STEP BY STEP PERFORM GAIT ASSESSMNET QUALITATIVE AND QUANTITATIVE PROPERLY
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
gait cycle phases stance swing assessment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Now I have comprehensive content from multiple authoritative textbooks. Let me compile the complete step-by-step gait assessment guide.
Step-by-Step Gait Assessment: Qualitative & Quantitative
PART 1 — FOUNDATIONS: THE NORMAL GAIT CYCLE
Before assessing gait, you must know what normal looks like.
The Gait Cycle
One full gait cycle = heel strike of the same foot to the next heel strike of the same foot (one stride).
| Parameter | Value |
|---|---|
| Stance phase (foot in contact with ground) | 60–65% of cycle |
| Swing phase (foot off ground) | 35–38% of cycle |
| Double-limb support (both feet on ground) | 20–25% of cycle |
| Ground reaction force — walking | ~1.5× body weight |
| Ground reaction force — running | 3–4× body weight |
As gait speed increases, stance phase decreases. Running eliminates double-limb support and introduces a float phase (both feet off ground simultaneously).
— Miller's Review of Orthopaedics, 9th Ed.
The 8 Sub-Phases of the Gait Cycle
| Phase | Abbrev. | Description |
|---|---|---|
| Initial Contact (Heel Strike) | IC | Heel contacts ground; foot slightly inverted/locked |
| Loading Response | LR | Foot flattens; hindfoot passively everts; shock absorption |
| Mid-Stance | MSt | Single-limb support; center of gravity at highest point |
| Terminal Stance | TSt | Heel rises; body weight shifts over forefoot |
| Pre-Swing (Toe-Off) | PSw | Toe leaves ground; swing phase begins |
| Initial Swing | ISw | Hip and knee flex; foot clears ground |
| Mid-Swing | MSw | Limb advances; tibialis anterior contracts concentrically |
| Terminal Swing | TSw | Knee extends; limb decelerates before heel strike |
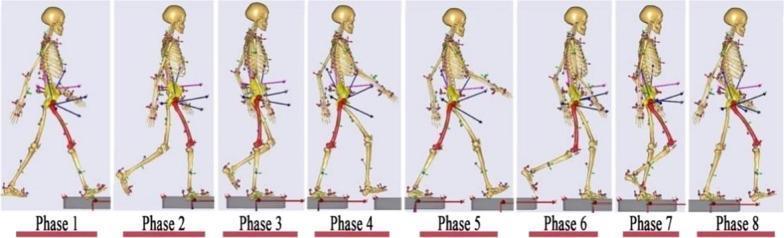
The 8 phases of the gait cycle from initial contact through terminal swing, showing skeletal kinematics and joint angles at each phase.
Key Muscle Actions During Normal Gait
| Muscle | Action | Function in Gait |
|---|---|---|
| Gluteus maximus | Concentric | Powers hip extension |
| Gluteus medius | Eccentric | Controls pelvic tilt at mid-stance |
| Hip adductors | Eccentric | Control lateral sway (late stance) |
| Iliopsoas | Concentric | Powers hip flexion (swing) |
| Quadriceps | Eccentric | Stabilizes knee at initial contact and pre-swing |
| Hamstrings | Eccentric | Control rate of knee extension at terminal swing |
| Tibialis anterior | Concentric/Eccentric | Dorsiflexes ankle in swing; slows plantar flexion at heel strike |
| Gastrocnemius-soleus | Eccentric | Slows dorsiflexion rate during stance; propulsion |
— Miller's Review of Orthopaedics, 9th Ed.
PART 2 — PREPARATION & ENVIRONMENT
Before the patient walks:
- Remove footwear if safe — observe foot shape, callus distribution, shoe wear patterns (heel wear = normal; lateral heel/forefoot = abnormal loading)
- Set a clear walkway ≥6–10 meters, unobstructed
- Note walking aids (cane, walker, crutches) — document which hand holds the cane (should be contralateral to affected limb)
- Document pain level, footwear worn, assistive devices
- Ask about history of falls, fear of falling, duration of any gait problem
PART 3 — QUALITATIVE (OBSERVATIONAL) GAIT ASSESSMENT
Observe from anterior, posterior, and lateral views. Assess systematically from the ground up.
Step 1: Overall Visual Impression
With the patient walking at their natural pace across the room, observe:
- Posture: erect trunk, head forward, arms swinging reciprocally?
- Symmetry: are step lengths and timing equal bilaterally?
- Base of support: narrow (normal: medial malleoli nearly touch) vs. wide vs. scissored
- Cadence: rhythm — is it steady or irregular?
- Arm swing: absent, reduced, or asymmetric (reduced unilateral arm swing → Parkinson's or hemiplegia)
- Foot clearance: any dragging or scuffing?
Normal: "The body is erect, the head is straight, and the arms hang loosely and gracefully at the sides, each moving rhythmically forward with the opposite leg. The feet are slightly externally rotated, the steps are approximately equal in length, and the medial malleoli almost touch as each foot passes the other." — Adams & Victor's Principles of Neurology, 12th Ed.
Step 2: Foot and Ankle (Lateral View)
| Observation | What to look for |
|---|---|
| Heel strike | Does the heel contact first? Absence = equinus, dropfoot, or antalgic gait |
| Foot flat | Complete sole contact at loading response |
| Hindfoot eversion | Passive eversion from heel strike to foot flat (energy absorption) |
| Heel rise | Occurs at terminal stance; requires adequate ankle plantar flexion |
| Toe-off | Clean propulsion through metatarsals |
| Dorsiflexion in swing | Foot clears ground? If not → foot drop / steppage gait |
Step 3: Knee (Lateral + Anterior View)
| Observation | What to look for |
|---|---|
| Flexion at loading | ~15–20° of knee flexion for shock absorption |
| Extension at mid-stance | Near full extension for single-limb support |
| Genu recurvatum | Hyperextension = quadriceps weakness or plantar flexor spasticity |
| Crouch gait | Excessive knee flexion throughout = hamstring contracture, plantar flexor weakness |
| Medial/lateral femoral rotation | Intoeing/out-toeing pattern |
Step 4: Hip and Pelvis (Anterior + Posterior View)
| Observation | What to look for |
|---|---|
| Pelvic drop (Trendelenburg) | Contralateral pelvis drops during single-limb stance → ipsilateral gluteus medius weakness |
| Trunk lateral lean (compensated Trendelenburg) | Trunk shifts ipsilaterally to unload hip abductors |
| Waddling gait | Bilateral pelvic drop → bilateral gluteus medius weakness or proximal myopathy |
| Hip hiking | Ipsilateral pelvis elevated to clear a foot (compensation for foot drop) |
| Scissoring | Legs cross midline → hip adductor spasticity (spastic diplegia, cerebral palsy) |
| Hip flexion contracture | Trunk leans forward to compensate |
Step 5: Trunk and Upper Extremities
| Observation | What to look for |
|---|---|
| Arm swing | Should be reciprocal. Absent/reduced unilaterally → UMN lesion or parkinsonism |
| Trunk flexion | Forward lean → hip flexion contracture or Parkinson's disease |
| Trunk extension | Backward lean → hip extensor weakness |
| Lateral trunk flexion | "Gluteus medius lurch" (Duchenne gait) |
PART 4 — PATHOLOGICAL GAIT PATTERNS (Qualitative Recognition)
| Gait Pattern | Key Feature | Common Cause |
|---|---|---|
| Antalgic | Shortened stance phase on affected side | Pain (OA, fracture, infection) |
| Steppage (footdrop) | Exaggerated hip + knee flexion in swing to clear toe | Tibialis anterior weakness, peroneal nerve palsy, TA rupture |
| Calcaneal | Excessive ankle dorsiflexion at heel strike | Triceps surae weakness |
| Trendelenburg | Contralateral pelvic drop at mid-stance | Gluteus medius weakness (ipsilateral) |
| Waddling | Bilateral pelvic drop, side-to-side lurch | Proximal myopathy, bilateral hip abductor weakness |
| Spastic/Scissor | Stiff-legged, circumduction, toe drag, legs cross midline | Corticospinal lesion, spasticity (stroke, CP, MS) |
| Hemiplegic | Arm flexion + leg circumduction ipsilateral | Contralateral UMN lesion; prolonged stance + double support |
| Parkinsonian | Stooped posture, shuffling, short steps, reduced arm swing, festination | Parkinson's disease, drug-induced parkinsonism |
| Cerebellar ataxic | Wide-based, irregular, staggering, cannot walk heel-to-toe (tandem) | Cerebellar lesion, alcohol, MS |
| Sensory ataxic | Stamping, watching the ground, worse in dark (Romberg +) | Peripheral neuropathy, dorsal column lesion |
| Cautious gait | Abbreviated stride, widened base, lowered center of mass, arms abducted | Fear of falling, age-related, nonspecific |
| Dystonic gait | Twisting, repetitive movements, abnormal foot posture | Dystonia, Parkinson's (early) |
| Choreic gait | Irregular, jerky, dance-like movements | Huntington's disease, levodopa dyskinesia |
| Freezing gait | Brief episodic absence of forward progression despite intent to walk | Parkinson's disease (esp. approaching narrow spaces) |
— Harrison's Principles of Internal Medicine, 22nd Ed.; Miller's Review of Orthopaedics, 9th Ed.; Adams & Victor's Principles of Neurology, 12th Ed.
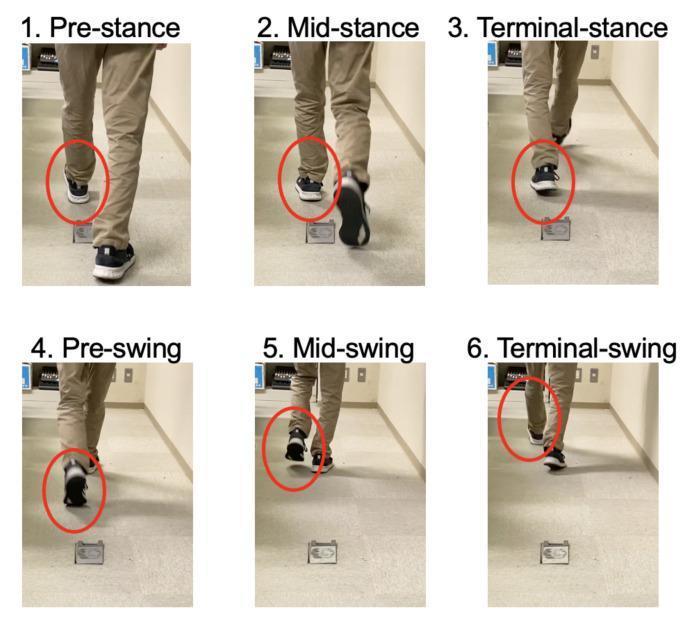
Clinical photograph series showing progression through pre-stance, mid-stance, terminal stance, pre-swing, mid-swing, and terminal swing with ankle position highlighted.
PART 5 — QUANTITATIVE GAIT ASSESSMENT
Quantitative assessment provides objective, reproducible measurements to track change over time or compare to norms.
5.1 Spatiotemporal Parameters (Measured Clinically)
Measure these with a measured walkway (tape on floor), stopwatch, or an instrumented walkway (GAITRite, etc.):
| Parameter | Definition | Normal Adult Values |
|---|---|---|
| Gait speed | Distance ÷ time (m/s) | ~1.2–1.4 m/s |
| Cadence | Steps per minute | ~100–120 steps/min |
| Step length | Distance from one heel strike to contralateral heel strike | ~0.65–0.75 m |
| Stride length | Distance from heel strike to next ipsilateral heel strike | ~1.3–1.5 m |
| Step width (base of support) | Mediolateral distance between successive heel strikes | ~8–12 cm |
| Stance phase % | % of cycle with foot on ground | 60–65% |
| Swing phase % | % of cycle with foot off ground | 35–40% |
| Double support % | Both feet on ground simultaneously | 20–25% |
How to measure gait speed (10-Meter Walk Test):
- Mark a 10-meter walkway (allow 2 m acceleration + 2 m deceleration zones; measure middle 10 m)
- Instruct: "Walk at your comfortable, normal pace"
- Time with stopwatch over the middle 10 meters
- Calculate: speed = 10 ÷ time (seconds) = m/s
- Repeat ×3 and average
Clinical thresholds:
- <0.8 m/s → increased fall risk, functional limitation
- <0.6 m/s → limited community ambulation
5.2 Timed Up and Go (TUG) Test
Purpose: Screens functional mobility, gait, and fall risk.
Protocol (from Miller's Anesthesia & Harrison's):
- Patient seated in standard chair (seat height ~43 cm, no armrest use if possible)
- Instruction: "When I say go, stand up, walk 10 feet (3 m), turn around, walk back, and sit down."
- Start timing on "go", stop when seated
- No physical assistance; walking aid permitted if normally used
Interpretation:
| Time | Clinical Significance |
|---|---|
| <12 seconds | Normal — low fall risk |
| ≥12 seconds | High fall risk; warrants further assessment |
| ≥15 seconds | Significantly impaired; associated with postoperative complications |
| >30 seconds | Severely impaired; dependent for most transfers |
— Harrison's Principles of Internal Medicine, 22nd Ed.; Miller's Anesthesia, 10th Ed.
5.3 Additional Functional Tests
| Test | Protocol | Interpretation |
|---|---|---|
| 30-Second Sit-to-Stand | Count repetitions of sit→stand from standard chair (no arms) in 30 s | <8 repetitions → weakness/fall risk |
| 5× Sit-to-Stand | Time to complete 5 repetitions sit→stand | >12 s → functional impairment |
| 6-Minute Walk Test | Distance walked in 6 minutes at self-selected pace | <300 m → significant impairment |
| Tandem gait (heel-to-toe) | Walk along a line, heel to toe, 5+ steps | Inability → cerebellar dysfunction |
| Romberg test | Stand feet together, eyes open → eyes closed | Sway/fall with eyes closed = sensory ataxia |
5.4 Advanced/Instrumented Quantitative Methods
For clinical research or complex cases:
| Method | What it Measures |
|---|---|
| Instrumented walkways (e.g., GAITRite) | Spatiotemporal parameters automatically |
| 3D motion capture | Joint kinematics (hip/knee/ankle angles) and kinetics throughout the cycle |
| Force plates | Ground reaction forces, center of pressure |
| Dynamic EMG | Timing and magnitude of muscle activation |
| Wearables / IMUs | Step count, cadence, stride variability in real-world settings |
"Quantitative gait analysis, with devices such as instrumented walkways, motion capture systems and wearables, is standard in research settings and has the potential to inform diagnosis and treatment of gait disorders when more widely adopted in clinical settings." — Harrison's Principles of Internal Medicine, 22nd Ed.
"Three-dimensional computerized gait analysis with dynamic electromyography and force-plate studies have allowed a more scientific approach to preoperative decision making." — Miller's Review of Orthopaedics, 9th Ed.
PART 6 — SYSTEMATIC OBSERVATION CHECKLIST (Quick Reference)
Use this head-to-toe checklist during observation:
Walking toward you (anterior view):
- Foot progression angle (toe-in / toe-out)
- Step width (narrow/normal/wide)
- Pelvic obliquity / drop
- Trunk sway laterally
- Arm swing symmetry
- Scissoring or hip adduction
Walking away from you (posterior view):
- Heel strike pattern
- Hindfoot valgus/varus alignment
- Pelvic drop (Trendelenburg)
- Trunk shift
- Foot clearance
Walking sideways (lateral view):
- Heel strike → foot flat progression
- Knee flexion/extension pattern (crouch vs. recurvatum)
- Heel rise at terminal stance
- Hip flexion/extension arc
- Forward/backward trunk lean
- Step length
PART 7 — DOCUMENTATION FRAMEWORK
For each patient document:
- Date, patient ID, footwear, assistive device used
- Qualitative descriptors: symmetry, base of support, cadence, arm swing, foot clearance, trunk posture
- Pathological pattern identified (if any) with phase of gait involved
- Quantitative measurements: gait speed (m/s), TUG time, step/stride length, cadence
- Functional classification: community ambulatory (>1.0 m/s), limited community, household ambulatory, non-functional
- Clinical impression and follow-up plan
Key References:
- Miller's Review of Orthopaedics, 9th Ed. — Gait Cycle, Gait Evaluation, Pathologic Gait (Tables 10.1–10.2)
- Adams & Victor's Principles of Neurology, 12th Ed. — Normal Gait (Chapter 6)
- Harrison's Principles of Internal Medicine, 22nd Ed. — Disorders of Gait, TUG Test (Chapter 28)
- Miller's Anesthesia, 10th Ed. — Timed Up-and-Go Protocol
- Bradley & Daroff's Neurology in Clinical Practice — Gait Disorders, Quantitative Analysis
This is a shared conversation. Sign in to Orris to start your own chat.