Embryological basis of caudal regression syndrome
Reading File
Finding Sources
Searching PubMed
"caudal regression syndrome" embryology pathogenesis
Searching the Web
caudal regression syndrome embryological basis mechanism
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough answer.
Caudal Regression Syndrome — Embryological Basis
Definition
Caudal regression syndrome (CRS) is a spectrum of congenital malformations resulting from defective development of the caudal end of the embryo, encompassing varying degrees of agenesis of the sacrum and lower lumbar vertebrae, associated lower limb anomalies, and malformations of the genitourinary and gastrointestinal systems. The term was coined by Duhamel (1961), who described the association of these "coincidentally" occurring malformations.
Incidence: 1–5 per 100,000 live births; classically ~3 per 1,000 diabetic pregnancies.
Critical Embryological Window
The insult occurs during weeks 4–5 of gestation (when the fetus is less than 10 mm crown-rump length). This is the window during which:
- The caudal somites are undergoing differentiation
- The cloaca is being divided by the urorectal septum
- Mesonephric duct contact with the cloaca is established
- Müllerian (paramesonephric) ducts are forming
- Limb buds are condensing from somites 25–29
- The lower lumbar and sacral vertebrae are being laid down in a cranio-caudal sequence
— Campbell-Walsh-Wein Urology; Creasy & Resnik's Maternal-Fetal Medicine
Core Embryological Mechanism
1. Paraxial Mesoderm and the Tail Bud
The paraxial mesoderm — which flanks the notochord and gives rise to somites, vertebrae, and associated structures — is formed by two mechanisms:
- Gastrulation, for most of the body axis (cranial to caudal)
- A specialized tail bud (the ventral ectodermal ridge), which drives posterior/caudal extension
"Disruption in this caudal center results in caudal regression syndrome, which is characterized by defects in the most caudal vertebrae, legs, and genitourinary systems." — Creasy & Resnik's Maternal-Fetal Medicine
2. Somitogenesis and the "Clock and Wavefront" Model
Somite formation progresses in a strict anterior-to-posterior sequence, controlled by an oscillating gene expression system called the segmentation clock:
- FGF8 (high caudally) and retinoic acid/RA (high cranially) form opposing gradients; their intersection triggers segmentation of the paraxial mesoderm
- The segmentation clock involves Notch, WNT, SHH, and FGF signalling pathways
- Key downstream factors include Hairy1/HES7/HER1 (Notch pathway)
- Approximately 42–44 somites form at a rate of 2 per side every 4–5 hours
Disruption of this clock at the level of the caudal somites produces the CRS malformation spectrum.
3. Multi-Organ Impact from a Single Insult
Because so many systems are developing simultaneously in the caudal region during weeks 4–5, a single insult produces a constellation of defects:
| System | Embryological structure affected |
|---|---|
| Lumbosacral vertebrae | Caudal somite → sclerotome → vertebral column |
| Lower limbs | Somites 25–29 → limb bud condensation |
| Kidneys & ureters | Ureteric bud from mesonephric duct |
| Bladder & urethra | Urogenital sinus division of cloaca |
| Müllerian ducts | Paramesonephric duct formation |
| Rectum & anus | Dorsal division of cloaca → hindgut |
"A disturbance in segmentation at the level of the caudal somites when the fetus is less than 10 mm (fourth to fifth weeks of human development) can affect many organ systems." — Campbell-Walsh-Wein Urology
The cranio-caudal direction of somite differentiation also explains why earlier insults cause more severe, higher-level anomalies (e.g., higher anorectal malformations with greater upper urinary tract and spinal involvement), while later insults produce milder lower-level defects.
Proposed Cellular Mechanisms
Three cellular mechanisms have been proposed for the primary insult:
- Disordered mesodermal migration — failure of mesodermal cells to migrate to and populate the caudal region (Kallen & Winberg, 1974)
- Reduced cellular proliferation — insufficient mitosis in the caudal eminence/tail bud
- Premature apoptosis — accelerated programmed cell death in caudal mesenchyme, truncating further development (Alles & Sulik, 1993)
These mechanisms ultimately disrupt the caudal eminence (the secondary neurulation center caudal to the posterior neuropore, which normally closes by day 28), impairing formation of the distal neural tube, caudal mesenchyme, and hindgut.
Role of Maternal Diabetes
Maternal diabetes is the strongest known risk factor:
- Insulin-dependent diabetic mothers have a ~1% risk of an affected child
- ≥16% of children with sacral agenesis have an insulin-dependent diabetic mother
- The disorder has been experimentally reproduced in chick embryos by exposure to insulin
The molecular link involves SHH (Sonic Hedgehog) signalling:
"Both [sacral agenesis and holoprosencephaly] involve downregulation of SHH. A defect at the same chromosome 7p36.2 locus... affects SHH at the posterior, rather than the anterior, end of the neural tube and results in sacral agenesis. Disturbed insulin metabolism may affect SHH in programming the neural tube." — Bradley and Daroff's Neurology in Clinical Practice
Additionally, maternal insulin-antibody complexes cross the placenta and may directly affect caudal mesenchymal development.
Genetic Basis
| Gene/Locus | Association |
|---|---|
| HLXB9 (chromosome 7q36) | Currarino syndrome triad (sacral agenesis + presacral mass + anorectal malformation); homeodomain protein responsible for neural plate infolding; found in 20/21 familial Currarino cases |
| SHH pathway downregulation | Sporadic CRS in diabetic embryopathy |
| HOX genes (homeobox region) | Specific deletions in mammalian homeobox region reproduce CRS constellation as predicted by Duhamel |
CRS is therefore best understood as a spectrum encompassing sacral meningoceles and anorectal malformations at one end, through isolated sacral agenesis, to sirenomelia at the severe end.
Relationship to Sirenomelia
Sirenomelia ("mermaid syndrome") — complete fusion of lower limbs — represents the extreme end of the caudal regression spectrum. It likely results from even earlier and more complete disruption of caudal mesoderm, including failure of normal vascular supply from paired umbilical arteries to the caudal body.
Imaging Correlate
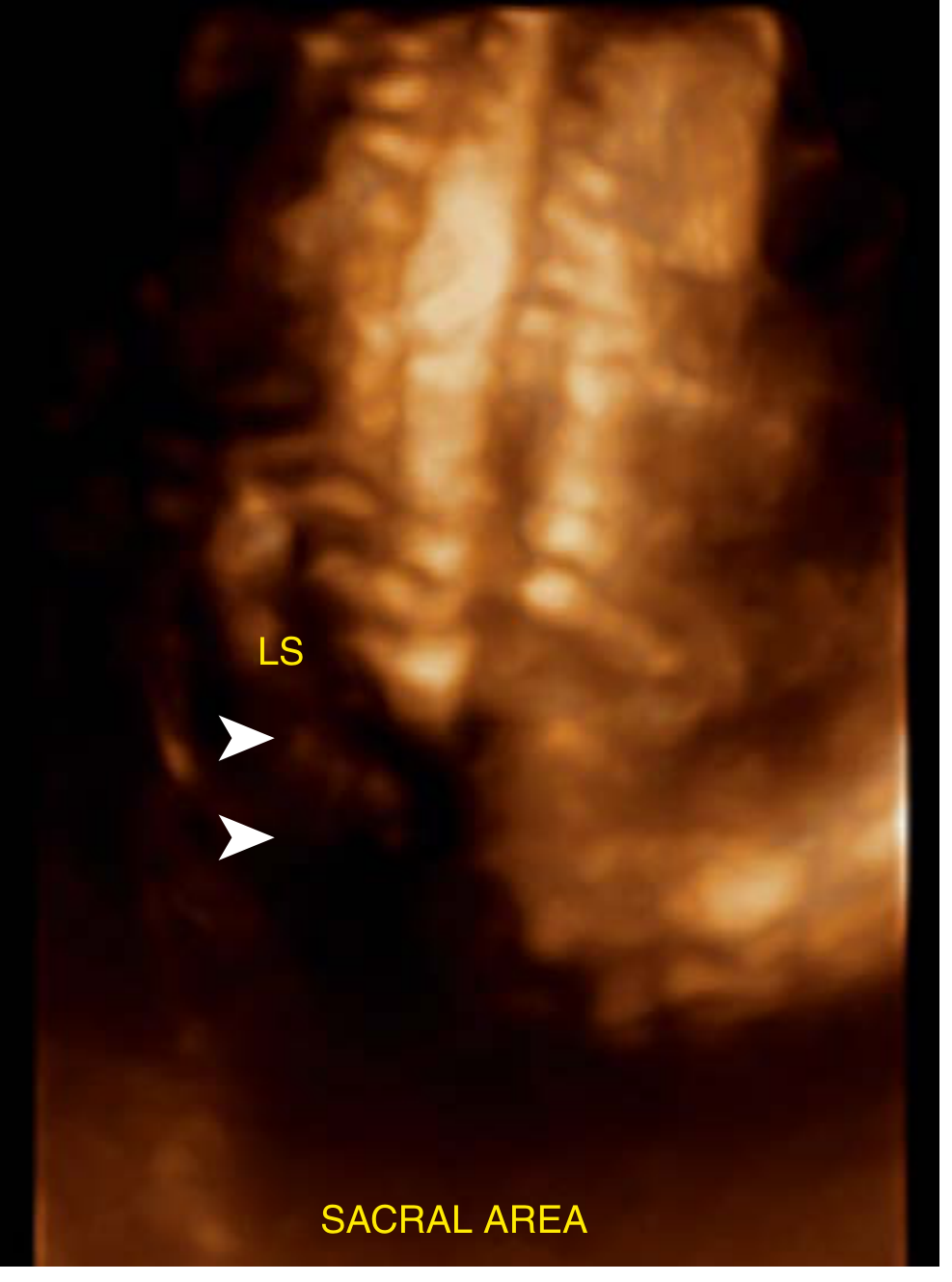
3D ultrasound at 25 weeks in a patient with poor early-pregnancy diabetic control, showing abrupt absence of the sacrum (arrowheads) — Creasy & Resnik's Maternal-Fetal Medicine, Fig. 26.43
Summary
| Feature | Detail |
|---|---|
| Timing of insult | Weeks 4–5 (embryo <10 mm) |
| Primary structure disrupted | Caudal eminence / tail bud (ventral ectodermal ridge) |
| Mechanism | ↓ mesodermal migration + ↓ proliferation + ↑ premature apoptosis |
| Molecular signal | SHH downregulation; Notch/WNT/FGF segmentation clock disruption |
| Strongest extrinsic teratogen | Maternal hyperglycemia (insulin-dependent DM) |
| Genetic cause (familial) | HLXB9 deletion (7q36) → Currarino syndrome |
| Why multisystem? | Cranio-caudal somite differentiation — all caudal structures develop simultaneously during the same narrow window |
Sources: Creasy & Resnik's Maternal-Fetal Medicine; Campbell-Walsh-Wein Urology; Adams & Victor's Principles of Neurology, 12th ed.; Bradley & Daroff's Neurology in Clinical Practice; The Developing Human (Clinically Oriented Embryology); Emery's Medical Genetics and Genomics; Goldman-Cecil Medicine. Recent review: Sánchez-Romero et al., Pediatric Neurology 2025 [PMID: 39642685].
How does maternal diabetes lead to caudal regression syndrome
Finding Sources
Searching PubMed
"caudal regression syndrome" AND "maternal diabetes" AND mechanism
Searching the Web
maternal diabetes caudal regression syndrome mechanism hyperglycemia SHH oxidative stress retinoic acid
Reading File
Searching PubMed
"diabetic embryopathy" AND "caudal" AND (SHH OR "oxidative stress" OR "retinoic acid")
Finding Sources
Reading File
Finding Sources
Searching PubMed
"diabetic embryopathy" AND ("sonic hedgehog" OR "oxidative stress" OR "retinoic acid" OR apoptosis)
Reading Article
PMID: 23702113
Reading Article
PMID: 25434839
Reading Article
PMID: 39209306
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.