ecmo
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of Extracorporeal Membrane Oxygenation (ECMO):
ECMO — Overview
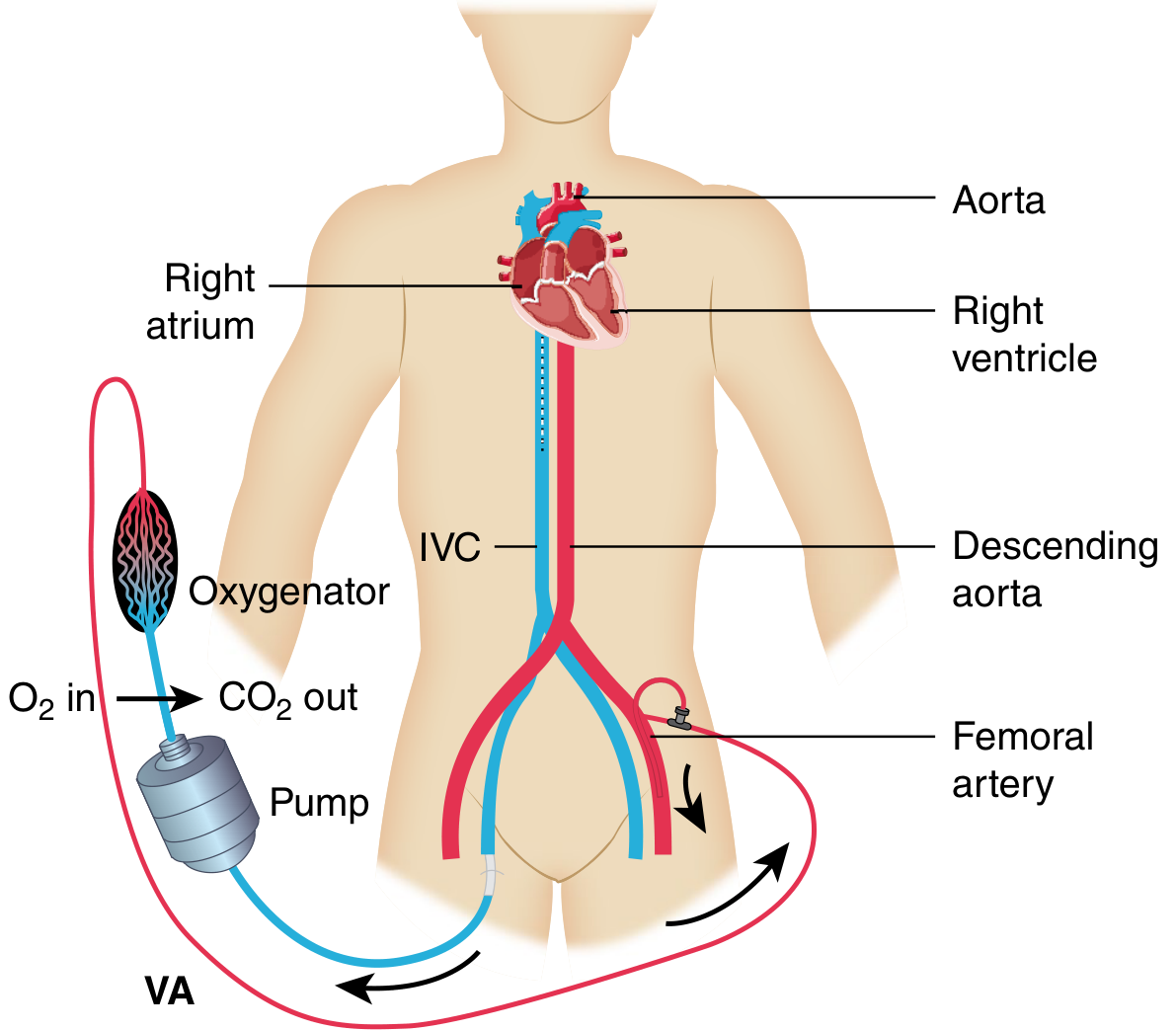
ECMO provides mechanical cardiorespiratory support to patients with severe cardiac and/or pulmonary failure when conventional therapies are exhausted. It works by draining venous blood, passing it through an oxygenator (artificial lung), and returning oxygenated blood to the patient.
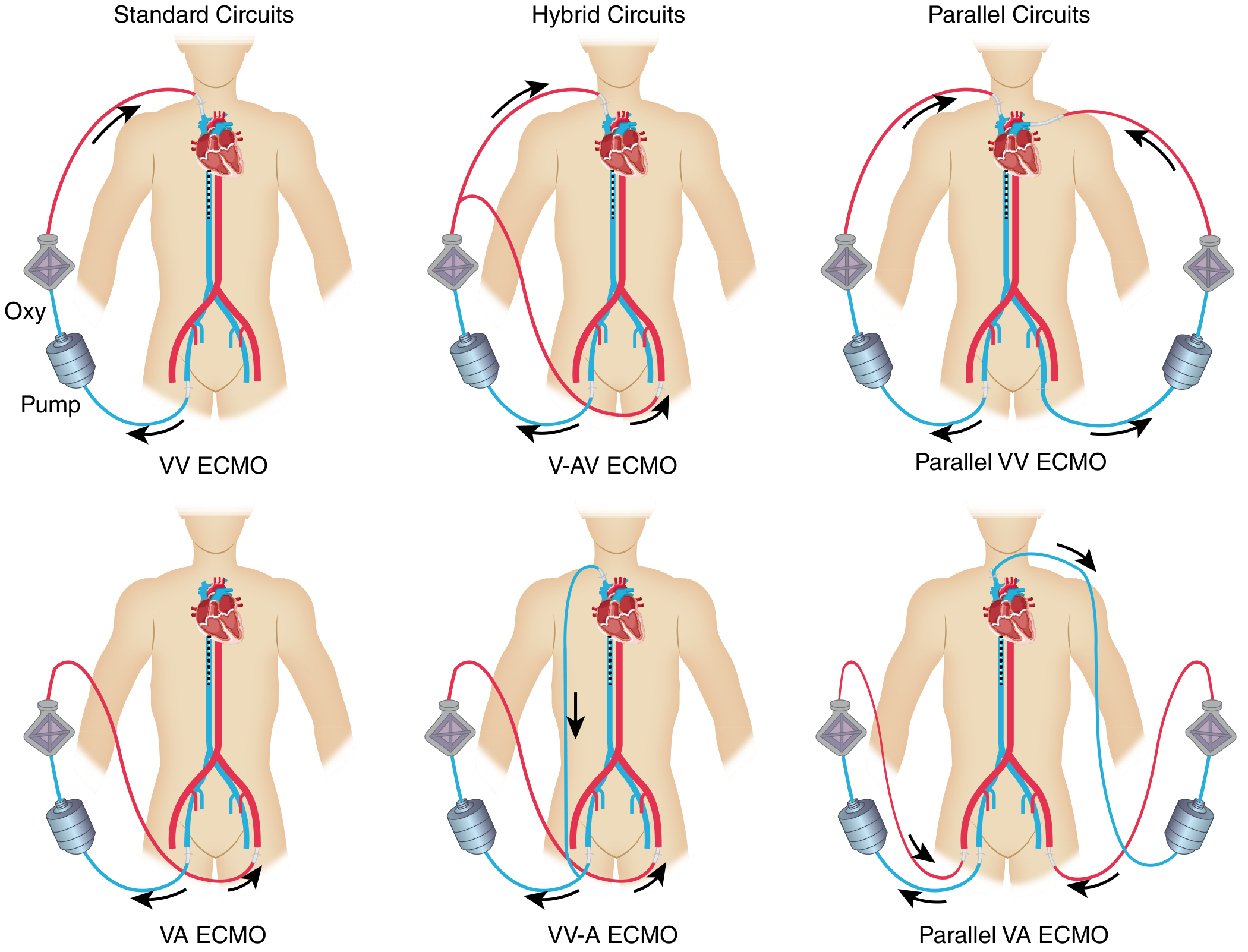
Configurations
| Mode | Full Name | Primary Support |
|---|---|---|
| VV ECMO | Venovenous | Respiratory only (gas exchange); requires intact cardiac function |
| VA ECMO | Venoarterial | Cardiac + respiratory; used in cardiogenic shock |
| V-AV ECMO | Veno-arteriovenous | Hybrid; flexible transitions between circulatory and respiratory support |
Brief History
- 1953 — John Gibbon develops the heart-lung machine
- 1972 — First successful cardiac ECMO use (2-year-old, cardiac failure post-Mustard procedure); J.D. Hill reports first prolonged ECMO in an adult ICU patient
- 1975 — Robert Bartlett (the "father of modern ECMO") saves a neonate with meconium aspiration
- 2009 — H1N1 pandemic triggers major expansion of adult ECMO for ARDS
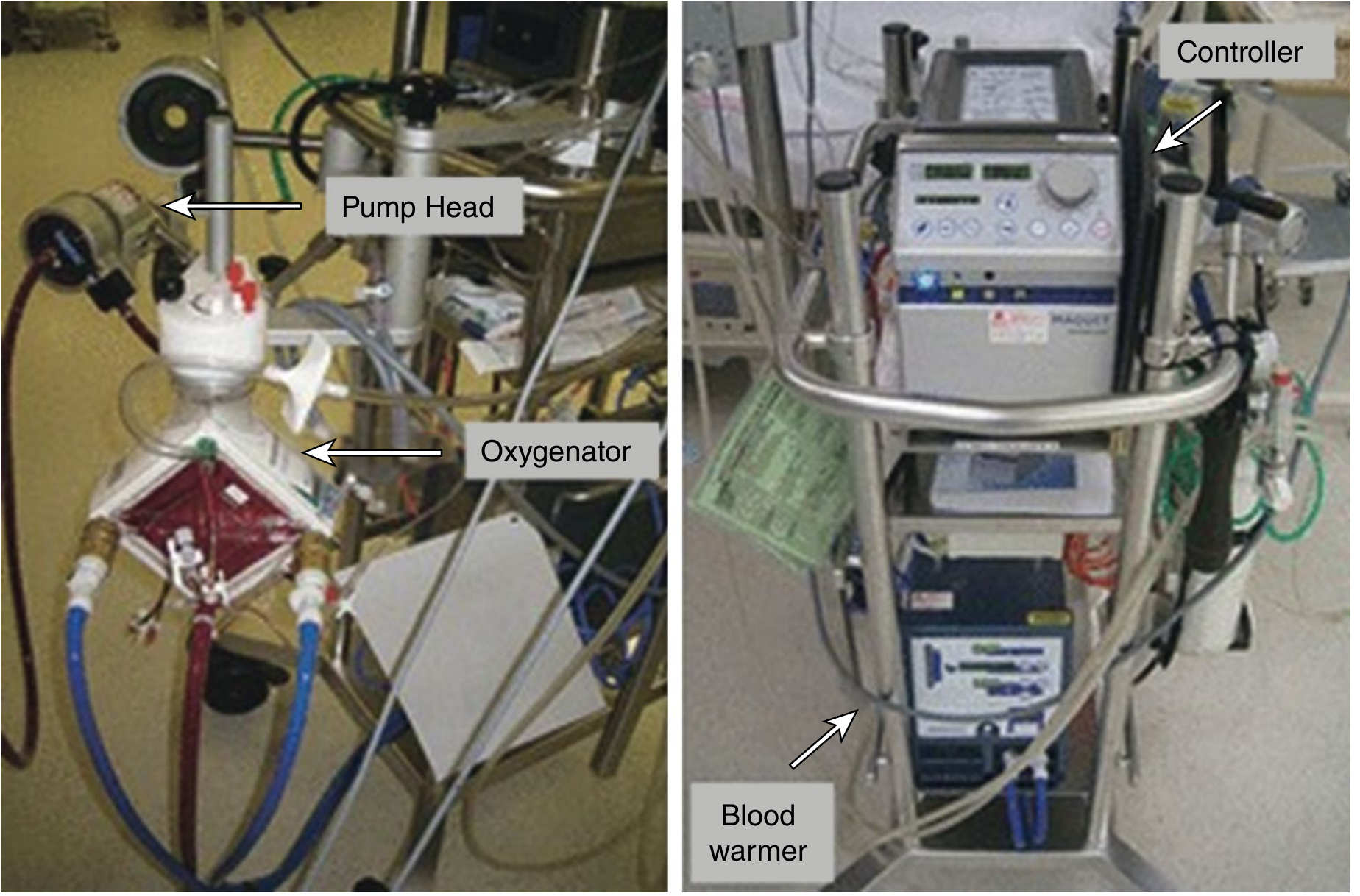
- Technology shift: roller pumps → centrifugal pumps; silicone membranes → polymethylpentene (PMP) oxygenators; open surgical cannulation → percutaneous bedside approach
Indications
VV ECMO (Respiratory Failure)
- Severe ARDS (PaO₂/FiO₂ < 100 mmHg with PEEP > 5 cm H₂O) — ~40% mortality without ECMO
- Viral/bacterial pneumonia (H1N1, COVID-19), bridge to lung transplant
- Murray score and Berlin criteria guide candidacy
VA ECMO (Cardiac Failure)
- Cardiogenic shock refractory to dual inotropes ± IABP/Impella
- Postcardiotomy failure (inability to wean from bypass)
- Acute MI with mechanical complications (VSR, acute MR, RV failure)
- Fulminant myocarditis (~67% survival), peripartum cardiomyopathy
- Massive pulmonary embolism with obstructive shock
- Refractory ventricular arrhythmias
- ECPR (CPR-ECMO) — ~29% survival to discharge in adults
- High-risk PCI support
Key Management Points
Respiratory (VV ECMO)
- Lung-protective ventilation: low tidal volume, PEEP ~10 cm H₂O, RR 10, FiO₂ 40%
- Sweep gas adjusted to keep PCO₂ 35–45 mmHg, pH 7.35–7.45
- Prone positioning can be performed concurrently
- Steroids (DEXA-ARDS/Meduri protocols) often continued
Cardiac (VA ECMO)
- Inotropes maintain LV pulsatility and aortic valve opening:
- Dobutamine (β₁ agonist, reduces afterload)
- Milrinone (PDE-3 inhibitor — preferred for RV failure/pulmonary HTN)
- Epinephrine (severe shock requiring strong inotropy)
- Loss of pulsatility → LV distention → pulmonary congestion, aortic root thrombus, coronary malperfusion
- Inhaled nitric oxide for RV failure/pulmonary hypertension
Anticoagulation
- Systemic heparin (institution-specific PTT/anti-Xa goals)
- May be withheld short-term in high bleeding risk (especially VV)
- HIT → switch to argatroban or bivalirudin
- Flow > 4 L/min reduces thrombosis risk
Cannulation
| Type | Sites | Notes |
|---|---|---|
| Peripheral | Femoral vein/artery, internal jugular | Percutaneous, bedside; limits mobility if femoral |
| Central | Direct aorta/RA via sternotomy or axillary | Post-cardiac surgery; requires OR skill |
Complications
| Complication | Details |
|---|---|
| Bleeding | Most common; from anticoagulation + cannula sites |
| Hemolysis | Mechanical shear; monitor LDH, free Hgb, transmembrane pressures |
| Infection | Cannula-site and circuit infections |
| Extremity ischemia | Femoral artery cannulation → distal limb ischemia; prevent with antegrade distal perfusion cannula |
| Stroke/CVA | Thromboembolism or hemorrhage from altered coagulation |
| DVT | Immobility + vascular trauma; duplex at 24h post-decannulation |
| Low flow / chugging | Hypovolemia, cannula malposition, or circuit thrombosis |
| Spinal cord ischemia | Rare; turbulent mixing zone in peripheral VA ECMO |
| LV distention (VA ECMO) | Retrograde flow impedes LV emptying → may need Impella or atrial septostomy |
Outcomes (ELSO Registry)
- Adult respiratory failure (VV ECMO): ~60% survival to discharge
- Adult cardiac failure (VA ECMO): varies by indication; myocarditis ~67%, postcardiotomy ~30%, ECPR ~29%
- Bridge to transplant/LVAD: 45–66% survive to discharge
Key Trials
- CESAR trial: 63% vs. 47% survival (ECMO vs. standard care) for severe ARDS — supported use at specialized centers
- EOLIA trial: No statistically significant mortality difference (35% vs. 46%, P = .09) but 28% crossover to ECMO; widely interpreted as supporting early ECMO in severe ARDS
Sources: Sabiston Textbook of Surgery, 20e; Miller's Anesthesia, 10e; Fishman's Pulmonary Diseases and Disorders
This is a shared conversation. Sign in to Orris to start your own chat.