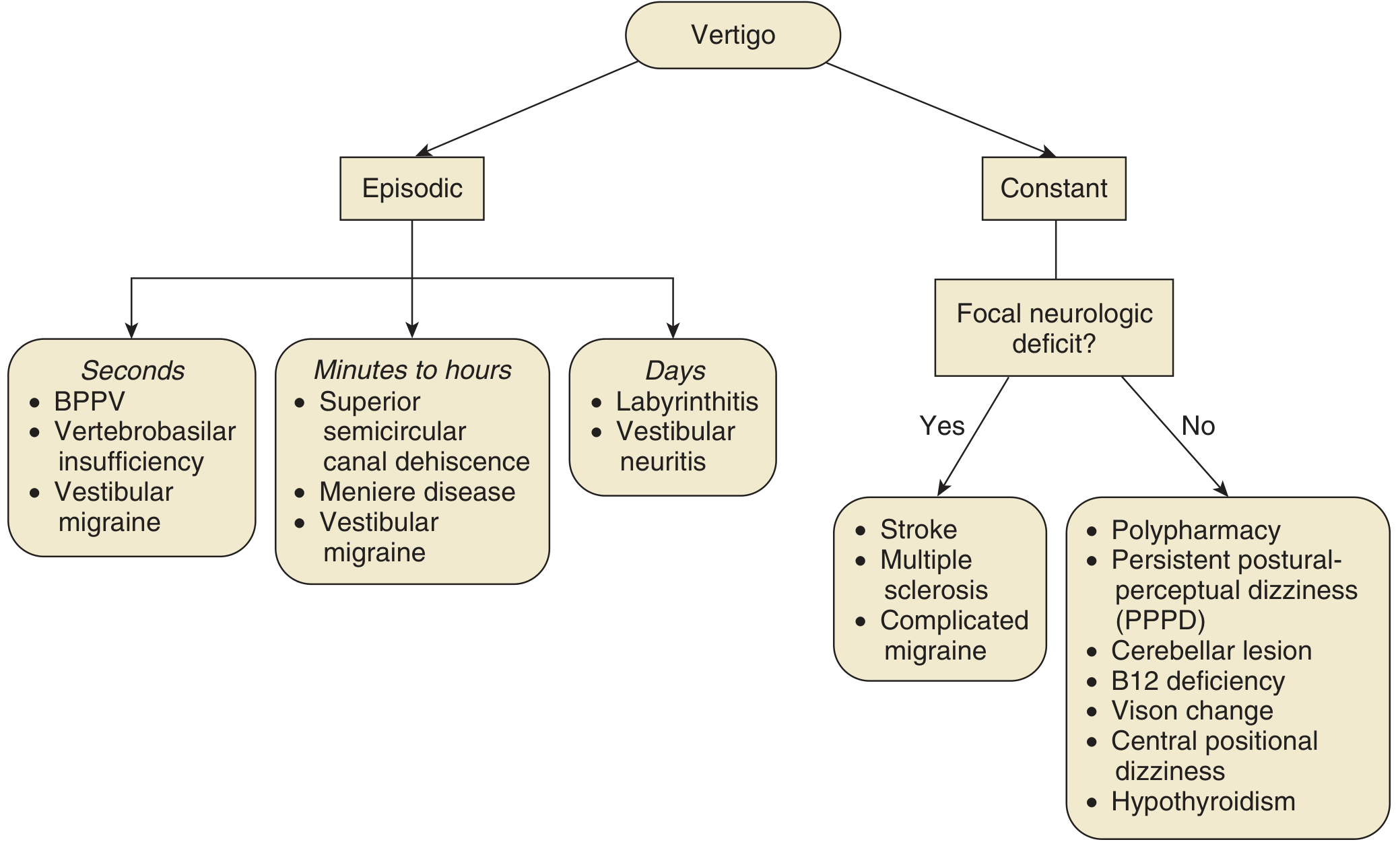
Fig. 137.5 — Establishing a differential diagnosis with a chief complaint of vertigo (Cummings Otolaryngology)
| Duration | Think of |
|---|---|
| Seconds | BPPV, vertebrobasilar insufficiency, vestibular migraine |
| Minutes–hours | Menière's disease, superior canal dehiscence, vestibular migraine |
| Days | Labyrinthitis, vestibular neuritis |
| Constant + focal neurology | Stroke, MS, complicated migraine |
| Constant, no focal neurology | Polypharmacy, PPPD, cerebellar lesion, B12 deficiency, hypothyroidism, vision change |
9. Summary Table for History Taking in Vertigo
| Domain | Key Questions |
|---|---|
| Symptom description | Spinning? Faintness? Imbalance? |
| Onset & duration | Sudden/gradual? Seconds/hours/days? |
| Pattern | Continuous or episodic? Frequency? |
| Triggers | Positional? Standing? Sound? |
| Associated ear sx | Hearing loss, tinnitus, fullness, otorrhoea |
| Neurological sx | Weakness, diplopia, headache, ataxia |
| Autonomic sx | Nausea, vomiting, sweating |
| Medications | Ototoxics, antihypertensives, polypharmacy |
| PMH/FH/SH | Ear disease, migraine, cardiovascular, noise exposure |
— Cummings Otolaryngology Head and Neck Surgery; Bradley and Daroff's Neurology in Clinical Practice
Seizure history
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have comprehensive content from authoritative sources. Let me synthesise a complete seizure history guide.
History Taking for Seizures
The clinical history is the cornerstone of seizure evaluation. Since the patient often has impaired consciousness during the event, obtaining a witness account is equally — sometimes more — important than the patient's own account.
1. Obtain History from Both Patient AND Witness
- Interview patient and witness separately where possible to assess consistency
- Witness's recollection may be distorted by panic — try to get more than one witness
- Ask family if they have captured events on home video — invaluable
- Construct the event in temporal order: Prodrome → Aura → Ictus (ictal phase) → Postictal
— Bradley and Daroff's Neurology in Clinical Practice
2. The Event Itself — Phase by Phase
Prodrome (hours to days before)
- Mood change, irritability, headache, sleep disturbance?
- Not part of the seizure itself but may warn of an impending event
Aura (seconds before — focal onset marker)
- Any warning the patient noticed just before losing awareness?
- Type of aura localises the epileptogenic zone:
| Aura Type | Likely Localisation |
|---|---|
| Epigastric rising sensation | Temporal lobe (mesial) |
| Déjà vu / jamais vu | Temporal lobe |
| Fear / psychic symptoms | Temporal (amygdala) |
| Visual (lights, colours) | Occipital lobe |
| Tingling / numbness | Parietal lobe |
| Motor twitching of one limb | Frontal/motor cortex |
| Olfactory hallucination | Temporal (uncus) |
Ictal Phase (the seizure itself — from witness)
- How did it begin? (focal jerking, eye deviation, head turn, automatisms?)
- Consciousness — fully aware, partially aware, or lost?
- Motor features: tonic (stiffening), clonic (rhythmic jerking), tonic-clonic, atonic (drop)?
- Automatisms: lip smacking, chewing, fumbling, picking, wandering?
- Eye deviation or head turn (lateralising — often contralateral to focus)
- Vocalisations or cry at onset (tonic-clonic)?
- Tongue biting (lateral biting = tonic-clonic seizure; tip biting = non-epileptic)
- Urinary or fecal incontinence?
- Colour: cyanosed, flushed, pale?
- Duration of the event?
Postictal Phase
- Confusion, drowsiness, amnesia?
- Duration of postictal confusion (longer = more severe seizure)
- Headache?
- Muscle soreness / aching?
- Todd's paralysis (focal weakness after focal motor seizure)?
- Able to recall the event? (Absent in GTC; present in focal aware seizures)
Absence seizures are a notable exception — no postictal phase
3. Seizure Frequency and Pattern
- First-ever seizure or recurrent?
- Age at first seizure
- Total number of seizures / frequency
- Clustering? (multiple in 24 hours)
- Any change in seizure type or frequency recently?
- Longest seizure-free interval?
- Status epilepticus ever?
4. Precipitating Factors / Triggers
| Trigger | Relevance |
|---|---|
| Sleep deprivation | Very common — lowers seizure threshold |
| Alcohol (use or withdrawal) | Direct proconvulsant effect |
| Drug use / withdrawal | Benzodiazepine, antiseizure drug non-compliance |
| Fever / infection | Especially in children |
| Flashing lights / TV screens | Photosensitive epilepsy |
| Menstrual cycle | Catamenial epilepsy |
| Stress / emotional upset | Common trigger |
| Missed medication | Most common cause of breakthrough seizures |
| Hyperventilation | Triggers absence seizures |
| Exercise, sudden movement | Paroxysmal dyskinesia vs. seizure |
5. Past Medical History
- Perinatal/birth history: hypoxia, prematurity, neonatal seizures
- Developmental milestones: regression or delays suggest underlying syndrome
- Febrile seizures in childhood (associated with mesial temporal lobe epilepsy)
- CNS infections: meningitis, encephalitis, brain abscess
- Head trauma: loss of consciousness, depressed skull fracture, intracranial pathology
- Stroke or cerebrovascular disease (especially in elderly-onset epilepsy)
- Brain tumours or neurosurgery
- Neurocutaneous disorders: tuberous sclerosis, neurofibromatosis, Sturge-Weber
- Metabolic disorders: hypoglycaemia, hyponatraemia, renal/hepatic failure
- Psychiatric history: anxiety, depression (non-epileptic attack disorder common)
6. Drug and Medication History
- Current antiseizure medications (ASMs) and compliance
- Recent dose changes or new prescriptions
- Drugs that lower seizure threshold: tramadol, bupropion, clozapine, ciprofloxacin, theophylline, isoniazid
- Drug-drug interactions with ASMs
- Recreational drugs, alcohol (especially withdrawal)
- Women of reproductive age: pregnancy (affects ASM clearance), oral contraceptive interaction with enzyme-inducing ASMs
7. Family History
- Afebrile seizures in first- or second-degree relatives
- Febrile seizures
- Other paroxysmal disorders (migraine, syncope)
- Ask a senior female relative for best family history recall
- Genetic epilepsy syndromes (Dravet, GEFS+, juvenile myoclonic epilepsy)
8. Social History
- Driving (legal obligation to report seizures in most jurisdictions)
- Occupation (working at heights, with machinery, near water — safety risk)
- Alcohol and substance use
- Sleep habits
- Psychosocial stressors
9. Seizure Classification (ILAE 2017) — guides history taking
| Onset | Type |
|---|---|
| Focal onset | Aware (previously: simple partial) or Impaired awareness (previously: complex partial) → may evolve to bilateral tonic-clonic |
| Generalised onset | Absence, myoclonic, tonic, clonic, tonic-clonic, atonic |
| Unknown onset | Tonic-clonic, behaviour arrest, others |
10. Differential Diagnosis — Key Distinguishing Questions
| Condition | Clues from History |
|---|---|
| Syncope | Prodrome of nausea/pallor/sweatiness; triggered by pain/standing; brief confusion; quick recovery |
| Non-epileptic attack disorder (NEAD/pseudoseizure) | Psychiatric history, prolonged events, suggestible triggers, eyes closed during event, no postictal confusion, high symptom burden |
| TIA | Negative symptoms (weakness, numbness), no postictal phase |
| Migraine with aura | Visual aura evolves slowly; headache follows |
| Narcolepsy/cataplexy | Triggered by emotion; preserved consciousness throughout |
| BPPV/panic attack | Positional or anxiety context; no loss of consciousness |
Summary Checklist
| Domain | Key Points |
|---|---|
| Source | Patient + witness + video |
| Phases | Prodrome → Aura → Ictus → Postictal |
| Ictal features | Onset, motor type, awareness, lateralising signs, autonomic, duration |
| Postictal | Confusion duration, Todd's paresis, tongue bite, incontinence |
| Pattern | Frequency, clustering, change over time |
| Triggers | Sleep, alcohol, drugs, fever, menses, missed medication |
| PMH | Birth, febrile seizures, CNS infection, head injury, stroke |
| Medications | Current ASMs, compliance, interactions, pregnancy |
| Family Hx | Seizures, febrile convulsions, paroxysmal disorders |
| Social | Driving, occupation, safety, alcohol/drugs |
— Bradley and Daroff's Neurology in Clinical Practice; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.