Potts spine
Reading File
Finding Sources
Finding Sources
Searching Images
Pott's spine tuberculosis vertebral
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information. Let me compile the full answer.
Pott's Disease (Tuberculous Spondylitis)
Pott's disease is spinal tuberculosis — extrapulmonary TB affecting the vertebral column, named after Percivall Pott (18th century). It is the most common form of skeletal TB, accounting for ~40% of all bone/joint TB cases.
Epidemiology
- Skeletal TB represents ~10% of extrapulmonary TB cases in the USA
- Spine is the most common skeletal site (40%), followed by hips (13%) and knees (10%)
- Predominantly affects immunocompromised individuals, those from TB-endemic regions, and the elderly
Pathogenesis
TB bacilli reach the spine via hematogenous spread (reactivation of old foci) or direct extension from adjacent paravertebral lymph nodes. The infection begins at the anterior superior or inferior angle of the vertebral body, then slowly spreads to the adjacent vertebral body and ultimately the intervertebral disc.
Sites of Involvement
| Age Group | Common Site |
|---|---|
| Children | Upper thoracic spine |
| Adults | Lower thoracic & upper lumbar vertebrae |
Two or more adjacent vertebral bodies are typically involved.
Pathology (Robbins)
- Infection destroys vertebral bodies and intervertebral discs
- Leads to compression fractures and kyphosis
- Granulomatous inflammation with caseous necrosis (mycobacterial osteomyelitis)

Clinical Features
- Back pain (most common presenting symptom)
- Gibbus deformity — angular kyphosis from vertebral body collapse
- Cold (paravertebral) abscess — hallmark finding
- Upper spine → tracks to chest wall (soft tissue mass)
- Lower spine → tracks along psoas muscle (psoas abscess) or to inguinal ligament
- Pott's paraplegia — most catastrophic complication; caused by abscess or granulation tissue compressing the spinal cord; paraparesis from a large abscess is a medical emergency requiring urgent drainage
Imaging
X-ray
- Endplate destruction, vertebral body collapse, disc space narrowing
- Focal angular kyphosis; Cobb angle used to quantify deformity

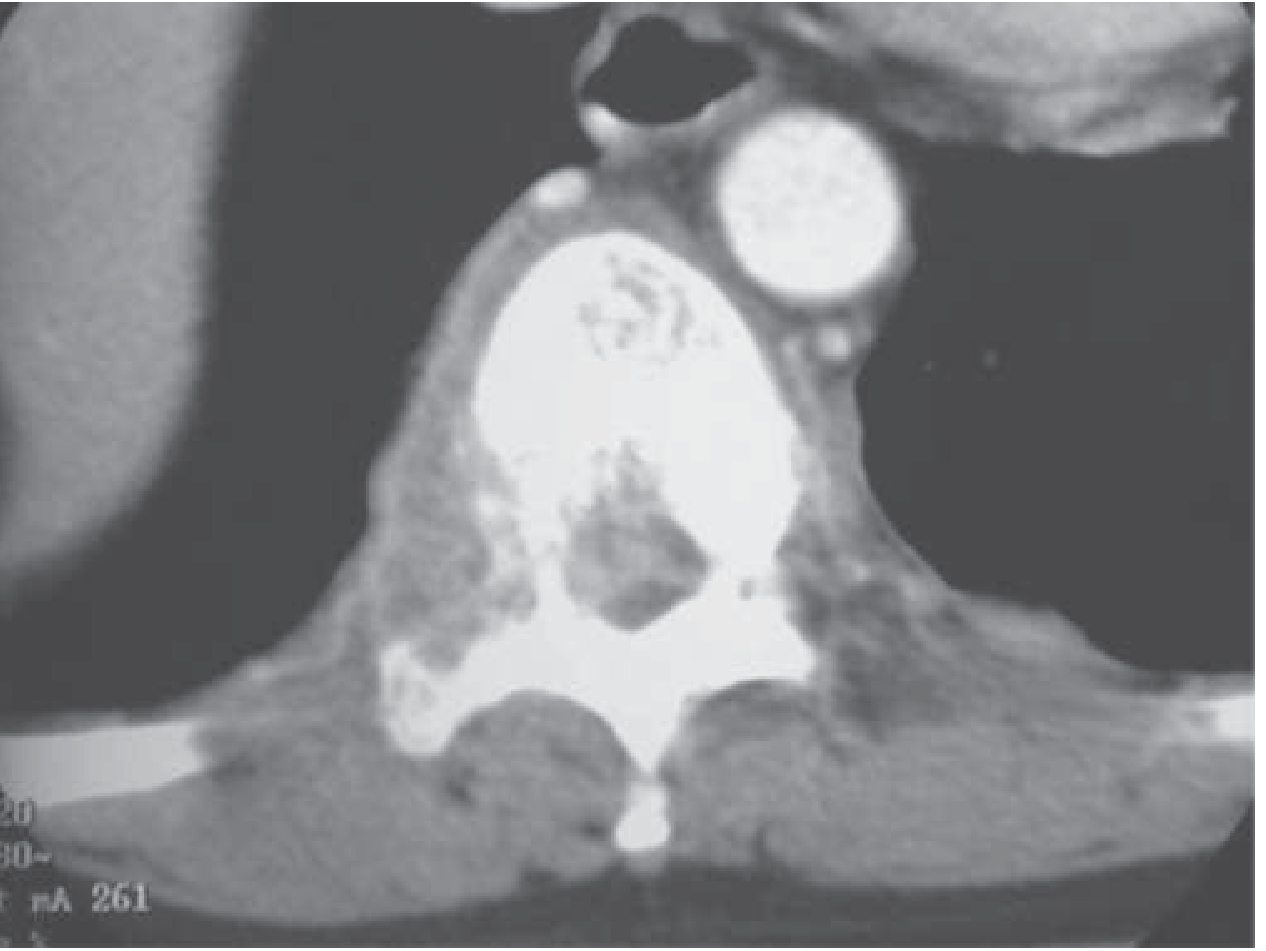
CT
- Defines extent of bone destruction; guides biopsy
- Shows pedicle destruction (see below)
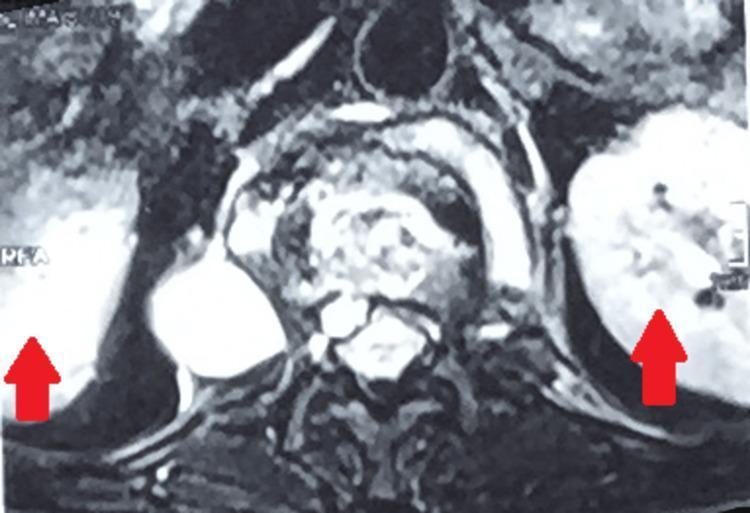
MRI (investigation of choice)
- ~90% accuracy for spinal infection
- Low T1 / high T2 signal in affected vertebral bodies and disc
- Characteristic features of TB vs. pyogenic spondylitis on MRI:
| Feature | Tuberculous | Pyogenic |
|---|---|---|
| Paraspinal abscess | Well-defined, thin enhancing rim | Irregular |
| Subligamentous spread | ≥3 vertebral levels | Less common |
| Vertebral enhancement | Heterogeneous, localized | Homogeneous, diffuse |
| Disc abscess | Vertebral intraosseous abscess with rim enhancement | Disc abscess with rim enhancement more common |
| Vacuum phenomenon | Absent | Present (suggests neuropathic or degenerative) |

Diagnosis
- CT/fluoroscopy-guided biopsy — percutaneous aspiration of abscess or bone biopsy; cultures usually positive, histology shows typical granulomas
- Synovial fluid (when joints involved): thick, high protein, variable cell count; culture positive in high percentage
- Differential diagnosis: pyogenic osteomyelitis (early disc involvement, rapid sclerosis), tumors
Treatment
- Antituberculous chemotherapy — mainstay; skeletal TB responds well
- Urgent surgical drainage — for Pott's paraplegia due to large abscess (medical emergency)
- Surgery — indicated in severe cases (instability, cord compression, failed medical therapy)
Sources: Harrison's Principles of Internal Medicine 22E, p. 1432 | Robbins Pathologic Basis of Disease, p. 1094 | Grainger & Allison's Diagnostic Radiology, pp. 1208–1209 | Adams and Victor's Principles of Neurology, 12th ed.
This is a shared conversation. Sign in to Orris to start your own chat.