Heart failure approach
Reading File
Finding Sources
Searching PubMed
"heart failure" management guidelines
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
I now have all the material needed for a comprehensive answer. Here is the full Heart Failure approach:
Heart Failure - Clinical Approach
Definition
Heart failure (HF) is a clinical syndrome in which the heart cannot meet the metabolic requirements of the body at normal filling pressures. It is not synonymous with congestive HF - pulmonary congestion may be absent; patients may present with dyspnea and reduced exercise capacity without overt fluid overload. The preferred term is simply "heart failure."
Classification
By Ejection Fraction
| Type | EF | Mechanism |
|---|---|---|
| HFrEF (HF with reduced EF) | < 45-50% | Impaired LV contraction (systolic dysfunction) |
| HFpEF (HF with preserved EF) | > 45-50% | Impaired LV filling/relaxation (diastolic dysfunction) |
HFpEF is nearly as common as HFrEF and carries similar morbidity.
NYHA Functional Classification
| Class | Symptoms |
|---|---|
| I | No symptoms with ordinary activity |
| II | Slight limitation - comfortable at rest, symptomatic with moderate exertion |
| III | Marked limitation - comfortable at rest, symptomatic with minimal exertion |
| IV | Symptoms at rest |
ACC/AHA Staging (A-D)
- Stage A: High risk, no structural disease, no symptoms
- Stage B: Structural disease, no symptoms (e.g., asymptomatic LV dysfunction post-MI)
- Stage C: Structural disease + prior or current symptoms
- Stage D: Refractory HF requiring advanced/specialized interventions
Etiology & Precipitants
Common causes of LV remodeling:
- Coronary artery disease / myocardial infarction (most common in developed countries)
- Hypertension
- Valvular heart disease
- Diabetes mellitus
- Cardiomyopathy (dilated, hypertrophic, restrictive)
- Congenital heart disease
- Alcohol, anemia, thyroid disease
High-output precipitants (CO > 4 L/min/m²): hyperthyroidism, Paget disease, AV fistula, severe anemia
Common decompensation triggers: dietary sodium/fluid non-compliance, medication non-adherence, infection, arrhythmia (especially new AF), ACS, uncontrolled hypertension, NSAID use.
Pathophysiology
The modern model centers on LV remodeling (stretching and dilation → reduced function), driven by neurohormonal activation regardless of the initial insult:
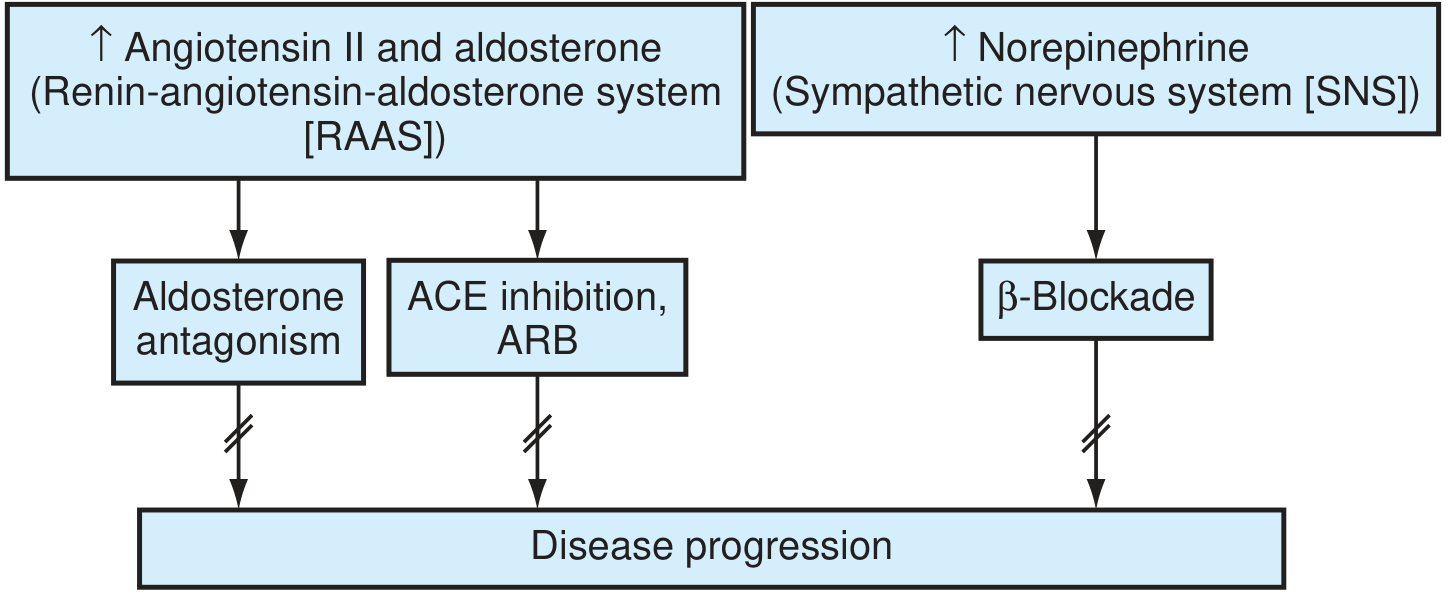
The two key axes: RAAS (Angiotensin II + Aldosterone) and SNS (Norepinephrine) - pharmacotherapy targets both to halt disease progression.
Key mechanisms:
- Angiotensin II: promotes myocyte apoptosis, hypertrophy, ventricular fibrosis, and aldosterone release
- Aldosterone: augments RAAS harmful effects, promotes adverse remodeling; "escapes" ACE inhibition over time - hence MRA needed in addition to ACEi/ARB
- Catecholamines (SNS): downregulate β-adrenoreceptors, directly toxic via cAMP-dependent calcium overload, increase MVO2, precipitate arrhythmias, induce LVH
- Cellular: increased MMPs → fibrosis and collagen deposition; altered calcium flux; metabolic shift to glycolysis
Clinical Features
Symptoms
- Left-sided: dyspnea on exertion, orthopnea, paroxysmal nocturnal dyspnea (PND), fatigue, reduced exercise tolerance
- Right-sided: peripheral edema, ascites, RUQ discomfort (hepatic congestion), early satiety, weight gain
Signs
- Elevated JVP, hepatojugular reflux
- S3 gallop (ventricular filling sound - classic for systolic HF)
- S4 gallop (atrial kick into stiff ventricle - suggests diastolic dysfunction)
- Displaced point of maximal impulse (PMI) - cardiomegaly
- Bibasilar crackles, pleural effusion (typically right > left)
- Pitting pedal/ankle edema, ascites
- Cool extremities, narrow pulse pressure (low output states)
- Cheyne-Stokes respiration (in severe HF)
Workup
Initial Investigations
| Test | Finding/Purpose |
|---|---|
| ECG | LVH, prior MI (Q waves), arrhythmia (AF), bundle branch block, ischemia |
| Chest X-ray | Cardiomegaly (CTR > 0.5), pulmonary venous congestion, Kerley B lines, bat-wing edema, pleural effusion |
| BNP / NT-proBNP | Key biomarker - elevated in HF; helps distinguish cardiac vs. non-cardiac dyspnea; guides therapy titration |
| Echocardiogram | Defines EF (HFrEF vs HFpEF), regional wall motion abnormalities, valvular disease, pericardial effusion - most important diagnostic test |
| CBC | Anemia (high-output HF, worsening HF) |
| BMP/CMP | Renal function (baseline before ACEi/diuretics), electrolytes, liver function |
| Thyroid function | Exclude hypo/hyperthyroidism |
| Lipids, fasting glucose | Cardiovascular risk |
| Urinalysis | Exclude renal disease |
Additional Studies (selected patients)
- Cardiac MRI: tissue characterization, infiltrative disease, myocarditis, sarcoidosis
- Cardiac catheterization: CAD assessment when revascularization is a consideration; hemodynamic evaluation
- Nuclear stress test/stress echo: myocardial viability, ischemia
- Holter/ambulatory monitor: arrhythmia screening
- Endomyocardial biopsy: suspected myocarditis, specific cardiomyopathies (per AHA/ACC/ESC guidance)
Management
General Principles
- Treat underlying cause
- Address precipitants
- Reduce symptoms
- Slow disease progression
- Reduce hospitalizations and mortality
Non-Pharmacologic
- Sodium restriction: < 2 g/day (evidence mixed for strict restriction, but reasonable in symptomatic HF)
- Fluid restriction: ~1.5-2 L/day in moderate-severe HF
- Daily weight monitoring: patient weighs every morning; seek care if weight gain > 2 lbs/day or 5 lbs/week
- Exercise: cardiac rehabilitation in stable HF - improves functional capacity and quality of life
- Alcohol abstinence (especially alcoholic cardiomyopathy)
- Smoking cessation
- Vaccination: influenza annually, pneumococcal
Pharmacotherapy - HFrEF (Evidence-Based)
The "four pillars" of disease-modifying therapy in HFrEF:
1. ACE Inhibitor (or ARB if intolerant)
- Mechanism: blocks RAAS, reduces Ang II-mediated apoptosis and fibrosis, lowers preload and afterload
- Evidence: Reduces mortality and hospitalization (CONSENSUS, SOLVD, TRACE trials)
- Agents: enalapril, lisinopril, ramipril, captopril
- Dose: titrate to target doses used in trials
- ARBs (e.g., valsartan, losartan): use when ACEi not tolerated due to cough; do NOT combine ACEi + ARB (increased adverse effects without benefit)
- ARNI (sacubitril/valsartan, Entresto): superior to enalapril in reducing CV death and HF hospitalization (PARADIGM-HF trial) - preferred over ACEi in patients who can tolerate and afford it (Class I recommendation)
2. Beta-Blocker
- Mechanism: blocks SNS toxicity, prevents catecholamine-induced myocyte damage, reduces arrhythmia risk, improves LV remodeling
- Evidence: Three agents proven to reduce mortality: carvedilol (COPERNICUS, US Carvedilol), metoprolol succinate (MERIT-HF), bisoprolol (CIBIS-II)
- Important: Start at low dose in stable (not acutely decompensated) HF and titrate up slowly
- Note: Carvedilol preferred in HF with diabetes (neutral metabolic effects vs. metoprolol per GEMINI trial)
3. Mineralocorticoid Receptor Antagonist (MRA)
- Mechanism: aldosterone "escapes" ACEi suppression - selective blockade is needed; reduces fibrosis and adverse remodeling
- Evidence: Spironolactone (RALES trial) - 30% mortality reduction in NYHA III-IV HFrEF; Eplerenone (EMPHASIS-HF) - reduced mortality and hospitalization in NYHA II HFrEF
- Monitoring: watch for hyperkalemia and renal impairment; avoid if K+ > 5.0 or GFR < 30
- Agents: spironolactone 25-50 mg/day; eplerenone 25-50 mg/day
4. SGLT2 Inhibitor
- Mechanism: reduces HF hospitalizations and CV death through cardiorenal mechanisms independent of glycemic effect
- Evidence: dapagliflozin (DAPA-HF) and empagliflozin (EMPEROR-Reduced) - significant reduction in HF hospitalizations and CV death in HFrEF, regardless of diabetes status
- Agents: dapagliflozin 10 mg/day, empagliflozin 10 mg/day
- Now Class I recommendation in HFrEF
Diuretics (Symptom Control)
- Loop diuretics (furosemide, torsemide, bumetanide): first-line for fluid overload/congestion; no proven mortality benefit but essential for symptom relief
- Torsemide has more predictable bioavailability than furosemide
- Titrate to achieve euvolemia (target: JVP normal, no peripheral edema, no orthopnea)
- Monitor electrolytes and renal function
Other Agents
| Drug | Indication |
|---|---|
| Hydralazine + Isosorbide dinitrate | Class I in Black patients with HFrEF on ACEi/ARB + beta-blocker; also use when ACEi/ARB/ARNI not tolerated (e.g., renal failure) |
| Ivabradine | HR > 70 bpm in sinus rhythm despite max beta-blocker; reduces HF hospitalization |
| Digoxin | Rate control in HF + AF; reduces HF hospitalization but no mortality benefit; narrow therapeutic window |
| Vericiguat | NYHA II-IV HFrEF who had recent HF event; reduces CV death/HF hospitalization |
HFpEF Management
- No proven mortality-reducing pharmacotherapy (contrast with HFrEF)
- Control heart rate and blood pressure aggressively
- Diuretics for congestion/fluid overload
- Treat underlying causes: hypertension, coronary disease, AF, obesity, sleep apnea
- SGLT2 inhibitors (empagliflozin - EMPEROR-Preserved trial): reduced HF hospitalizations in HFpEF - Class IIa
Device Therapy
| Device | Indication |
|---|---|
| ICD (Implantable Cardioverter-Defibrillator) | EF ≤ 35% despite ≥ 3 months GDMT, NYHA Class II-III; expected survival > 1 year |
| CRT (Cardiac Resynchronization Therapy) | EF ≤ 35% + LBBB with QRS ≥ 150 ms + NYHA II-IV; improves EF, symptoms, survival |
| CRT-D | Combination CRT + defibrillator |
| LVAD (Left Ventricular Assist Device) | NYHA IV refractory HF - bridge to transplant or destination therapy |
| Heart transplantation | End-stage HF refractory to maximal therapy |
Acute Decompensated HF (ADHF)
"LMNOP" mnemonic:
- Lasix (furosemide IV) - aggressive diuresis
- Morphine (use cautiously; reduces preload, anxiolytic - not routinely recommended)
- Nitrates (IV nitroglycerin or nitroprusside for hypertensive HF; powerful preload/afterload reduction)
- Oxygen / NIV (supplemental O2 to maintain SaO2 > 94%; CPAP/BiPAP reduces intubation need)
- Positioning (sit upright)
Additional ADHF management:
- Identify and treat precipitant
- Vasopressors/inotropes (dobutamine, dopamine, milrinone) in cardiogenic shock or low output state
- Avoid negative inotropes, NSAIDs
- Ultrafiltration for diuretic-refractory congestion
- Consider hemodynamic monitoring (Swan-Ganz) in refractory cases
Monitoring
- BNP/NT-proBNP: trending down indicates effective therapy; rising signals decompensation
- Renal function and electrolytes: monitor 1-2 weeks after ACEi/ARB/MRA initiation or dose change
- Echocardiogram: reassess EF after 3-6 months of optimal medical therapy (EF may recover)
- Weight monitoring: patient self-monitoring daily
Prognosis
- Mortality remains ~50% at 5 years from diagnosis
- 1-month rehospitalization rate ~25%
- Poor prognostic markers: low EF, elevated BNP, low sodium, worsening renal function, NYHA class IV, cardiac cachexia, inability to tolerate GDMT
Sources: Textbook of Family Medicine 9e, pp. 689-738; Braunwald's Heart Disease, 2-Volume Set (Cardiovascular Medicine)
This is a shared conversation. Sign in to Orris to start your own chat.