How to study ecg
Reading File
Finding Sources
Searching the Web
how to study ECG electrocardiogram systematic approach beginners
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG waveform P wave QRS complex T wave labeled diagram
Reading File
Reading File
Reading File
I now have excellent content from Harrison's and Kaplan & Sadock's. Let me compile a comprehensive guide.
How to Study ECG
Why a Systematic Approach Matters
The most common errors in ECG interpretation are errors of omission — missing something because you didn't look for it. Every expert source, from Harrison's to Kaplan & Sadock's, agrees: always follow a fixed sequence, every single time.
Step 1 — Understand the Basics First
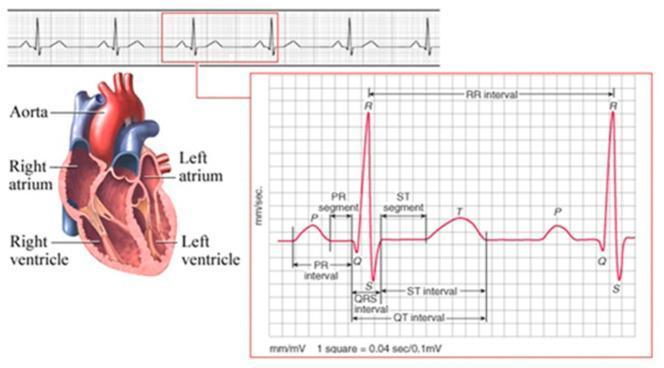
Before reading any ECG, you need to know what the waveforms represent:
| Component | Meaning |
|---|---|
| P wave | Atrial depolarization |
| QRS complex | Ventricular depolarization |
| T wave | Ventricular repolarization |
| U wave | After-repolarization (origin debated) |
| PR interval | AV conduction time (P start → QRS start) |
| QRS interval | Ventricular conduction time |
| QT interval | Total ventricular electrical activity |
| ST segment | Between QRS end and T wave start |
Paper basics:
- Small box = 0.04 sec (horizontal) / 0.1 mV (vertical)
- Large box = 0.2 sec (5 small boxes)
- Standard ECG = 10 seconds long
Step 2 — The 14-Parameter Systematic Checklist
From Harrison's Principles of Internal Medicine (22nd ed.), analyze every ECG in this order:
- Standardization & technical features — Is it calibrated? Any lead misplacement? Artifacts?
- Rhythm — Regular or irregular? P before every QRS?
- Heart rate — Calculate using one of two methods (see below)
- PR interval / AV conduction — Normal: 0.12–0.20 sec (3–5 small boxes)
- QRS interval — Normal: <0.12 sec (<3 small boxes)
- QT/QTc interval — Prolonged QTc >440 ms (men), >460 ms (women)
- Mean QRS electrical axis — Use Leads I and aVF
- P waves — Morphology, presence, regularity
- QRS voltages — High (hypertrophy) or low (effusion, obesity, emphysema)
- Precordial R-wave progression — Should grow V1 → V5
- Abnormal Q waves — Suggests prior infarction
- ST segments — Elevation or depression
- T waves — Inversion, flattening, peaking
- U waves — Prominent in hypokalemia, bradycardia
Always compare with previous ECGs — this is invaluable. — Harrison's Principles of Internal Medicine, p. 1919
Step 3 — Calculating Heart Rate
Method 1 — "Rate by squares" (regular rhythms):
Count large boxes between two R waves → divide 300 by that number.
- Example: 4 large boxes between R waves → 300 ÷ 4 = 75 bpm
Method 2 — "QRS count" (irregular rhythms like AF):
Count all QRS complexes on the 10-second strip → multiply by 6.
- Example: 10 complexes × 6 = 60 bpm
Step 4 — Determine the Axis
- Normal axis: −30° to +90°
- Use Lead I (0°) and aVF (90°) — they are perpendicular to each other
- Both upright → normal axis
- Left axis deviation (LAD): Lead I up, aVF down — seen in LVH (from chronic hypertension)
- Right axis deviation (RAD): Lead I down, aVF up — seen in RVH, pulmonary HTN, congenital disease
Step 5 — Classify the Rhythm
Approach rhythms by two questions:
- Narrow or wide QRS?
- Narrow (<0.12 sec) = supraventricular origin (follows normal conduction)
- Wide (≥0.12 sec) = ventricular origin OR aberrant conduction
- Regular or irregular?
- Regularly irregular → recurring pattern (e.g., Wenckebach)
- Irregularly irregular → completely disorganized (e.g., atrial fibrillation — no clear P waves)
Step 6 — Key ST/T Wave Patterns to Know
| Finding | Think of |
|---|---|
| ST elevation | STEMI, pericarditis, early repolarization, LV aneurysm |
| ST depression | Subendocardial ischemia, digoxin effect |
| T-wave inversion | Ischemia, PE, subarachnoid hemorrhage, myocarditis |
| Peaked T waves | Hyperkalemia (or hyperacute STEMI) |
| Prolonged QT | Drugs, hypokalemia, hypomagnesemia, congenital syndromes |
| Wide QRS | Bundle branch block, ventricular rhythm, hyperkalemia |
Repolarization (ST-T) is an active, ATP-dependent process — making it especially susceptible to ischemia. — Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 6825
How to Build Proficiency — Practical Tips
- Read ECGs daily — volume is everything. Free resources include ECG Wave-Maven (Harvard's self-assessment library) and Lifeinthefastlane.com.
- Use a fixed sequence every time — don't skip steps, even on "obvious" tracings.
- Start with normal — read 50+ normal ECGs before focusing on abnormal ones.
- Learn by pattern recognition — LBBB, RBBB, AF, STEMI, AV blocks each have a visual gestalt.
- Correlate with clinical context — age, sex, symptoms, and medications change interpretation dramatically.
- Reference textbooks:
- Goldberger's Clinical Electrocardiography: A Simplified Approach (10th ed., 2024) — the classic beginner's book
- Harrison's Principles of Internal Medicine (22nd ed.) — Chapter 247 for ECG basics
- Braunwald's Heart Disease — for advanced/cardiology-level detail
Sources
- Harrison's Principles of Internal Medicine, 22nd ed., Chapter 247, p. 1919
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, pp. 6824–6826
This is a shared conversation. Sign in to Orris to start your own chat.