Uh, send me a picture of a stenotropes tube, uh, from the, uh, front, uh, photo of a human. That's it.
Send me a picture of eustachian tube that is known as, uh, auditory tube. From the forward, uh, from a human, from a fo- uh, picture is taken from the forward, from the, uh, front of a human, uh, like a, uh, passport size photo, then represent only eustachian tube on that photo from where, uh, from, uh, its, its extend from where it, uh, from where to where it extends.
A front-facing passport-style anatomical illustration of a human head and upper neck, like a frontal view. The face is shown transparently or as a cutaway so the internal anatomy is visible. Highlight and label only the Eustachian tube (auditory tube) on both sides in bright color (e.g. orange or red). Show clearly that each Eustachian tube extends from the middle ear (tympanic cavity) on each side of the head, running diagonally downward and inward to connect to the nasopharynx (back of the throat) at the center. Draw the tube as a clear line or tube shape with arrows showing the path from middle ear to nasopharynx. Label both ends: "Middle Ear" and "Nasopharynx (back of throat)". Clean medical diagram style, white background, frontal human face view.
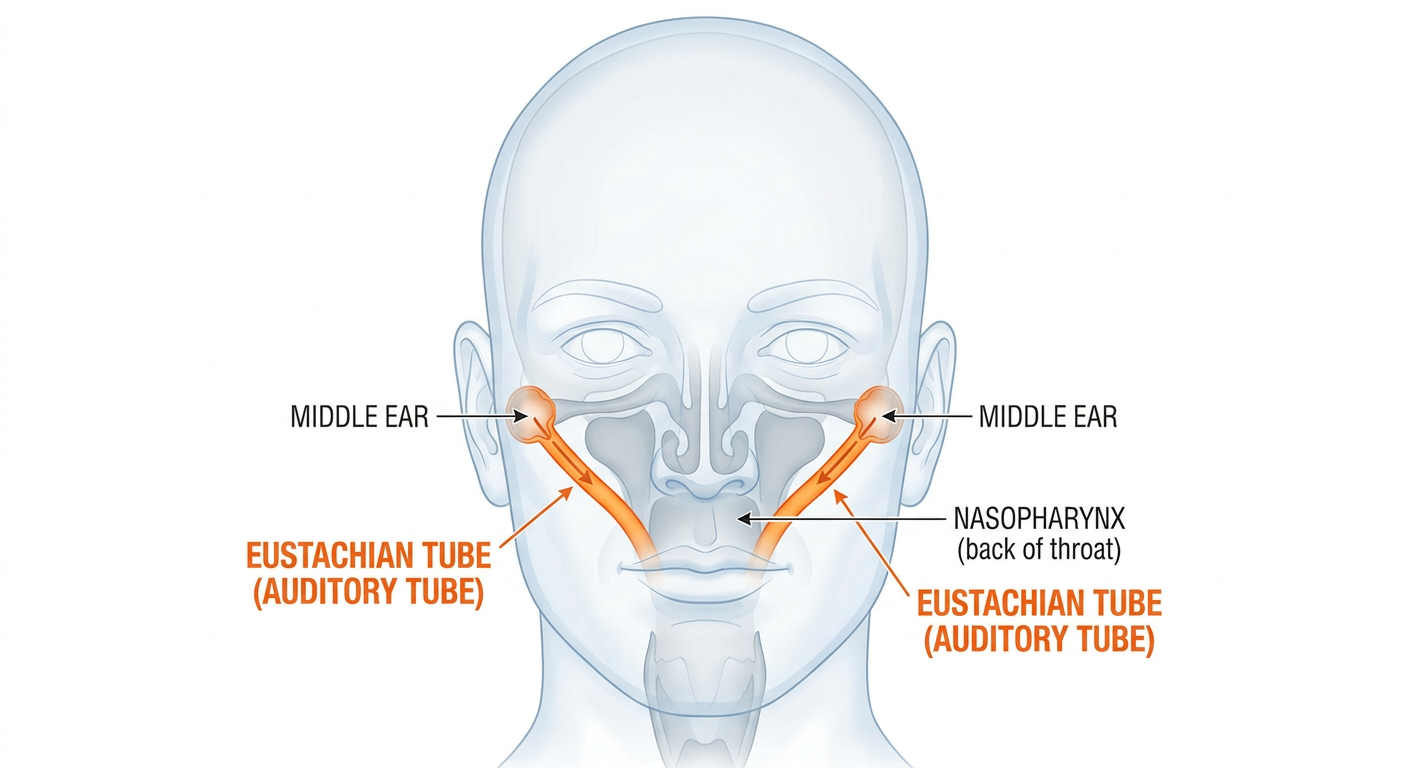
- Starts at: The middle ear (tympanic cavity) - located just behind each eardrum, on the left and right sides of the skull
- Ends at: The nasopharynx - the upper back of the throat, behind the nose, at the center
Oh, that's amazing. I, I really want this type of picture. Thank you. Yeah.
Uh, what is the lining up theme of skin? Skin, skin is.
The Lining (Epithelium) of Skin
1. Epidermis (the outer/surface layer)
| Layer | Description |
|---|---|
| Stratum Basale | Single layer of dividing (mitotic) basal cells - the "factory" layer |
| Stratum Spinosum | Several layers of larger keratinocytes joined by desmosomes |
| Stratum Granulosum | Flattened cells with keratohyalin granules; forms the waterproof barrier |
| Stratum Corneum | Most superficial - dead, flat cells filled with keratin (no nuclei); constantly shed |
- Melanocytes (5%) - produce melanin pigment for UV protection
- Langerhans cells (2-5%) - immune/antigen-presenting cells
- Merkel cells (6-10%) - touch/mechanoreceptor cells
2. Dermis (the deeper layer)
Why "keratinized"?
- Waterproof
- A barrier against infection
- Resistant to friction and abrasion
- Histology: A Text and Atlas, p. 1379
Myringotomy
Myringotomy
Indications
- Immediate relief of pain and pressure from acute otitis media (AOM)
- Chronic serous otitis media ("glue ear" / otitis media with effusion - OME) - to relieve conductive hearing loss or discomfort
- Placement of tympanostomy (ventilation) tubes
- Alternative for patients wishing to avoid antibiotics
Contraindications
- Known anomalous positioning of the jugular bulb (risk of vascular injury)
- Cochlear implant present
- Acute otitis externa (relative)
- Uncooperative patient (relative)
- Obscure landmarks - refer to otolaryngologist
Equipment
- Myringotomy knife (for the incision)
- Otoscope with operating head
- Local anesthesia: 8% tetracaine otic solution
- Aspiration equipment (vacuum pump + Juhn Tym-Tap aspirator or Baron suction tube) if drainage needed
- Papoose board for patient restraint if needed (children)
Procedure (Step by Step)
- Apply topical local anesthesia to the tympanic membrane (inject at cartilaginous-bony junction of external canal at multiple clock positions)
- Visualize the tympanic membrane with the otoscope
- Use the myringotomy knife to make a curved incision in the tympanic membrane (typically in the anteroinferior quadrant)
- If aspiration is needed - re-enter the incision with aspiration equipment before removing the speculum
- If tubes are being placed, insert the tympanostomy tube through the incision
- Do NOT irrigate the ear canal after myringotomy
Post-Procedure Care
- Purulent drainage may continue for up to 5 days
- Keep the ear dry for 5 days (when bathing/washing hair - use petroleum jelly-coated cotton plug)
- Topical antibiotic drops may be applied
- No peroxide rinse after myringotomy (unlike tympanocentesis)
Complications
| Complication | Note |
|---|---|
| Chronic perforation | If incision fails to heal |
| Jugular vein bulb puncture | If anomalous positioning present |
| Tympanic membrane scarring | |
| Hearing loss | If unrestricted needle traverse used |
| Otitis externa | Less serious complication |
Key Points
- Myringotomy alone heals quickly (the incision closes in days)
- When a tympanostomy tube is inserted, the opening is kept patent for weeks to months for continuous drainage and ventilation
- In adults with OME, the Valsalva manoeuvre and Toynbee manoeuvre are tried first before surgery
- CPT code: 69420 (myringotomy including aspiration and/or Eustachian tube inflation)
Uh, give me a photo of tegmentum tympani, uh, because, uh, from outside because it's a surgical landmark to invade the ear cavity. So, uh, from, I want to see from outside, uh, मतलब from outside, uh, the ear, uh, on which, from where the, um, from where we gave the incision to, uh, we gave the incision to invade the middle ear cavity.
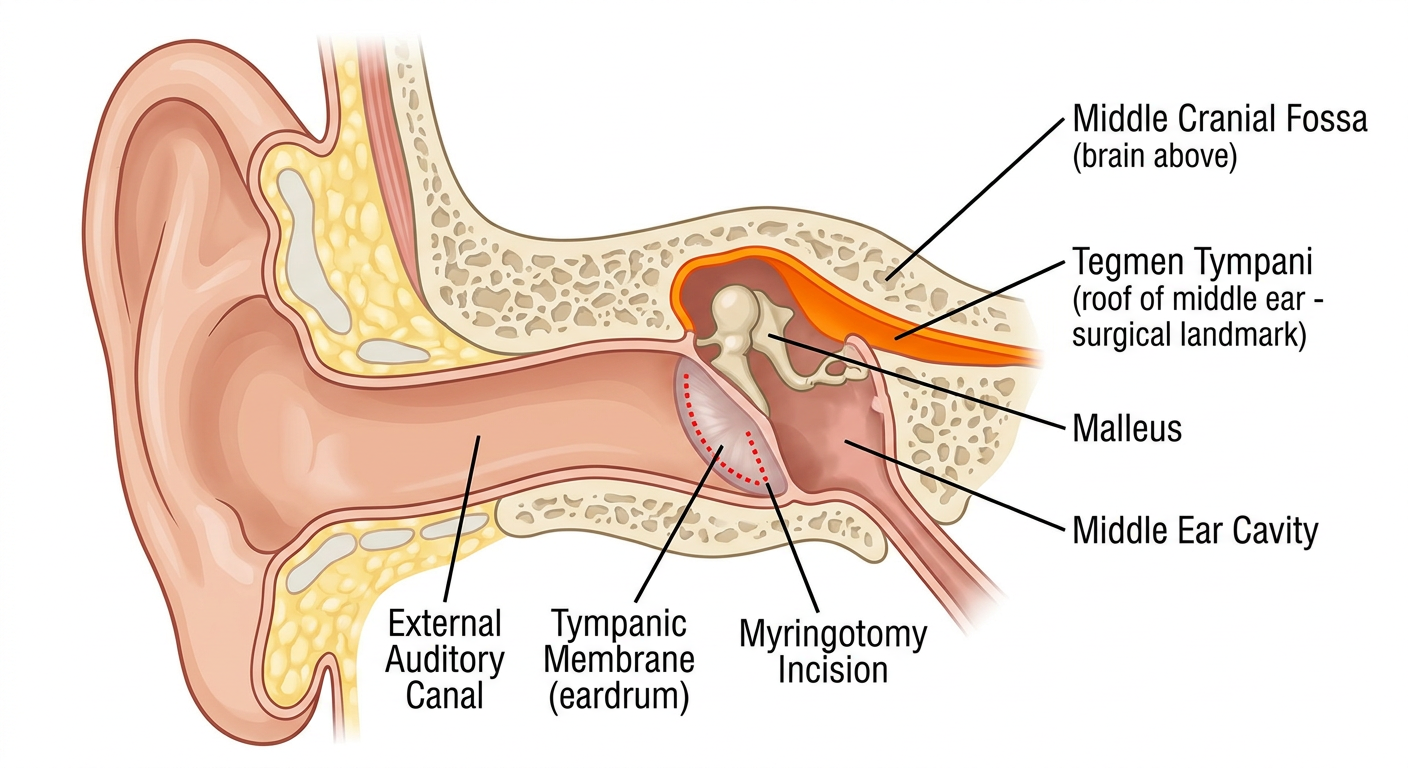
A surgical anatomical diagram showing the external view of the human ear as a surgeon sees it, from outside. Show a coronal cross-section cutaway of the ear from the front/outside perspective. Clearly label and highlight in bright orange the "Tegmen Tympani" - the thin bony roof/ceiling of the middle ear cavity, which is the superior wall separating the middle ear from the brain (middle cranial fossa). Show the external auditory canal leading inward to the tympanic membrane (eardrum). Show the middle ear cavity (tympanic cavity) below the tegmen tympani. Draw a red dotted incision line on the tympanic membrane showing where the surgical incision (myringotomy) is made to enter the middle ear cavity. Label all key structures: External Auditory Canal, Tympanic Membrane (eardrum), Tegmen Tympani (roof of middle ear - surgical landmark), Middle Ear Cavity, Malleus, and Middle Cranial Fossa (brain above). Clean medical illustration style, white background, clearly showing the tegmen tympani as the bony ceiling and the myringotomy incision site below it.
What is the Tegmen Tympani?
- Below: the middle ear (tympanic cavity)
- Above: the middle cranial fossa (where the brain sits)
Why is it a Surgical Landmark?
- Via the ear canal (Myringotomy route): The surgeon looks through the external auditory canal, sees the tympanic membrane, and makes the incision in the anteroinferior quadrant of the eardrum - well away from the tegmen tympani above
- Via mastoid approach: The tegmen tympani forms the superior limit of dissection - going above it risks entering the brain cavity
- A low-lying tegmen can block access and must be identified pre-operatively to avoid accidental breach during surgery (Scott-Brown's Otorhinolaryngology)
The Incision Site (from outside)
- Anteroinferior quadrant of the tympanic membrane (lower front portion)
- This is the safest zone - farthest from the tegmen tympani (above), the ossicles (center/upper), and the jugular bulb (below-posterior)
Secondary tympanic membrane
Secondary Tympanic Membrane
What it is
Location
- Sits on the medial wall of the middle ear cavity
- Closes off the lower end of the scala tympani (the lower canal of the cochlea)
- Sits just below the oval window (where the stapes footplate sits)
Its Role in Hearing (very important)
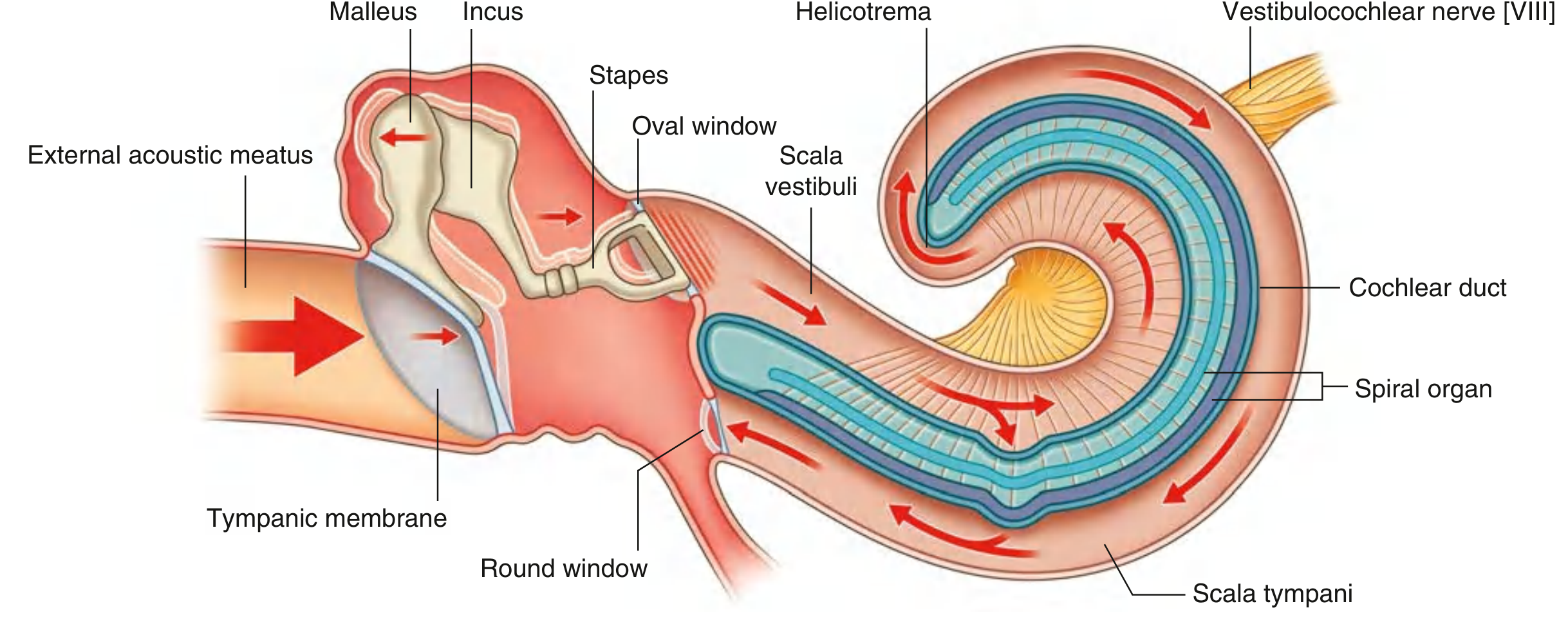
- Sound enters the external canal → strikes the primary tympanic membrane (eardrum)
- Eardrum vibrates → moves malleus → incus → stapes
- Stapes pushes inward on the oval window → creates a pressure wave in the perilymph of the scala vestibuli
- This pressure wave travels through the cochlea (through the helicotrema at the apex)
- The wave travels down the scala tympani and must be "released" - it causes the secondary tympanic membrane to bulge outward into the middle ear
- This outward bulging deflects the basilar membrane → stimulates the spiral organ (of Corti) → hearing impulses sent via vestibulocochlear nerve [VIII]
Key Point - Why it matters:
- The secondary tympanic membrane acts as a pressure relief valve for the incompressible cochlear fluid (perilymph)
- Without it, the fluid could not move and sound transmission through the cochlea would be impossible
- It moves in the opposite direction to the oval window at all times
Summary Table
| Feature | Detail |
|---|---|
| Also called | Round window membrane |
| Location | Covers the round window, medial wall of middle ear |
| Which canal | Closes off the scala tympani |
| Movement | Bulges outward when oval window moves inward |
| Function | Pressure relief - allows perilymph waves to travel through cochlea |
Mastoid antrum
Mastoid Antrum
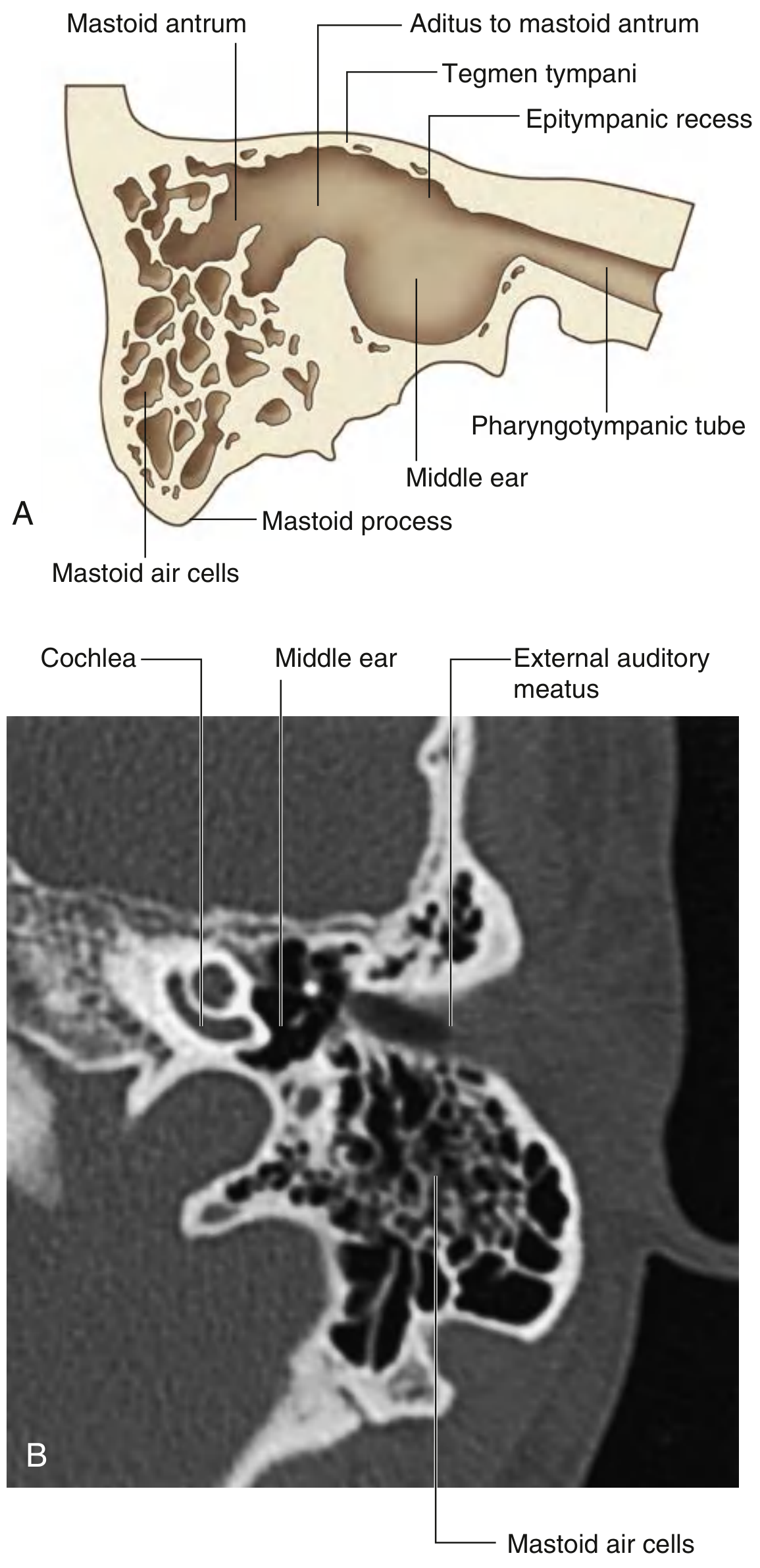
Diagram + CT Scan (Gray's Anatomy for Students)
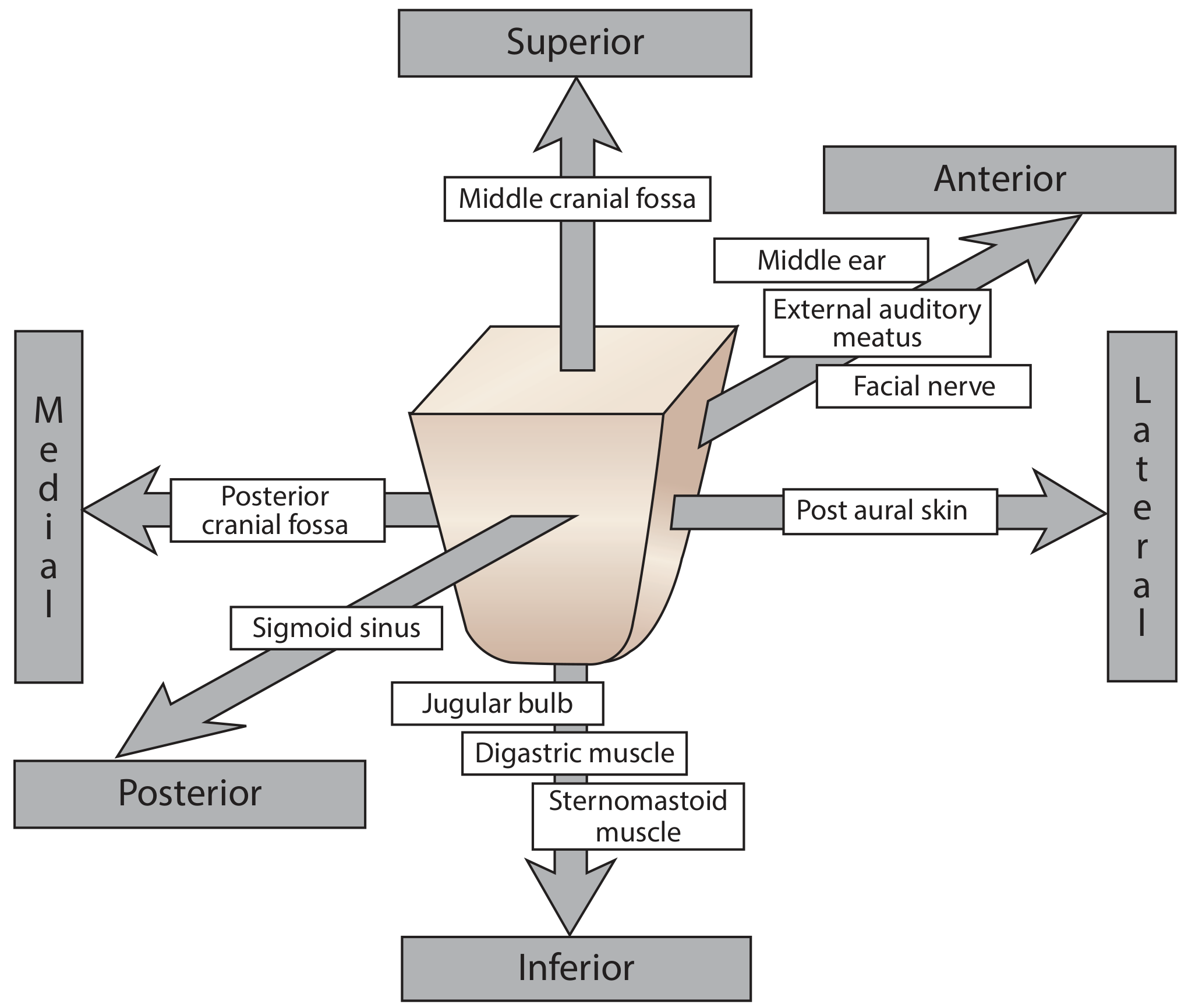
Relationships of the Mastoid Antrum (Scott-Brown's Otorhinolaryngology)
What is the Mastoid Antrum?
Key Anatomical Facts
Location & Connection
- Situated posterosuperior to the middle ear (tympanic cavity)
- Connects to the middle ear via the aditus to the mastoid antrum (aditus = opening/entrance)
- The aditus opens from the epitympanic recess (attic - the upper part of the middle ear)
- Lies in the petromastoid part of the temporal bone
Relations (from the diagram - all 6 directions)
| Direction | Relation |
|---|---|
| Superior | Middle cranial fossa (tegmen tympani - thin bony roof) |
| Inferior | Jugular bulb, Digastric muscle, Sternomastoid muscle |
| Anterior | Middle ear, External auditory meatus, Facial nerve |
| Posterior | Posterior cranial fossa, Sigmoid sinus |
| Medial | Posterior cranial fossa |
| Lateral | Post-aural skin (Macewen's triangle - surgical landmark) |
Macewen's Triangle - The Surgical Access Point
- A posterior prolongation of the line of the zygomatic arch
- A tangent passing through the posterior border of the external auditory meatus
Development (Embryology)
- The mastoid antrum forms during the late fetal period by expansion of the tympanic cavity
- It is almost adult size at birth
- No mastoid air cells are present in neonates - they only develop by age 5
- This is why mastoiditis presents differently in infants vs. older children
Lining
Clinical Significance
- Infection spreading from the middle ear → aditus → mastoid antrum = acute mastoiditis
- A low-lying tegmen (roof) may hinder surgical access from above
- An anteriorly placed sigmoid sinus (posterior) may complicate mastoid surgery
- A high-riding jugular bulb (inferiorly) is a vascular risk during surgery
What is air cell
What is an Air Cell? (in the Ear)
Simple Analogy
Imagine a sponge - it has many small holes filled with air. The mastoid bone is similar - its interior is filled with many small air-filled chambers (cells) all connected to each other.
The Mastoid Air Cell System - Hierarchy
Middle Ear (Tympanic Cavity)
↓ (via Aditus)
Mastoid Antrum ← LARGEST air cell (always present, even at birth)
↓
Mastoid Air Cells ← Many smaller cells branching off in all directions
- The mastoid tip (inferior)
- The retrofacial region (behind the facial nerve)
- The sinodural angle (between sigmoid sinus and dura)
- Anteriorly into the petrous apex and zygomatic arch
Lining of Air Cells
Development (Pneumatization)
- Mastoid antrum is present and nearly adult-sized at birth
- Mastoid air cells start developing after birth
- They are well developed by age 5
- Air cells grow as the mastoid process develops in early childhood
Types of Mastoid (based on air cells)
| Type | Description |
|---|---|
| Pneumatized | Well-developed, many air cells - normal |
| Diploic | Partially developed air cells, filled with spongy bone |
| Sclerotic (acellular) | No air cells - just the antrum remains; seen in ~20% of adults, associated with chronic ear disease |
Clinical Importance
- All mastoid air cells connect to the middle ear → infection in the middle ear can spread into them → mastoiditis
- Poor pneumatization (few air cells) + Eustachian tube dysfunction = predisposition to chronic otitis media (COM)
- Surgery (mastoidectomy) involves drilling out and removing these air cells to eliminate infection
caffeine is a cause of cancer?
caffeine coffee cancer risk
caffeine causes cancer IARC WHO classification 2024
Is Caffeine a Cause of Cancer?
What the WHO/IARC Says (Official Classification)
| Substance | IARC Group | Meaning |
|---|---|---|
| Coffee / Caffeine | Group 3 | "Not classifiable as to carcinogenicity" - no clear cancer link |
| Very hot beverages (>65°C) | Group 2A | "Probably carcinogenic" - but due to temperature, NOT caffeine itself |
Caffeine May Actually PROTECT Against Some Cancers
- Liver cancer - consistent protective effect across multiple studies
- Endometrial (uterine) cancer - reduced risk with higher coffee intake (Gao et al., 2022, PMID 35048465)
- Ovarian cancer - no increased risk; possibly reduced (Shafiei et al., 2019, PMID 30833443)
- Overall mortality - coffee drinkers tend to have lower all-cause mortality (Kim et al., 2019, PMID 31055709)
The One Exception - Very Hot Drinks
Bottom Line
| Question | Answer |
|---|---|
| Does caffeine cause cancer? | No |
| Does coffee cause cancer? | No (IARC Group 3) |
| Does very hot coffee/tea cause cancer? | Possibly - but it is the heat, not caffeine |
| Can coffee be protective? | Yes - for liver and endometrial cancer |