Explain in detail about thoracic duct
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative textbooks. Let me compile the complete, detailed answer.
The Thoracic Duct
The thoracic duct is the largest lymphatic vessel in the body and the principal channel through which lymph from most of the body is returned to the venous system. Here is a detailed account covering its anatomy, course, tributaries, embryology, histology, and clinical significance.
1. Overview and Dimensions
The thoracic duct measures 38 to 45 cm in length and 2 to 5 mm in diameter. It drains lymph from roughly three-quarters of the body - specifically everything except the right upper extremity, right side of the head and neck, right half of the thorax, and right lung. Those regions are drained by the right lymphatic duct.
- Fischer's Mastery of Surgery, p. 2442
- Gray's Anatomy for Students, p. 270
2. Origin - Cisterna Chyli
The thoracic duct begins at the cisterna chyli (chyle cistern), a saccular dilation located in the retrocrural abdomen between L1 and L2 vertebral levels. It lies dorsal to the aorta and to the right of the midline.
The cisterna chyli receives:
- Right and left lumbar trunks (draining the lower limbs, pelvic organs, and abdominal walls)
- Intestinal trunks (draining the gut and unpaired abdominal viscera)
Not all individuals have a discrete cisterna chyli - in some people it is represented by a convergence plexus rather than a single sac.
- Gray's Anatomy for Students, p. 270
- The Developing Human: Clinically Oriented Embryology, p. 885
3. Course and Relations
The thoracic duct travels through three anatomical regions:
A. Abdomen (below diaphragm)
- Arises from the cisterna chyli at L1-L2
- Lies between the aorta (left) and the azygos vein (right)
B. Posterior Mediastinum (T12 to T4/5)
The thoracic duct enters the chest through the aortic hiatus of the diaphragm at T12 and ascends through the posterior mediastinum to the right of midline, lying:
- Left: thoracic aorta
- Right: azygos vein
- Anterior: esophagus
- Posterior: bodies of thoracic vertebrae
At approximately T4-T5, the duct crosses to the left of midline and enters the superior mediastinum.
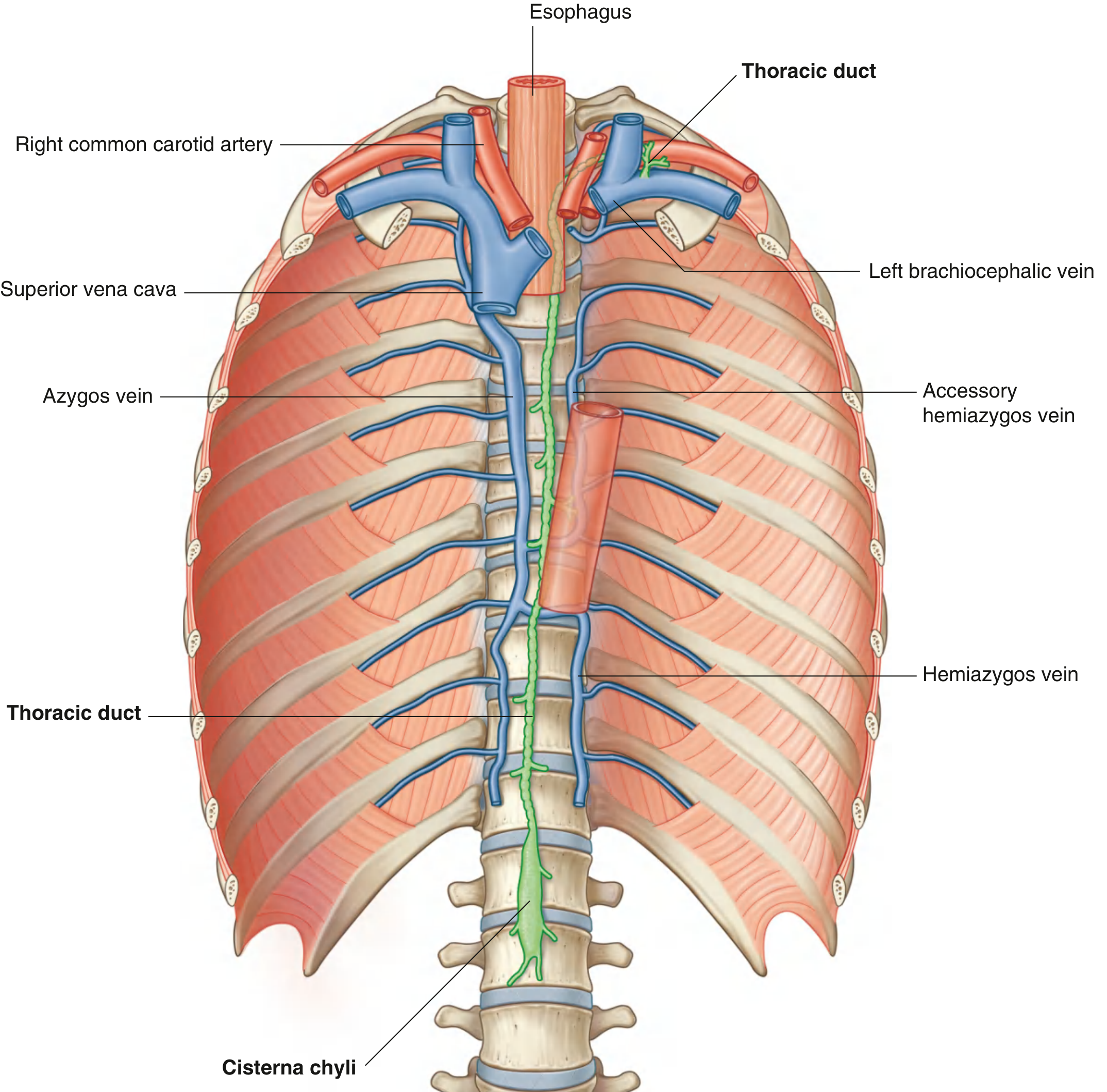
Fig. 3.106 from Gray's Anatomy for Students - Thoracic Duct in the posterior mediastinum
C. Superior Mediastinum and Neck
After crossing to the left at T4-T5, the duct:
-
Passes posterior to the arch of the aorta and the initial portion of the left subclavian artery
-
Lies between the esophagus and the left mediastinal pleura
-
Enters the root of the neck to the left of the esophagus
-
Arches laterally in the neck, passing posterior to the carotid sheath
-
Turns inferiorly in front of the thyrocervical trunk, phrenic nerve, and vertebral artery
-
Gray's Anatomy for Students, p. 1176-1177
4. Termination
The thoracic duct terminates by emptying into the junction of the left internal jugular vein and the left subclavian vein (the left venous angle / left brachiocephalic vein).
Just before emptying, it is joined by three tributaries:
- Left jugular trunk - drains left side of the head and neck
- Left subclavian trunk - drains the left upper limb
- Left bronchomediastinal trunk (occasionally) - drains the left half of thoracic structures
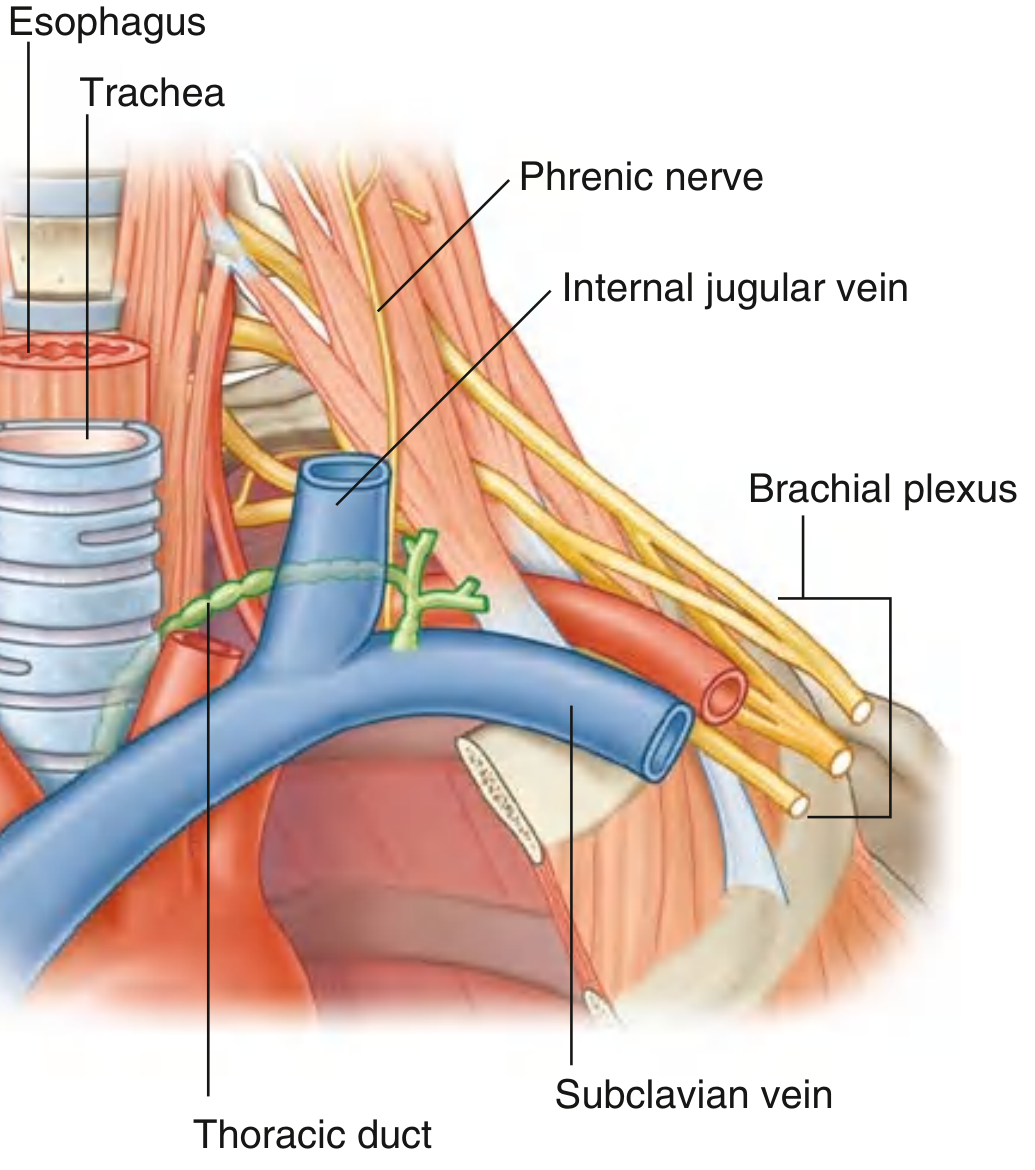
Fig. 8.198 from Gray's Anatomy for Students - Thoracic Duct in the root of the neck
5. Right Lymphatic Duct (Counterpart)
On the right side, a parallel but smaller system drains:
- Right jugular trunk (right head and neck)
- Right subclavian trunk (right upper limb)
- Right bronchomediastinal trunk (right thorax + right upper intercostal spaces)
These may unite into a single right lymphatic duct or enter the right venous angle as three separate trunks. There is significant variability.
- Gray's Anatomy for Students, p. 1177
6. Tributaries in the Thorax
Within the thorax, the thoracic duct also receives:
-
Descending thoracic lymph trunks from the lower 6-7 intercostal spaces on both sides
-
Upper intercostal trunks from the upper left 5-6 intercostal spaces
-
Ducts from posterior mediastinal nodes
-
Ducts from posterior diaphragmatic nodes
-
Gray's Anatomy for Students, p. 270
-
Color Atlas of Human Anatomy Vol. 2, p. 148
7. Embryological Development
The lymphatic system develops from six primary lymph sacs in the embryo:
- Two jugular lymph sacs (near the internal jugular-subclavian junction)
- Two iliac lymph sacs
- One retroperitoneal lymph sac (in the mesenteric root)
- One cisterna chyli (dorsal to the retroperitoneal sac)
Initially, both a right and left thoracic duct are present, connecting the jugular lymph sacs to the cisterna chyli. An anastomosis then forms between these two channels. The definitive thoracic duct is formed from:
- The caudal part of the right thoracic duct
- The anastomosis between the right and left ducts
- The cranial part of the left thoracic duct
This explains why there are many anatomical variations in the origin, course, and termination of the thoracic duct. The right lymphatic duct derives from the cranial part of the right thoracic duct.
- The Developing Human: Clinically Oriented Embryology, p. 885
- Langman's Medical Embryology
8. Histological Structure
Like all lymphatic vessels, the thoracic duct has three layers:
- Tunica intima: endothelium with bicuspid valves (numerous, to prevent backflow of lymph)
- Tunica media: smooth muscle (thicker than in peripheral lymphatics, enabling active peristalsis)
- Tunica adventitia: loose connective tissue
The valves give the duct a beaded appearance on lymphangiography. Flow is maintained by:
- Smooth muscle peristalsis
- Respiratory movements (thoracic pressure changes)
- Arterial pulsations from adjacent vessels
- Skeletal muscle contractions
9. Physiology and Function
- Drains approximately 2-4 liters of lymph per day into the venous system
- Carries chylomicrons (dietary fat absorbed in the gut via lacteals) - the thoracic duct is the main route for fat transport from the intestine to the bloodstream
- Returns proteins, lymphocytes, and fluid from interstitial spaces
- After a fatty meal, the lymph appears milky white and is called chyle
10. Clinical Significance
Chylothorax (Thoracic Duct Injury)
Disruption of the thoracic duct leads to chylothorax - chyle accumulating in the pleural cavity. The fluid appears milky-white.
Causes:
- Iatrogenic (most common): thoracic surgery (esophagectomy, mediastinal dissection), left-sided neck dissection at level IV
- Trauma
- Malignancy (especially lymphoma)
- Congenital (atresia of thoracic duct)
Diagnosis: Pleural fluid triglycerides (TAG) >110 mg/dL is pathognomonic for chylothorax. Chylomicrons are more specific but less practical.
Management:
- Low-output leaks (<500 mL/day): conservative - low-fat diet (MCT-based), systemic octreotide (reduces lymph flow), close monitoring of fluid/electrolyte balance
- High-output leaks (>500-1000 mL/day): total parenteral nutrition (TPN) to reduce gut lymph flow; surgical re-exploration and ligation
- Thoracic duct ligation is not harmful because anastomotic channels between lymphatic and venous systems exist in the lower neck
- Minimally invasive options: lymphangiography, thoracic duct embolization, thoracic duct disruption (multiple needle passes through the duct or cisterna chyli)
Note: ligation of the duct is safe because numerous anastomoses between lymphatic and venous systems exist.
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 829
- Fischer's Mastery of Surgery, p. 2442
- Murray and Nadel's Textbook of Respiratory Medicine
Surgical Landmark in Neck Dissection
The duct is at risk during level IV lymph node dissection in the neck (left side especially). The terminal portion arches over the left subclavian vein - a key danger zone.
Thoracic Duct Cysts
Rare mediastinal cysts arising from the thoracic duct wall - can present as an incidental mediastinal mass.
Metastatic Cancer
Because it drains the entire body, cancer cells can be found in thoracic duct fluid - notably, the Virchow's node (left supraclavicular lymph node) enlarges when tumor cells reflux from the thoracic duct into the left jugular trunk, indicating abdominal malignancy.
11. Anatomical Variations
Due to its complex embryological origin, the thoracic duct shows significant variability:
- It may be duplicated or plexiform over part of its course
- May cross midline at levels other than T4-T5
- The cisterna chyli may be absent (plexus instead)
- The terminal trunks may enter the venous system separately rather than as a single duct
- It may terminate in the left subclavian vein, internal jugular vein, or their junction
The most consistent anatomical landmark for surgical ligation is where the duct enters the chest through the aortic hiatus between T10-T12 - this is the site used for prophylactic ligation during esophagectomy.
- Mulholland and Greenfield's Surgery, p. 4358
Summary Table
| Feature | Detail |
|---|---|
| Length | 38-45 cm |
| Diameter | 2-5 mm |
| Origin | Cisterna chyli (L1-L2) |
| Enters thorax | Aortic hiatus (T12) |
| Crosses midline | At T4-T5 (right to left) |
| Termination | Left internal jugular + subclavian vein junction |
| Drainage territory | ~3/4 of body (all except right upper quadrant + right thorax) |
| Contents | Lymph, chylomicrons, fat, proteins, lymphocytes |
| Key clinical complication | Chylothorax (TAG >110 mg/dL in pleural fluid) |
Classify white matter of brain and describe internal capsule in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive, well-sourced content from multiple authoritative textbooks plus rich diagrams. Let me compile the detailed answer.
White Matter of the Brain - Classification and the Internal Capsule
PART I: Classification of White Matter of the Brain
The cerebral hemispheres contain billions of myelinated axons that give white matter its characteristic appearance. These fiber bundles carry information to and from the cerebral cortex and are classified into three main categories based on the direction and extent of their connections:
1. Projection Fibers
Projection fibers connect the cerebral cortex to subcortical structures (and vice versa). They are of two types:
- Corticofugal (efferent) - arise in the cortex and project downward to subcortical targets
- Corticospinal tract (to spinal cord)
- Corticobulbar tract (to brainstem motor nuclei)
- Corticopontine tract (to pontine nuclei)
- Corticothalamic fibers
- Corticoreticular fibers
- Corticopetal (afferent) - arise outside the telencephalon and project up to the cortex
- Thalamocortical radiations (sensory relay to cortex)
All projection fibers traveling between the cortex and deeper structures pass through the internal capsule. Above the level of the internal capsule, these fibers fan out into a broad sheet called the corona radiata, which merges superiorly with the white matter of the centrum semiovale.
Below the internal capsule, the same fibers converge to form the cerebral peduncles (basis pedunculi) in the midbrain.
2. Commissural Fibers
Commissural fibers interconnect corresponding (homotopic) or different (heterotopic) cortical areas in the two cerebral hemispheres. The main commissural systems are:
| Structure | Connection |
|---|---|
| Corpus callosum | Largest white matter bundle (~300 million axons); connects most cortical areas bilaterally |
| Anterior commissure | Connects anterior temporal lobes and olfactory areas |
| Posterior commissure | Connects caudal diencephalic regions |
| Hippocampal commissure (Psalterium) | Connects the two hippocampal formations |
The Corpus Callosum has four parts (from anterior to posterior):
- Rostrum - most anterior, thin
- Genu - curves anteriorly/dorsally; carries prefrontal and higher cognitive fibers
- Body (trunk) - largest part; carries motor, somatosensory, auditory fibers
- Isthmus - narrow junction between body and splenium
- Splenium - rounded posterior end; carries visual fibers and temporal/parietal information
Notable exceptions - the corpus callosum does NOT connect:
- The hand area of motor and somatosensory cortices
- The primary visual cortex (except areas near the vertical midline)
3. Association Fibers
Association fibers connect cortical areas within the same hemisphere. They are subdivided into:
Short Association Fibers
- Connect adjacent gyri within the same lobe
- Called U fibers (or arcuate fibers) because they curve in a U-shape between neighboring gyri
- Located just beneath the cortex in the subcortical white matter
Long Association Fibers
Five major long tracts:
| Tract | Course | Connection |
|---|---|---|
| Superior longitudinal fasciculus | Laterally, above the insula | Frontal - Parietal - Occipital cortices |
| Arcuate fasciculus | Arcs around the insula | Frontal lobe - Temporal lobe (key for language) |
| Uncinate fasciculus | Curved bundle, hooking under the Sylvian fissure | Orbital frontal lobe - Anterior temporal lobe |
| Inferior occipitofrontal fasciculus | Ventral and lateral course | Occipital lobe - Frontal lobe |
| Cingulum | Within white matter beneath cingulate gyrus | Cingulate gyrus - Parahippocampal gyrus |
| Inferior longitudinal fasciculus | Along temporal and occipital lobes | Temporal lobe - Occipital lobe |
Other notable structures: the external capsule (between claustrum and putamen) and the extreme capsule (between claustrum and insular cortex) also carry association fibers.
PART II: The Internal Capsule - Detailed Description
Overview
The internal capsule is a compact, V-shaped band of projection fibers that carries almost all afferent and efferent fibers traveling between the cerebral cortex and the brainstem/spinal cord. On a horizontal section, it appears like two arrowheads pointing inward (or like the letter "V" or a boomerang).
Relations (Borders)
The internal capsule is consistently bounded by specific structures on all sides:
| Side | Structure |
|---|---|
| Medial | Head of the caudate nucleus (anteriorly) + Thalamus (posteriorly) |
| Lateral | Lentiform nucleus (putamen + globus pallidus) |
| Below (continuation) | Cerebral peduncles of the midbrain |
| Above (continuation) | Corona radiata (fan-like spread to cortex) |
Mnemonic: "Caudate and Thalamus are always medial; Lentiform nucleus is always lateral."
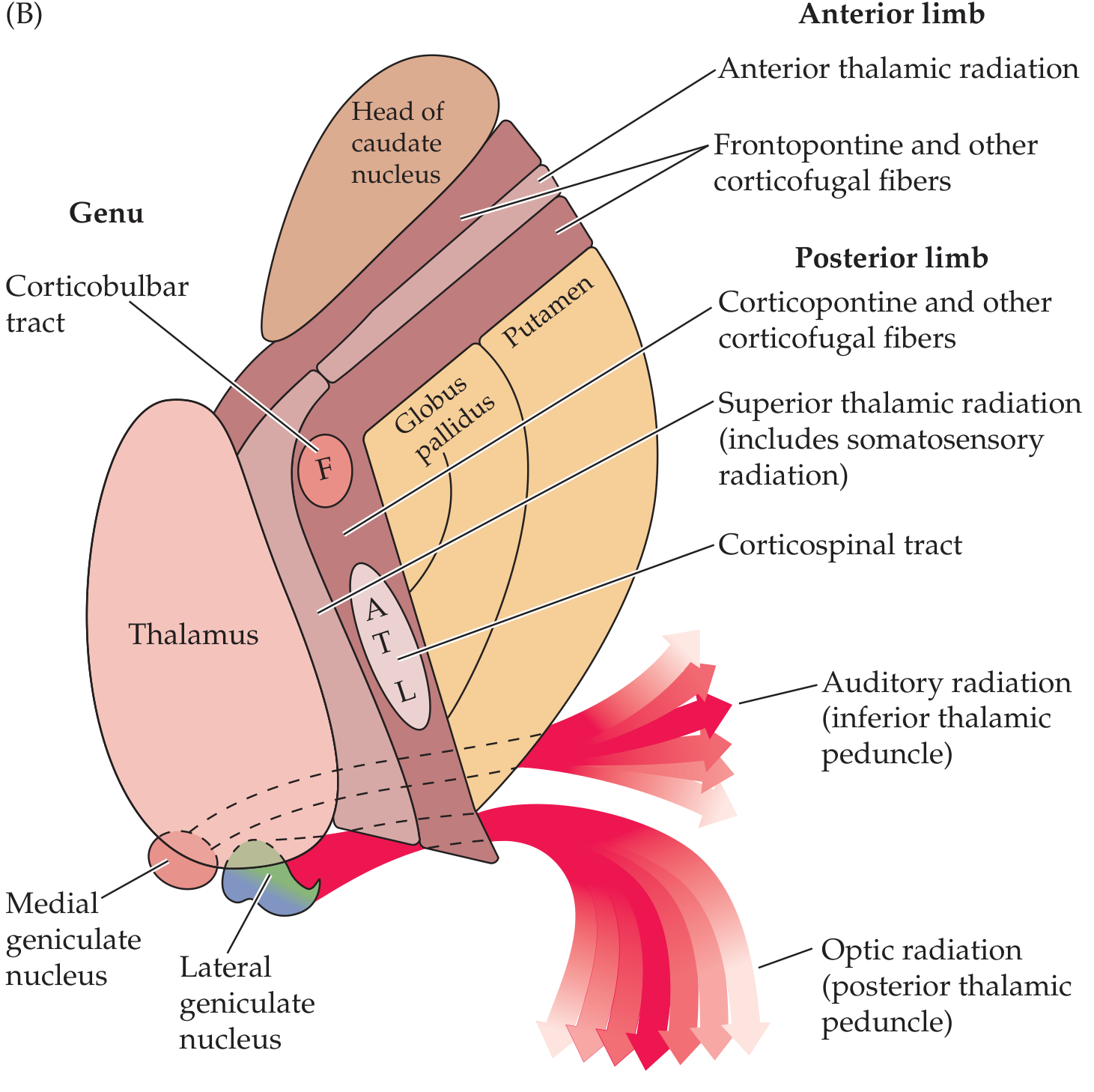
Fig. 6.9B from Neuroanatomy through Clinical Cases - Horizontal section of internal capsule showing all fiber pathways
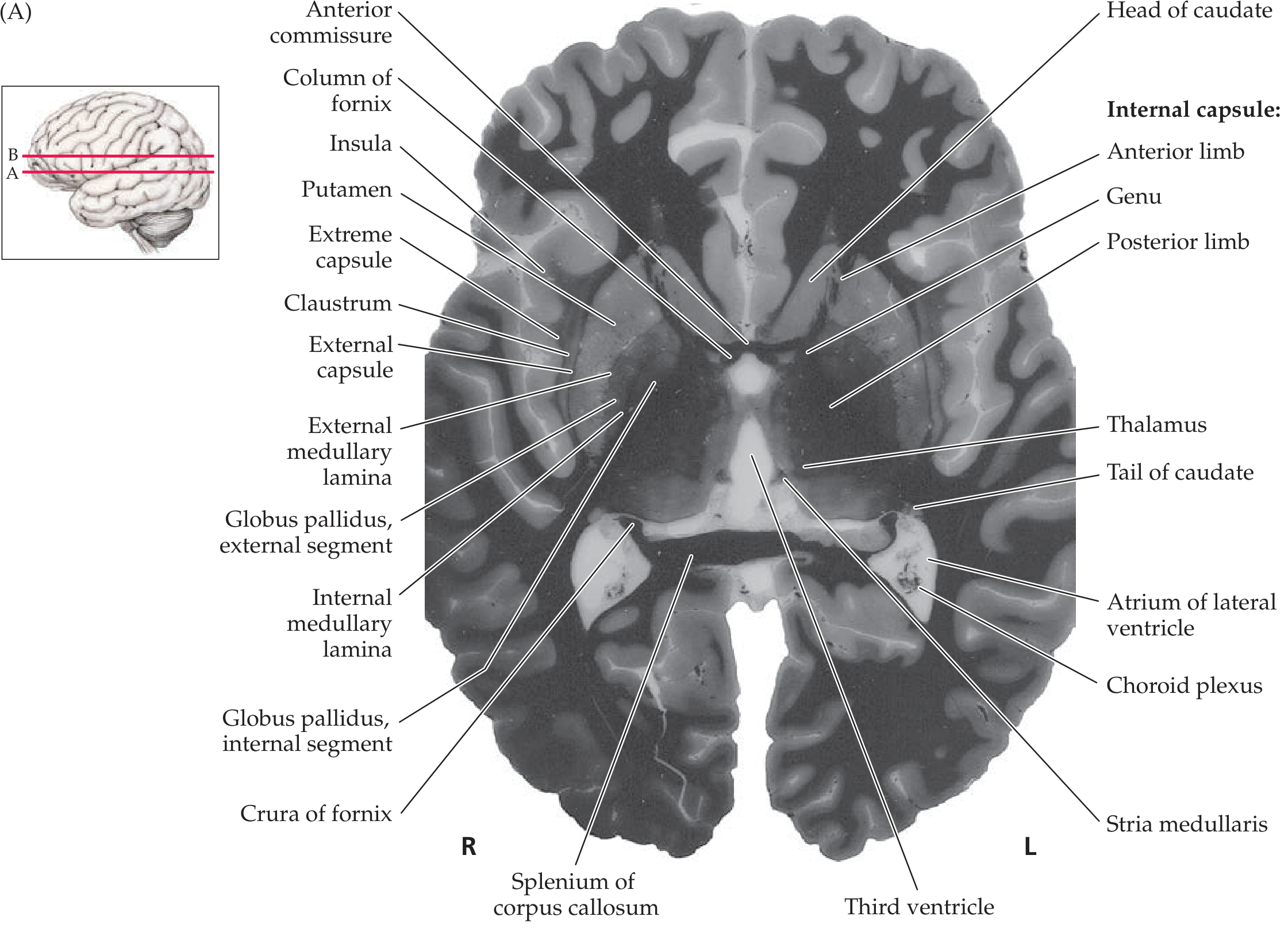
Fig. 16.2A from Neuroanatomy through Clinical Cases - Brain slice showing the internal capsule in relation to surrounding structures
Parts of the Internal Capsule
The internal capsule is divided into five parts:
1. Anterior Limb (Frontal Part)
- Located between the head of the caudate nucleus (medially) and the lentiform nucleus (laterally)
- Fibers carried:
- Anterior thalamic radiation - connects mediodorsal thalamic nucleus with prefrontal cortex
- Frontopontine fibers - from frontal cortex to pontine nuclei
- Other corticofugal fibers from the frontal lobe
2. Genu ("Knee")
- The bend between the anterior and posterior limbs
- Located at the level of the foramen of Monro
- Fibers carried:
- Corticobulbar (corticonuclear) tract - motor fibers from motor cortex to cranial nerve nuclei in the brainstem
- Somatotopic: face area most anterior
3. Posterior Limb (Occipital Part) - the LARGEST component
-
Located between the thalamus (medially) and the lentiform nucleus (laterally)
-
Fibers carried (from anterior to posterior within the limb):
- Corticospinal tract - voluntary motor fibers to the spinal cord; the most important fiber system
- Superior thalamic radiation - includes somatosensory radiation from VPL/VPM thalamus to parietal cortex
- Corticorubral fibers
- Corticothalamic fibers
- Corticoreticular fibers
- Corticopontine fibers (posterior frontal and parietal)
-
Somatotopic organization within corticospinal fibers (anterior to posterior):
- Face → Arm → Trunk → Leg (mnemonic: FATL)
- Face fibers are most anterior; leg fibers are most posterior
4. Retrolenticular (Retrolentiform) Part
- Lies posterior to the lenticular nucleus
- Fibers carried:
- Optic radiation (visual radiation / geniculo-calcarine tract / radiatio optica) - from lateral geniculate nucleus of the thalamus to the primary visual cortex (calcarine cortex)
- Corticotectal fibers
- Corticonigral fibers
5. Sublenticular (Sublentiform) Part
- Lies inferior to the lenticular nucleus
- Fibers carried:
- Auditory radiation - from medial geniculate nucleus of the thalamus to the primary auditory cortex (Heschl's gyri, superior temporal gyrus)
- Temporopontine fibers
Summary Table: Parts of the Internal Capsule and Their Fibers
| Part | Location | Key Fibers |
|---|---|---|
| Anterior limb | Between caudate head & lentiform | Anterior thalamic radiation, frontopontine fibers |
| Genu | Bend between anterior & posterior limbs | Corticobulbar tract (face) |
| Posterior limb | Between thalamus & lentiform | Corticospinal tract (arm, trunk, leg), superior thalamic radiation |
| Retrolenticular | Behind lentiform nucleus | Optic radiation |
| Sublenticular | Below lentiform nucleus | Auditory radiation |
Blood Supply of the Internal Capsule
This is clinically essential because small vessel disease here causes devastating strokes.
| Part of Internal Capsule | Arterial Supply |
|---|---|
| Anterior limb | Recurrent artery of Heubner (branch of anterior cerebral artery) |
| Genu | Anterior choroidal artery (branch of internal carotid artery) |
| Posterior limb - genu/middle/inferior | Anterior choroidal artery |
| Posterior limb - superior aspect | Lenticulostriate arteries (branches of middle cerebral artery) |
The lenticulostriate arteries (also called "arteries of cerebral hemorrhage" or Charcot's arteries) are particularly prone to rupture in hypertension, leading to hypertensive capsular hemorrhage.
- Localization in Clinical Neurology 8e, p. 32
Continuation of Internal Capsule Fibers
The fibers of the internal capsule are continuous with structures both above and below:
- Superiorly → Corona radiata (fan-like radiation spreading to all parts of the cortex)
- Inferiorly → Cerebral peduncles (basis pedunculi) in the midbrain
- Middle one-third: corticobulbar + corticospinal fibers
- Medial one-third: frontopontine fibers
- Lateral one-third: temporopontine + parietopontine fibers
Clinical Significance of the Internal Capsule
Because the internal capsule is a highly concentrated bundle of fibers, even a small lesion produces major deficits:
Capsular Stroke (Lacunar Infarct / Hypertensive Hemorrhage)
- Posterior limb lesion (most common): contralateral pure motor hemiplegia (face + arm + leg) due to damage to corticobulbar and corticospinal fibers
- Genu + posterior limb: hemiplegia + dysarthria (corticobulbar involved)
- Adding thalamic radiation: contralateral hemisensory loss
- Retrolenticular involvement: contralateral homonymous hemianopia
Posterior Limb Lesion Syndrome (from Bradley's Neurology)
Full syndrome includes:
- Contralateral hemiparesis
- Contralateral diminished pain and temperature
- Dysarthria
- Homonymous hemianopia (with a tongue of sparing along horizontal meridian)
- Memory impairment
- Right-sided lesions: visuoperceptual abnormalities
Arterial territory: anterior choroidal artery
Decoricate Rigidity
Hemorrhages or thromboses in the internal capsule can produce decorticate rigidity on the hemiplegic side due to interruption of corticospinal and corticoreticular fibers.
Why Small Lesions Cause Complete Hemiplegia
Despite the somatotopic arrangement, fibers at the capsular level are so compact that even a small lesion typically damages motor fibers for face, arm, and leg simultaneously - producing a complete contralateral hemiplegia.
- Neuroanatomy through Clinical Cases, 3rd Edition, p. 257-258
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 197-198
- Bradley and Daroff's Neurology in Clinical Practice
- Localization in Clinical Neurology 8e, p. 31-32
- Ganong's Review of Medical Physiology 26th Edition
This is a shared conversation. Sign in to Orris to start your own chat.