Chemosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Here is the full answer:
Chemosis
Chemosis is edema (fluid accumulation) of the bulbar conjunctiva, producing a translucent, gelatinous swelling that can protrude through the eyelids. The word comes from Greek cheme (gaping) + osis (condition).
Moderate chemosis in acute allergic conjunctivitis (Kanski's):
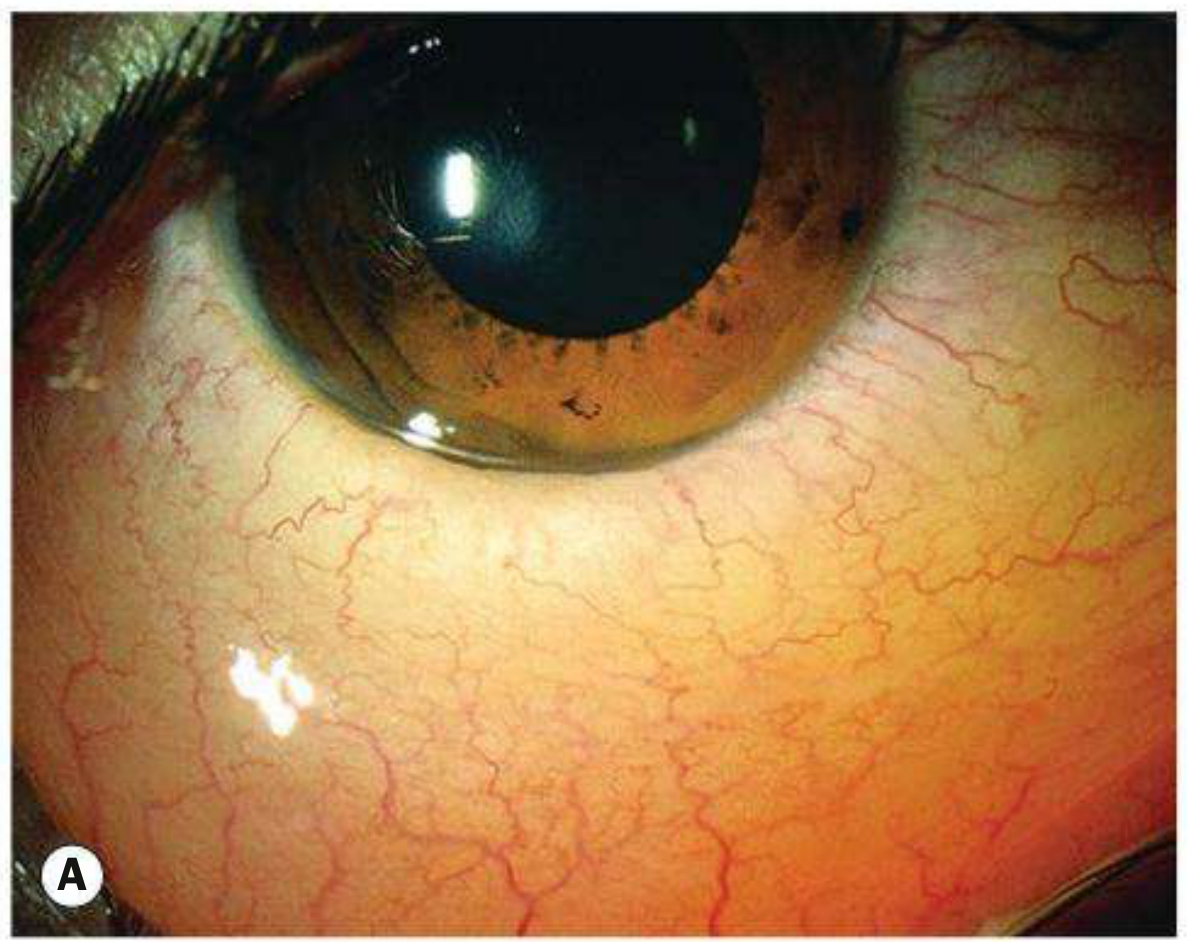
Chemosis visible from below (Kanski's, Fig. 6.2C):

Pathophysiology
Chemosis results from increased fluid in the subconjunctival space due to one or more of the following mechanisms:
| Mechanism | Example |
|---|---|
| Increased vascular permeability | Hypersensitivity (IgE-mediated), infection |
| Increased venous pressure | Carotid-cavernous fistula (CCF), SVC syndrome, right heart failure |
| Decreased plasma oncotic pressure | Nephrotic syndrome, hypoalbuminemia |
| Local inflammation/venous obstruction | Orbital disease, post-surgical |
Causes
Acute Chemosis
- Allergic (most common) - acute pollen exposure (type I hypersensitivity); hallmark of acute allergic conjunctivitis in children, frequently dramatic; resolves within hours as vascular permeability normalizes
- Severe infective conjunctivitis - bacterial or viral
- Angioneurotic edema (hereditary or acquired C1-esterase inhibitor deficiency)
Subacute / Chronic Chemosis
Local causes:
- Thyroid eye disease (Graves' orbitopathy)
- Chronic allergic conjunctivitis
- Ocular or eyelid surgery (post-operative)
- Trauma
- Carotid-cavernous fistula (CCF) - chemosis + proptosis + red eye + pulsating exophthalmos + bruit; arterialized conjunctival vessels are the hallmark
Systemic causes:
- Increased systemic vascular permeability: allergic conditions, meningitis, vasculitis
- Increased venous pressure: SVC syndrome, right-sided heart failure
- Decreased plasma oncotic pressure: nephrotic syndrome, hypoalbuminemia
- Drugs (e.g., topical eye drops)
- Venous congestion (e.g., carotid-cavernous fistula)
- Myxedema
Clinical Features
- Appearance: Translucent, boggy, jelly-like swelling of the bulbar conjunctiva; may herniate between the eyelids
- Symptoms: Usually asymptomatic unless severe; foreign body sensation, red eye; itching and watering in allergic cases
- Associated signs (depending on cause): proptosis, lid edema, conjunctival injection, restricted eye movements, bruit (CCF)
Key Associations to Remember
| Cause | Key Distinguishing Feature |
|---|---|
| Acute allergy (pollen) | Children, spring/summer, dramatic chemosis, resolves in hours |
| Carotid-cavernous fistula | Proptosis + chemosis + arterialized (corkscrew) vessels + pulsatile exophthalmos |
| Thyroid eye disease | Lid lag, lid retraction, restrictive myopathy, bilateral |
| Nephrotic syndrome | Bilateral periorbital edema + generalized edema, low albumin |
| SVC syndrome | Facial/neck edema, collateral veins on chest |
| Gonorrheal conjunctivitis | Hyper-acute purulent discharge, preauricular lymphadenopathy |
Management
Treatment is directed at the underlying cause:
- Acute allergic: Cool compresses; resolves spontaneously; topical adrenaline 0.1% (a single drop) can reduce extreme chemosis; antihistamine drops for seasonal/perennial forms
- Infective: Appropriate antimicrobial therapy
- Post-surgical: Lubricant eye drops, time; severe cases may need temporary tarsorrhaphy
- CCF: Endovascular embolization
- Systemic disease: Treat the underlying condition (e.g., diuretics for heart failure, immunosuppression for nephrotic syndrome)
Sources: Kanski's Clinical Ophthalmology, 10th ed.; The Wills Eye Manual; Localization in Clinical Neurology, 8th ed.
Blepharitis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from both Kanski's and Wills Eye Manual. Here is the full structured answer:
Blepharitis
Blepharitis is chronic inflammation of the eyelid margins. It is one of the most common ocular conditions, causing persistent discomfort and irritation with a characteristic pattern of remissions and exacerbations. There is a well-known poor correlation between symptom severity and objective signs.
Classification
Blepharitis is divided into anterior and posterior forms, with considerable overlap ("mixed blepharitis"):
| Feature | Anterior Blepharitis | Posterior Blepharitis |
|---|---|---|
| Location | Base of eyelashes, anterior lid margin | Meibomian glands, posterior lid margin |
| Subtypes | Staphylococcal, Seborrhoeic | Meibomian gland dysfunction (MGD) |
| Key deposit | Hard scales / collarettes (Staph); soft greasy scales (Seb) | Oily/turbid/toothpaste-like meibomian secretion |
| Lash changes | Madarosis, trichiasis, poliosis (more marked) | Mild lash changes |
| Cysts | Hordeolum (stye) | Chalazion (meibomian cyst) |
| Corneal signs | Punctate erosions, infiltrates, vascularization | More pronounced - punctate erosions, infiltrates |
| Tear film | Mild instability | Foamy, unstable - dry eye more marked |
| Associated skin disease | Staphylococcal: atopic dermatitis; Seborrhoeic: seborrhoeic dermatitis | Acne rosacea |
Pathophysiology
Anterior - Staphylococcal
An abnormal cell-mediated immune response to S. aureus cell wall components produces lid inflammation. This is more common and severe in atopic dermatitis patients. Bacterial toxins directly damage the ocular surface.
Anterior - Seborrhoeic
Strongly associated with generalized seborrhoeic dermatitis (scalp, nasolabial folds, retroauricular skin, sternum).
Posterior - Meibomian Gland Dysfunction (MGD)
Bacterial lipases (from S. aureus and others) break down meibum triglycerides into free fatty acids (FFAs). FFAs:
- Raise the melting point of meibum → inspissation, gland plugging
- Promote S. aureus growth
- Disrupt the lipid layer of the tear film → increased tear evaporation and osmolarity → unstable tear film and dry eye
Demodex
- Demodex folliculorum longus - anterior blepharitis
- Demodex folliculorum brevis - posterior blepharitis
Collarettes (cylindrical collections of keratin, waste, mite eggs around lash bases) are considered pathognomonic of Demodex infestation.
Clinical Features
Symptoms
- Burning, grittiness, mild photophobia, crusting of lid margins
- Symptoms worse in the morning (vs. dry eye alone which worsens through the day)
- Stinging may be more prominent in posterior disease
- Contact lens intolerance
- Usually bilateral and symmetrical, no visual disturbance
Signs - Anterior (Staphylococcal)
Blepharitis with lash collarettes (Wills Eye Fig. 5.8.1):

- Hard scales and crusting at the base of lashes
- Collarettes (cylindrical collections around lash bases) - pathognomonic
- Mild papillary conjunctivitis, chronic conjunctival hyperaemia
- Long-standing: scarring/notching of lid margin, madarosis (lash loss), trichiasis, poliosis (white lashes)
Signs - Anterior (Seborrhoeic)
- Hyperaemic, greasy anterior lid margins
- Soft scales; lashes stuck together
Signs - Posterior (MGD)
Meibomitis with inspissated meibomian glands (Wills Eye Fig. 5.8.2):
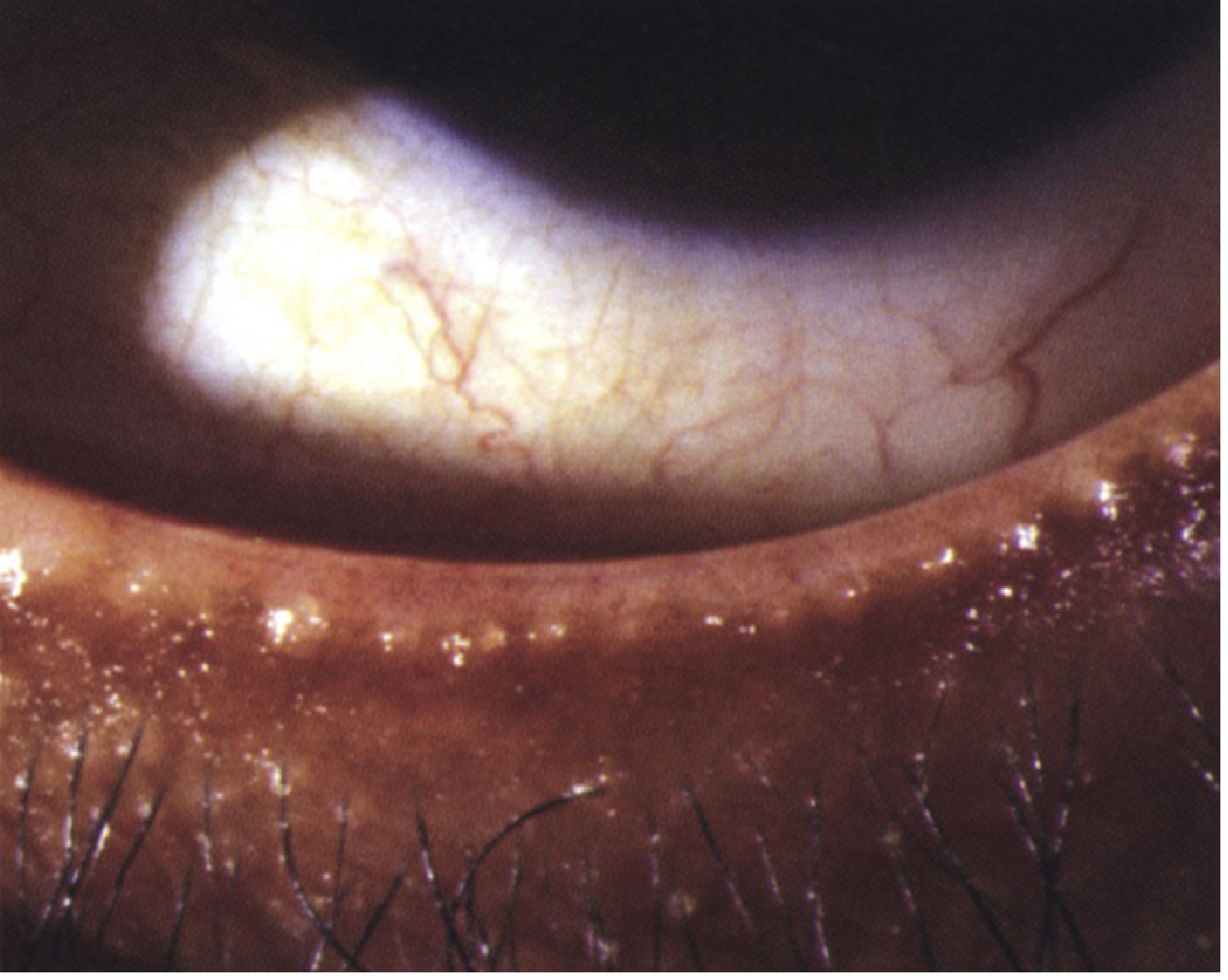
- Capping of meibomian gland orifices with oil globules
- Pouting, recession, or plugging of gland orifices
- Hyperaemia and telangiectasis of the posterior lid margin
- Expression of turbid or toothpaste-like meibomian secretion on pressure
- Lid transillumination: gland loss and cystic ductal dilatation
- Oily, foamy, unstable tear film; froth at lid margins and inner canthi
Complications / Associated Conditions
- Dry eye syndrome (all types, most severe in posterior)
- Corneal changes: superficial punctate keratopathy (SPK), peripheral infiltrates, vascularization (pannus), phlyctenules
- Chalazion / hordeolum
- Atopic keratoconjunctivitis (in patients with atopic dermatitis)
- Acne rosacea (posterior)
- Blepharokeratoconjunctivitis (chronic progression)
Red flag: Intractable, unilateral, or asymmetric blepharitis (especially upper vs. lower eyelid asymmetry) is a rare but important presentation of sebaceous cell carcinoma of the eyelid - requires appropriate clinical workup. - Wills Eye Manual
Angular Blepharitis
- Involves the canthal area (medial or lateral angle)
- Caused by Moraxella lacunata (most common) or S. aureus
- Associated with angular conjunctivitis
- Treatment: topical tetracycline or chloramphenicol
Treatment
Step-by-step (Wills Eye Manual)
- Eyelid hygiene (cornerstone) - lid margin scrubs twice daily with commercial eyelid scrub or dilute baby shampoo on a washcloth
- Warm compresses - 5-10 minutes, 2-4 times daily (softens inspissated meibum)
- Artificial tears - preservative-free, 4-8 times/day if dry eye component
- Topical antibiotics - erythromycin ointment or azithromycin gel-drop to lid margins at bedtime (moderately severe disease)
- Oral tetracyclines - doxycycline 100 mg twice daily (unresponsive cases, rosacea); azithromycin 500 mg/day x 3 days for 3 cycles with 7-day intervals is an alternative
- Omega-3 supplementation - improves meibomian gland function
- Cyclosporine 0.05%/0.09% or lifitegrast 5% drops twice daily for the inflammatory/dry eye component
- Demodex-directed therapy - tea-tree oil lid scrubs or hypochlorous acid lid cleansing agent for minimum 6 weeks if collarettes present and prior treatment failed
- Advanced meibomian gland treatments - thermal pulsation + expression, intense pulsed light (IPL), microblepharoexfoliation, meibomian gland probing
Note: Tetracycline derivatives (doxycycline) are contraindicated in pregnancy, breastfeeding, and children ≤8 years. Use erythromycin 200 mg twice daily as an alternative. - Wills Eye Manual
Follow-up
Review at 2-4 weeks. Lid hygiene and warm compresses may be reduced to once daily as the condition improves but are typically needed indefinitely - blepharitis is rarely cured, only controlled.
Sources: Kanski's Clinical Ophthalmology, 10th ed.; The Wills Eye Manual, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.