Treatment of interstitial lung disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
"interstitial lung disease" AND treatment
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Searching the Web
interstitial lung disease treatment guidelines 2025 antifibrotic nintedanib pirfenidone
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full answer.
Treatment of Interstitial Lung Disease (ILD)
ILD encompasses a large group of diffuse parenchymal lung disorders. Treatment is not uniform - it must be tailored to the specific ILD subtype, whether the process is predominantly inflammatory or fibrotic, and the underlying cause.
General Principles
Treatment should be individually tailored based on:
- The underlying rheumatic or systemic disease (if present)
- Whether the disease is predominantly inflammatory vs. fibrotic
- Radiographic extent and pattern (HRCT findings, particularly UIP vs. NSIP)
- Severity of pulmonary function impairment (FVC, DLCO)
- Rate of progression (FVC decline >10% over 6 months is a poor prognostic sign)
A multidisciplinary team approach - involving pulmonology, radiology, pathology, and rheumatology - improves diagnostic accuracy and management planning. - Washington Manual of Medical Therapeutics, p. 367; Rheumatology, 2-Volume Set (Elsevier)
ILD by Subtype: Specific Treatment Approaches
1. Idiopathic Pulmonary Fibrosis (IPF)
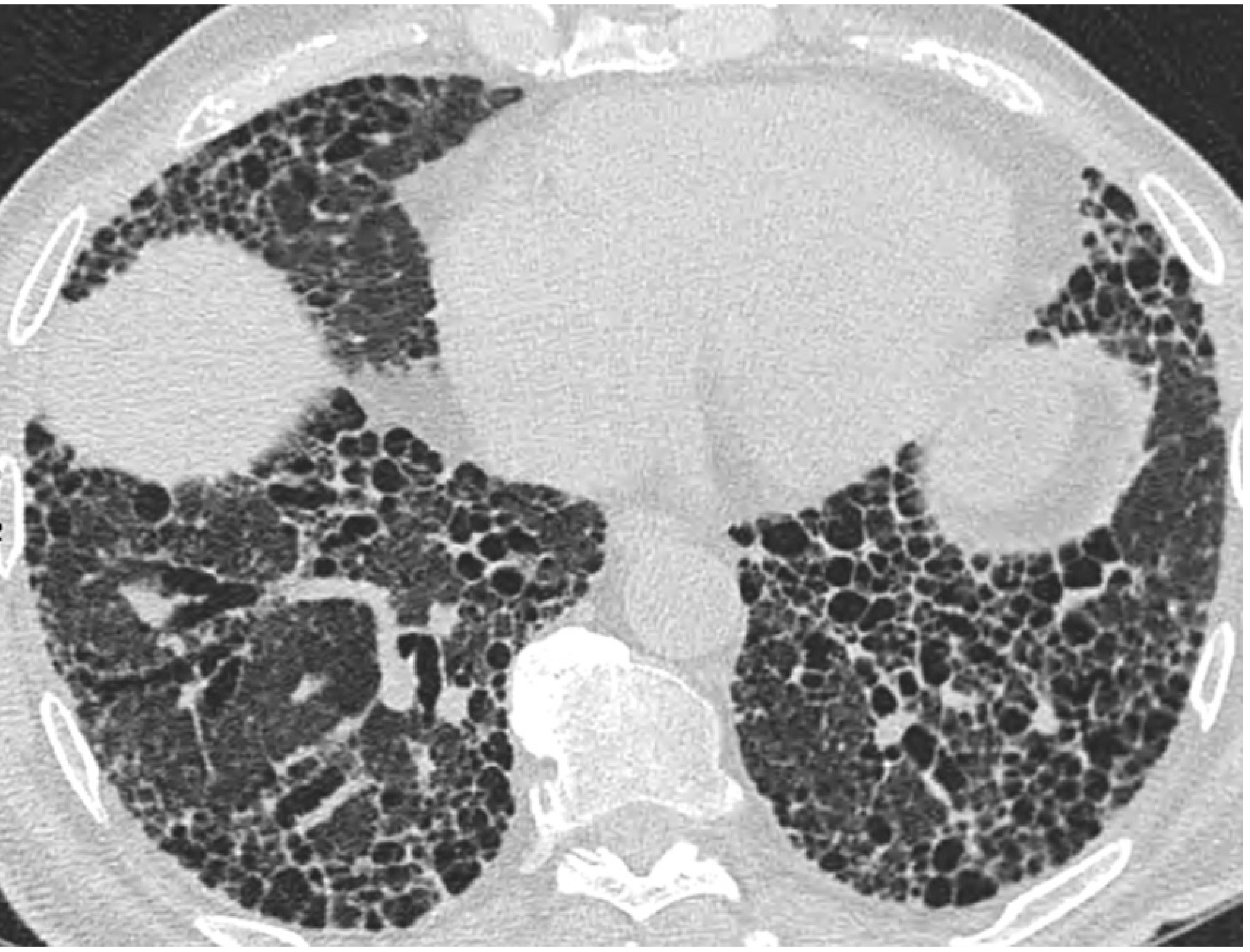
IPF is the most common idiopathic interstitial pneumonia and carries the worst prognosis. Radiographically, it shows a UIP pattern on HRCT (subpleural/basilar honeycombing + reticulation):
There is no medical cure for IPF. Disease-modifying options are limited:
| Drug | Mechanism | Key Side Effects |
|---|---|---|
| Pirfenidone | Antifibrotic (TGF-β inhibition) | Skin rash (~30%), photosensitivity, nausea, diarrhea |
| Nintedanib | Tyrosine kinase inhibitor (PDGF, VEGF, FGF receptors) | Diarrhea (~62%), nausea, vomiting, elevated LFTs |
Both agents slow the rate of FVC decline and may confer a mortality benefit. They are not used in combination. LFT monitoring is mandatory with both. - Washington Manual of Medical Therapeutics, p. 367-368
Important: The triple therapy combination of N-acetylcysteine + azathioprine + prednisone is harmful (increased risk of death and hospitalization) and must be avoided.
Acute exacerbations of IPF (acute worsening of dyspnea/oxygenation within 30 days with new ground-glass changes, excluding infection/PE/CHF) are treated with high-dose corticosteroids, though benefit is not proven. Mortality is high and patients often fail to return to baseline.
Lung transplantation is the ultimate therapy for advanced IPF. Patients should be referred to a transplant program at diagnosis. - Washington Manual of Medical Therapeutics, p. 368
Poor prognostic factors in IPF:
- FVC decline >10% over 6 months
- DLCO decline >15% over 6 months
- 6-minute walk distance decline >150 m over 12 months
- Median survival: mild (55.6 months), moderate (38.7 months), severe (27.4 months)
2. Connective Tissue Disease-Associated ILD (CTD-ILD)
CTD-ILD includes ILD in the setting of SSc, RA, polymyositis/dermatomyositis, Sjögren's, SLE, and antisynthetase syndrome. These typically show an NSIP pattern (more responsive to treatment) though a UIP pattern may also occur.
For predominantly inflammatory disease:
- Corticosteroids (first-line)
- Mycophenolate mofetil (MMF) - preferred maintenance agent (better tolerability than cyclophosphamide)
- Azathioprine
- Rituximab - especially in refractory inflammatory ILD
- Calcineurin inhibitors
- Cyclophosphamide (IV monthly or oral for 6-12 months) for severe disease, then transition to MMF or azathioprine
For predominantly fibrotic disease:
-
Antifibrotic therapy (nintedanib) is appropriate based on emerging evidence from recent trials
-
Rheumatology, 2-Volume Set (Elsevier), p. 2903
SSc-Associated ILD (SSc-ILD)
SSc-ILD is the leading cause of death in systemic sclerosis. The algorithm below guides management:
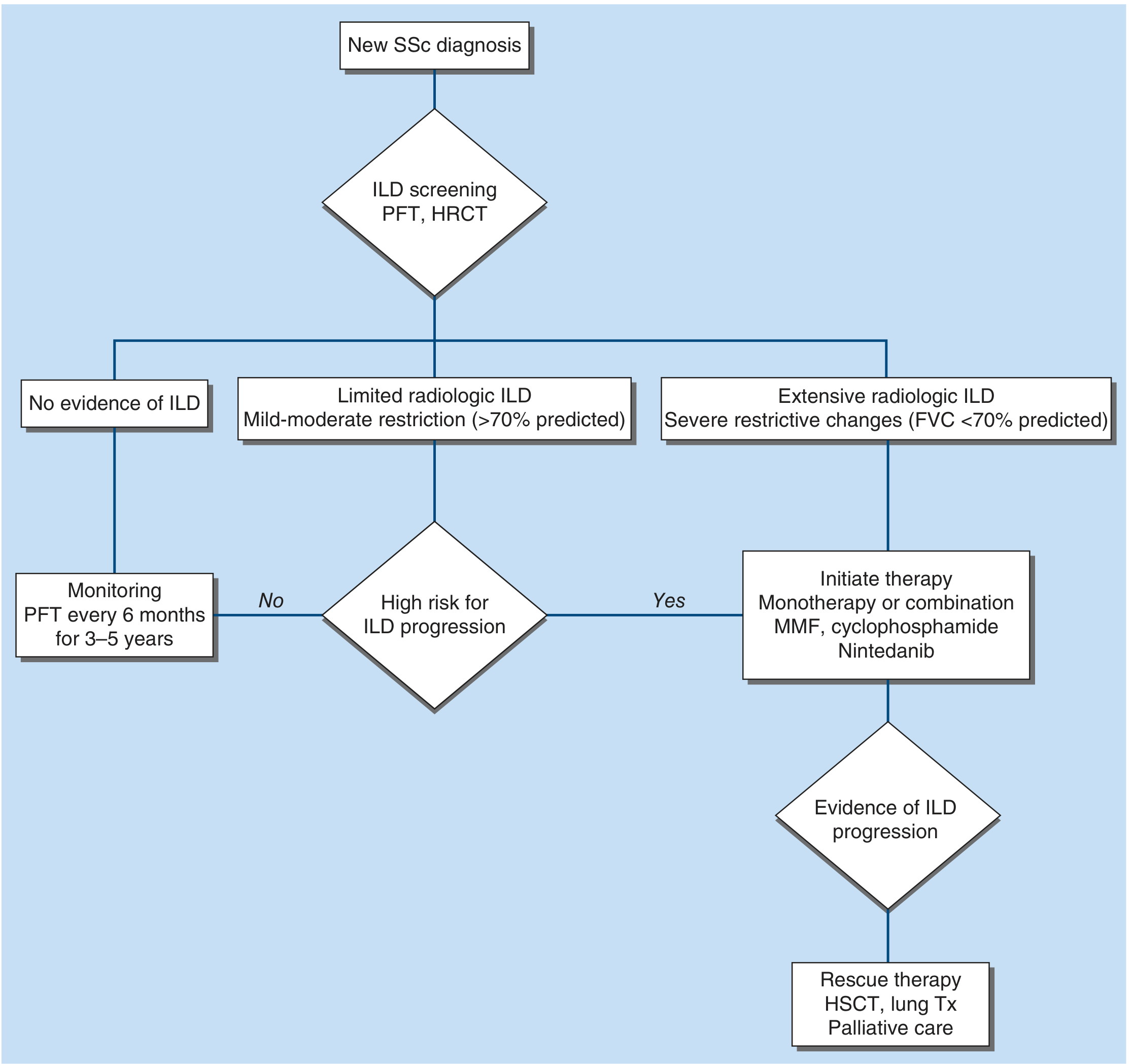
Key points for SSc-ILD:
-
Baseline HRCT + PFTs every 3-6 months in high-risk patients (male sex, older age, anti-topoisomerase I positivity, progressive skin involvement)
-
MMF is generally preferred over cyclophosphamide due to fewer side effects; both slow FVC decline
-
Nintedanib may be added if ILD progresses despite immunotherapy (FDA-approved for SSc-ILD)
-
Tocilizumab has been FDA-approved for early SSc-ILD
-
HSCT is a consideration in refractory cases with good performance status
-
Lung transplantation for continued progression despite medical therapy
-
Harrison's Principles of Internal Medicine 22E, p. 2915
3. ANCA-Associated ILD (MPO-ANCA ± MPA)
-
Active MPA + ILD: Standard remission induction - glucocorticoids + cyclophosphamide or rituximab
-
MPO-ANCA + NSIP/bronchiolitis pattern without vasculitis: Glucocorticoids + azathioprine or MMF
-
UIP pattern + MPO-ANCA without vasculitis: Do NOT give immunosuppressives (increases mortality); treat with antifibrotic therapy instead
-
Fishman's Pulmonary Diseases and Disorders, p. 3046
4. Specific ILD Subtypes - Treatment Summary
| ILD Type | Primary Treatment |
|---|---|
| Drug-induced ILD | Discontinue culprit medication; corticosteroids |
| Sarcoidosis | Corticosteroids; methotrexate, azathioprine, infliximab for refractory cases |
| Hypersensitivity pneumonitis (HP) | Antigen avoidance; corticosteroids (limited benefit); antifibrotic therapy if fibrotic |
| DIP / RB-ILD | Smoking cessation; corticosteroids (limited benefit) |
| NSIP (CTD-associated) | Corticosteroids + immunosuppressives (MMF, azathioprine, rituximab) |
| COP | Corticosteroids (often dramatic response) |
| IPF | Pirfenidone or nintedanib; lung transplant |
| Progressive fibrosing ILD (non-IPF) | Nintedanib (INBUILD trial data) |
- Washington Manual of Medical Therapeutics, p. 367
5. Supportive & General Measures (All ILD)
- Oxygen supplementation for hypoxia
- Pulmonary rehabilitation - improves 6-minute walk distance and quality of life in IPF
- Pneumocystis jirovecii pneumonia (PJP) prophylaxis in all patients on corticosteroid-based regimens
- Vaccination against influenza and pneumococcal pneumonia
- Treatment of co-existing pulmonary hypertension (bosentan, sildenafil, riociguat)
- GERD management (proton pump inhibitors) - aspiration may drive ILD progression
- Early lung transplant evaluation in patients with progressive disease, poor response to therapy, and good performance status
6. Progressive Fibrosing ILD (PF-ILD)
An increasingly recognized category of non-IPF ILDs that behave like IPF (progressive despite treatment). Nintedanib was approved for PF-ILD based on the INBUILD trial, which showed slowing of FVC decline. This category includes fibrotic HP, fibrotic NSIP, RA-ILD, and others showing a self-sustaining fibrotic progression. A 2025 study on nerandomilast (a PDE4B inhibitor) suggests a new class of antifibrotics may offer a better GI side-effect profile than nintedanib. - RheumNow 2025 Antifibrotics review
Recent Evidence (2024-2026)
- PMID 39721758 (Thorax, 2025): Systematic review on corticosteroid therapy for acute exacerbation of ILD - evidence remains limited; high-dose steroids are widely used but not definitively proven effective.
- Real-world studies from 2025 show nintedanib has a 4-fold higher rate of dose reduction vs. pirfenidone due to GI side effects, though both demonstrate similar progression-free survival in IPF.
- Current guidelines (2025) require FVC ≥50% predicted and DLCO 30-79% for nintedanib/pirfenidone authorization in IPF.
Sources: Harrison's Principles of Internal Medicine 22E (2025), Washington Manual of Medical Therapeutics, Fishman's Pulmonary Diseases and Disorders, Rheumatology 2-Volume Set (Elsevier 2022)
This is a shared conversation. Sign in to Orris to start your own chat.