what is the role of Vitamin B12 and Folic acid in Redblood cells production
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive explanation of the roles of Vitamin B12 and Folic Acid in red blood cell (RBC) production, drawn from authoritative medical textbooks.
Vitamin B12 and Folic Acid in Red Blood Cell Production
Both vitamins are essential for the maturation and proliferation of red blood cells, but through distinct biochemical mechanisms that ultimately converge on DNA synthesis.
The Core Mechanism: DNA Synthesis
Red blood cells originate from rapidly dividing precursor cells (erythroblasts) in the bone marrow. For these cells to divide and mature, they must replicate their DNA. Both B12 and folate are indispensable for this process.
"Megaloblastic anemia is characterized by enlargement of all rapidly proliferating cells of the body, including marrow cells. The major abnormality is the diminished capacity for deoxyribonucleic acid (DNA) synthesis." — Henry's Clinical Diagnosis and Management by Laboratory Methods
Role of Folic Acid (Folate / Vitamin B9)
Folate, in its active form tetrahydrofolate (FH₄), acts as a carrier of one-carbon units. Its critical functions in RBC production are:
- Synthesis of purines — carbons 2 and 8 of the purine ring are donated by N10-formyl-FH₄
- Synthesis of thymidine (dTMP) — FH₄ donates a methyl group via thymidylate synthase to convert dUMP → dTMP, a key building block of DNA
Without folate, erythroid progenitors cannot synthesize enough DNA to divide properly. Instead of maturing normally, they grow large but fail to divide — producing abnormally large, nucleated cells called megaloblasts. This results in megaloblastic (macrocytic) anemia, characterized by:
- Increased Mean Corpuscular Volume (MCV)
- Hypersegmented neutrophils
- Pancytopenia in severe cases
"A primary result of folic acid deficiency is megaloblastic anemia (large-sized red blood cells, characterized by an increase in mean corpuscular volume [MCV]), which is caused by diminished synthesis of purines and pyrimidines. This leads to an inability of erythropoietic tissue to make DNA and, thereby, proliferate." — Lippincott Illustrated Reviews: Pharmacology
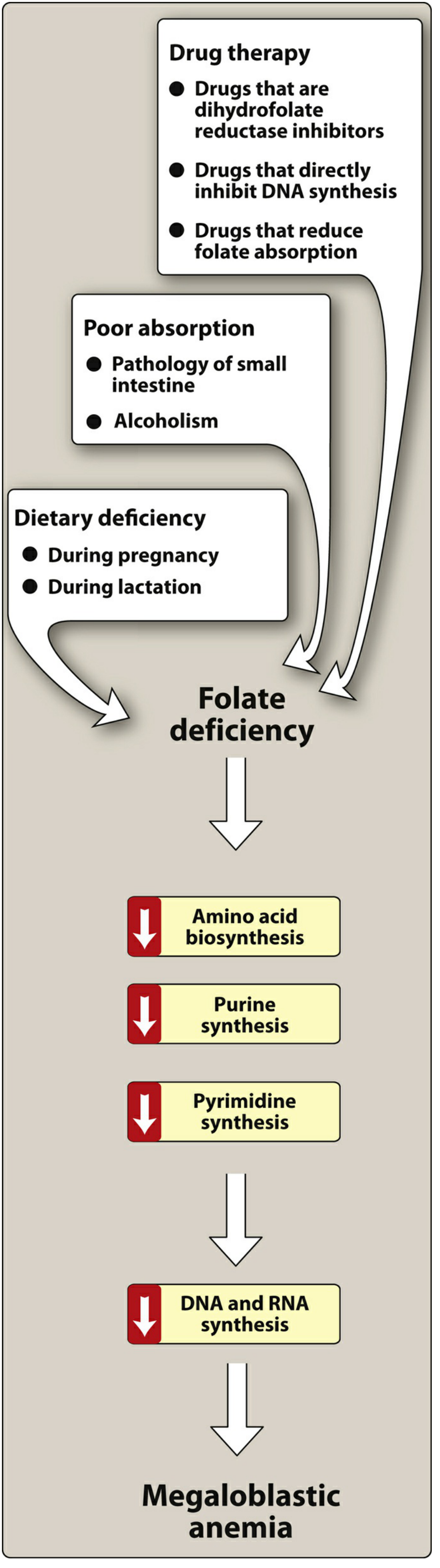
Causes of folate deficiency: increased demand (pregnancy, lactation), poor intestinal absorption, alcoholism, and drugs that inhibit dihydrofolate reductase (e.g., methotrexate, trimethoprim).
Role of Vitamin B12 (Cobalamin)
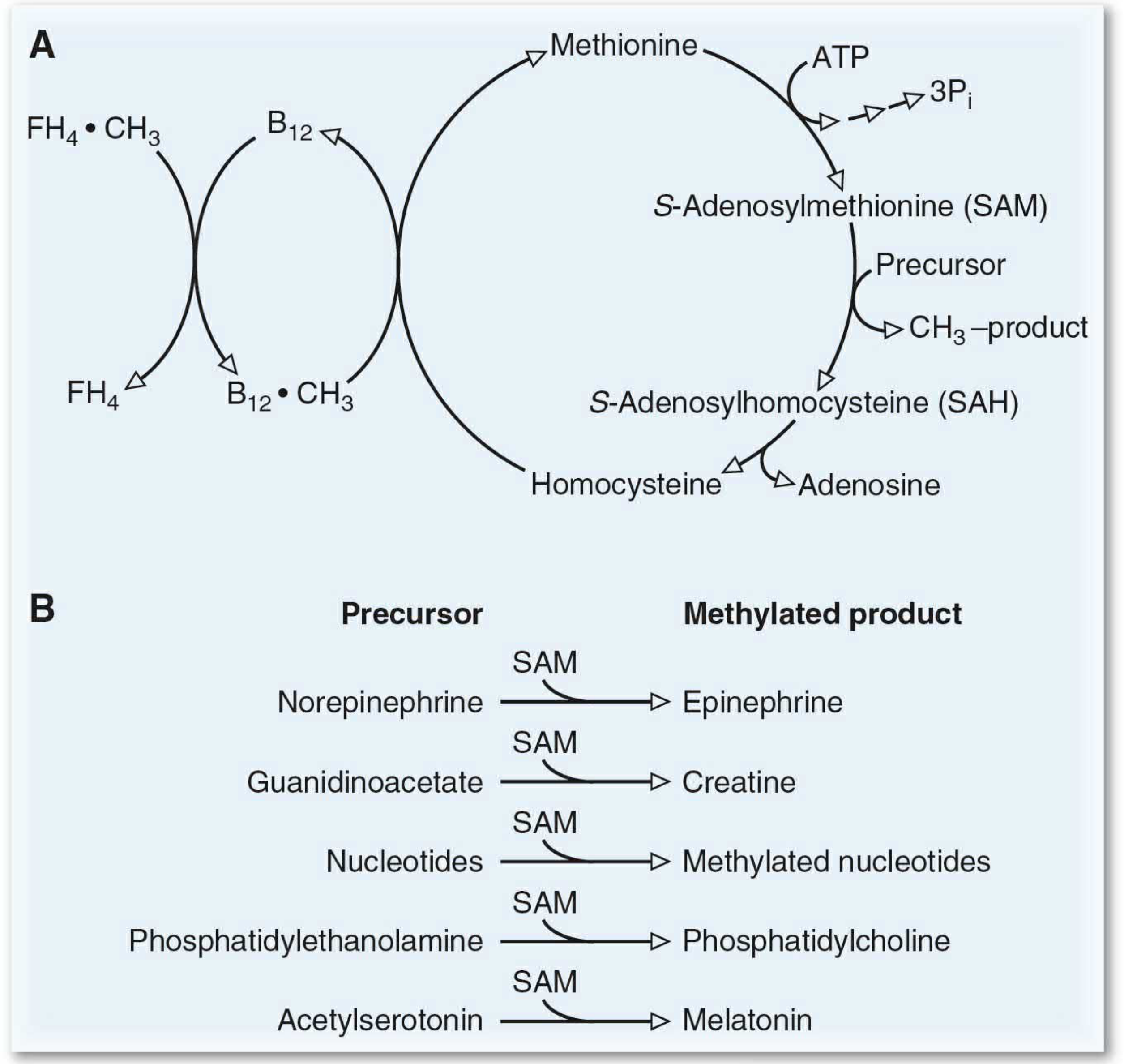
Vitamin B12 supports RBC production primarily through its interdependence with folate metabolism — the methyl-trap hypothesis:
- The enzyme methionine synthase requires B12 (as methylcobalamin) to transfer a methyl group from N5-methyl-FH₄ → FH₄, regenerating free tetrahydrofolate
- This is the only reaction through which the methyl group can leave FH₄ (the formation of N5-methyl-FH₄ is irreversible)
- Without B12, folate becomes trapped as N5-methyl-FH₄ — unavailable for DNA synthesis
- The result: FH₄ derivatives needed for purine and dTMP biosynthesis are depleted → megaloblastic anemia
This is why B12 deficiency produces the same blood picture as folate deficiency, even though the primary block is not in folate itself.
B12 also acts as a coenzyme to reduce ribonucleotides to deoxyribonucleotides, a step directly required for DNA replication.
— Guyton & Hall Textbook of Medical Physiology
Causes of B12 Deficiency
Unlike folate, dietary B12 deficiency is rare (it is found in all animal products). The most common cause is impaired absorption:
- Pernicious anemia: autoimmune destruction of gastric parietal cells → lack of intrinsic factor → B12 cannot be absorbed in the terminal ileum
- Gastric resection, ileal disease, or malabsorption syndromes
Distinguishing the Two Deficiencies
| Feature | B12 Deficiency | Folate Deficiency |
|---|---|---|
| Blood picture | Megaloblastic anemia | Megaloblastic anemia |
| Neurological effects | Yes (subacute combined degeneration of spinal cord) | No |
| Cause | Usually malabsorption (pernicious anemia) | Usually dietary / drugs |
| Serum homocysteine | Elevated | Elevated |
| Serum methylmalonic acid | Elevated | Normal |
Critical warning: Treating B12 deficiency with folic acid alone will correct the blood picture but mask the ongoing neurological damage (demyelination of posterior/lateral spinal columns), which can progress to paralysis. Always determine the cause before treating. — Lippincott Illustrated Reviews: Pharmacology
The Consequences of Deficiency (Summary Diagram)
Summary
- Folic acid directly supplies one-carbon units for purine and thymidine synthesis, enabling DNA replication in dividing erythroid cells
- Vitamin B12 regenerates active FH₄ from its trapped methyl form, making folate available for DNA synthesis; it also reduces ribonucleotides to deoxyribonucleotides
- Deficiency of either vitamin halts erythroid cell division → megaloblastic (macrocytic) anemia
- B12 deficiency uniquely causes irreversible neurological damage due to hypomethylation and methylmalonic acid accumulation in nervous tissue
This is a shared conversation. Sign in to Orris to start your own chat.