Paraplegia- causes, localisation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Now I have comprehensive content. Let me compile the answer.
Paraplegia — Causes & Localisation
Definition
Paraplegia is paralysis (complete or incomplete) of both lower limbs. It results from interruption of descending corticospinal tracts or of motor neurons/peripheral nerves supplying the legs.
An injury below T1 causes paraplegia; above T1 (cervical cord) causes tetraplegia/quadriplegia. An injury in the upper cervical cord can cause death by denervating the diaphragm.
— Gray's Anatomy for Students
Localisation of the Lesion
The clinically important distinction is between spinal cord, nerve root, and peripheral nerve lesions.
1. Spinal Cord (most common site)
| Feature | Finding |
|---|---|
| Level of weakness | All muscles below the lesion level |
| Sensory loss | Circumferential sensory level on trunk (spinothalamic + posterior column involvement) |
| Reflexes (acute) | Flaccid paralysis + areflexia (spinal shock) |
| Reflexes (chronic) | Spastic paraplegia, hyperreflexia, bilateral Babinski signs, extensor/flexor spasms |
| Autonomic | Bladder & bowel dysfunction (initially atonic → later spastic), anhidrosis below level, orthostatic hypotension |
| Segmental LMN signs | At the level of the lesion: atrophy, areflexia, fasciculations (anterior horn / root damage) |
"With acute lesions, the paralysis is flaccid as a result of spinal cord hypoexcitability (spinal shock). Eventually, hypertonic, hyperreflexic paraplegia develops with bilateral Babinski signs." — Localization in Clinical Neurology, 8e
Level clues:
- Above T6 → risk of autonomic dysreflexia (severe uncontrolled hypertension)
- Cervicothoracic sympathetic chain involved → ipsilateral Horner syndrome
- Complete lower cord lesion → flexion at hips and knees; high/incomplete cord lesion → extension at hips and knees
2. Cauda Equina / Conus Medullaris
| Feature | Finding |
|---|---|
| Weakness | Flaccid, lower motor neuron (LMN) type |
| Reflexes | Absent (areflexia) |
| Sensory | Saddle anaesthesia, asymmetric radicular pattern |
| Bladder/bowel | Atonic (overflow incontinence) |
3. Peripheral Nerve Disease
- Motor loss is distal > proximal (mainly legs)
- Sphincter function usually spared
- Sensory loss is distal and often modality-selective
- Exceptions: Guillain-Barré syndrome, diabetic neuropathy, porphyria (more proximal involvement) — Adams and Victor's Principles of Neurology, 12e
Causes of Paraplegia
Acute Onset (minutes to hours)
| Cause | Notes |
|---|---|
| Spinal cord trauma | Most common cause — fracture-dislocation of spine |
| Spinal cord infarction | Anterior spinal artery occlusion; segmental aortic branch occlusion (dissecting aneurysm, atheroma, vasculitis, nucleus pulposus embolism) |
| Vascular malformation / dural AV fistula | Cord ischaemia by complex mechanism |
| Epidural/subdural haemorrhage | Haemorrhagic diathesis, warfarin; rarely post-lumbar puncture |
Subacute Onset (hours to days)
| Cause | Notes |
|---|---|
| Postinfectious myelitis | Demyelinating or necrotising myelopathy |
| Epidural abscess | Bacterial; cord compression |
| Epidural tumour | Cord compression |
| Paralytic poliomyelitis | Purely motor, mild meningitis |
| Guillain-Barré syndrome | Predominantly motor, ascending, often with sensory disturbance |
Chronic / Progressive Onset
| Cause | Notes |
|---|---|
| Multiple sclerosis | Most common cause of chronic spinal paraplegia in adults |
| Spinal tumour (intrinsic or extrinsic) | Intramedullary or extramedullary |
| Cervical spondylosis / disc prolapse | Especially with congenitally narrow canal |
| Subacute combined degeneration | Vitamin B12 or copper deficiency — posterior + lateral columns |
| Syringomyelia | Central cord cavitation |
| Epidural abscess (chronic) | Tuberculous, fungal, granulomatous |
| Syphilitic meningomyelitis | |
| HIV myelopathy / HTLV-1 | Tropical spastic paraparesis (HTLV-1) |
| Motor neuron disease (ALS) | Corticospinal tract degeneration |
| Neuromyelitis optica (NMO) | Aquaporin-4 antibody; severe transverse myelitis |
| Epidural lipomatosis | Usually steroid-related |
| Hereditary spastic paraplegia | Genetic — upper motor neuron degeneration |
| Degenerative lateral & posterior column disease |
Infantile / Congenital
| Cause | Notes |
|---|---|
| Periventricular leukomalacia | Most common cause of infantile diplegia (spastic legs > arms) |
| Congenital cysts / tumours / diastematomyelia | |
| Spinal cord infarction | Umbilical catheter thrombotic complication |
| Metabolic cerebral diseases | Leukodystrophies, lipid storage diseases |
— Adams and Victor's Principles of Neurology, 12e; Localization in Clinical Neurology, 8e
Key Localisation Summary
| Lesion Site | Pattern | Tone | Reflexes | Sphincters |
|---|---|---|---|---|
| Spinal cord (acute) | Below level | Flaccid (shock) | Absent → brisk | Impaired |
| Spinal cord (chronic) | Below level | Spastic | Hyperreflexic, Babinski | Impaired |
| Conus medullaris | Saddle + legs | Flaccid | Absent | Atonic |
| Cauda equina | Asymmetric radicular | Flaccid | Absent | Variable |
| Peripheral nerve | Distal legs | Flaccid | Absent/reduced | Usually spared |
| Bilateral cortex / parasagittal | Legs > arms (diplegia) | Spastic | Hyperreflexic | Variable |
Paraparesis
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
I now have sufficient content from authoritative sources to construct a comprehensive answer.
Paraparesis
Paraparesis is partial (incomplete) weakness of both lower limbs, in contrast to paraplegia which implies complete paralysis. The distinction is clinically important because paraparesis often represents a reversible or treatable condition.
Definition & Clinical Features
Spasticity of both legs gives rise to a spastic paraparesis: the legs are stiffly extended at the knees, plantarflexed at the ankles, and slightly flexed at the hips. Both legs circumduct, and the toes catch on the floor with each step. The gait is slow and laboured. When the disorder begins in childhood, there is a tendency to adduct the legs — the classic "scissors gait."
— Bradley and Daroff's Neurology in Clinical Practice
Classification
A. Spastic Paraparesis (UMN type)
Lesion in the corticospinal tracts — bilateral, above the level of the lumbar cord.
Features:
- Increased tone (spasticity), hyperreflexia, clonus
- Bilateral extensor plantar responses (Babinski sign)
- Weakness below the level of the lesion
- Bladder/bowel dysfunction
- Sensory level on trunk (if spinal cord)
Causes:
| Category | Examples |
|---|---|
| Degenerative / Structural | Cervical spondylotic myelopathy (most common cause of spastic paraparesis in patients >55 years), lumbar spondylosis, disc prolapse |
| Demyelinating | Multiple sclerosis, neuromyelitis optica (NMO) |
| Vascular | Anterior spinal artery infarction, spinal AV fistula/malformation |
| Infective | HTLV-1 associated myelopathy/tropical spastic paraparesis (HAM/TSP), HIV myelopathy, syphilitic meningomyelitis, epidural abscess (TB, bacterial) |
| Neoplastic | Spinal cord compression by extradural tumour (metastasis), intradural extramedullary (meningioma, neurofibroma), intramedullary tumour |
| Nutritional / Metabolic | Subacute combined degeneration (B12/copper deficiency — posterior + lateral columns) |
| Hereditary | Hereditary spastic paraplegia (HSP) — pure form: progressive spasticity, arms and sphincters unaffected; little or no actual weakness |
| Inflammatory | Transverse myelitis (post-infectious, autoimmune) |
| Structural malformations | Syringomyelia, Arnold-Chiari malformation |
| Parasagittal / bilateral cortical | Parasagittal meningioma, bilateral anterior cerebral artery territory strokes (legs > arms) |
"Cervical spondylotic myelopathy causes the greatest degree of impairment and disability in the continuum of spondylosis. In addition, myelopathy is the most common cause of spastic paraparesis in patients older [than 55]." — Tintinalli's Emergency Medicine
B. Flaccid Paraparesis (LMN type)
Lesion in the lower motor neurons, nerve roots, or peripheral nerves.
Features:
- Decreased or absent tone
- Areflexia or hyporeflexia
- Muscle wasting, fasciculations
- Sensory loss in radicular or "stocking" distribution
- Sphincters variably affected
Causes:
| Category | Examples |
|---|---|
| Cauda equina syndrome | Central disc prolapse (L4/5, L5/S1), epidural tumour, spinal stenosis |
| Conus medullaris lesion | Tumour, AVM, infarction |
| Guillain-Barré syndrome | Ascending, predominantly motor; post-infectious |
| Polyneuropathy | Diabetic, CIDP, toxic (heavy metals), paraneoplastic |
| Motor neuron disease | Lower motor neuron variant; primary lateral sclerosis (UMN) |
| Poliomyelitis | Pure LMN; anterior horn cell destruction |
Key Distinguishing Features: UMN vs LMN Paraparesis
| Feature | Spastic (UMN) | Flaccid (LMN) |
|---|---|---|
| Tone | Increased (spasticity) | Decreased (flaccidity) |
| Reflexes | Hyperreflexic, clonus | Hyporeflexic / absent |
| Plantar response | Extensor (Babinski +ve) | Flexor or absent |
| Wasting | Mild/late | Early and prominent |
| Fasciculations | Absent | May be present |
| Sensory level | Truncal level (cord) | Saddle/radicular/glove-stocking |
| Bladder | Spastic (urgency) | Atonic (retention/overflow) |
Important Mimics
- Bilateral leg dystonia (dystonic paraparesis): mimics spastic paraparesis; occurs in dopa-responsive dystonia in childhood. Can be misdiagnosed as HSP or cerebral diplegia. A "striatal toe" (spontaneous great toe extension) may be misinterpreted as Babinski.
- Distinction is critical: levodopa is curative in dopa-responsive dystonia.
"Occasionally bilateral leg dystonia (dystonic paraparesis) mimics a spastic paraparesis... Clinical differentiation between these conditions can be difficult. Brisk tendon reflexes occur in both." — Bradley and Daroff's Neurology in Clinical Practice
Investigation Approach
- MRI spine (with contrast): investigation of choice — exclude compressive, inflammatory, vascular, and demyelinating myelopathy
- MRI brain: parasagittal lesions, MS plaques
- CSF analysis: oligoclonal bands (MS), infection, inflammatory markers
- Serum B12, copper, folate: subacute combined degeneration
- HTLV-1 serology: in endemic regions or at-risk patients
- HIV serology
- VEPs, SSEPs: demyelination
- Genetic testing: hereditary spastic paraplegia (SPG gene panel)
- EMG/NCS: to differentiate from peripheral neuropathy or polyradiculopathy
"Patients with paraparesis of recent onset should be investigated with MRI of the spinal cord to exclude potentially treatable causes such as spinal cord compression." — Bradley and Daroff's Neurology in Clinical Practice
Wrist drop
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Excellent — comprehensive content gathered. Here is the structured answer:
Wrist Drop
Definition
Wrist drop (drop hand) is the inability to actively extend the wrist, resulting in the hand hanging flaccidly in a flexed/pronated position. It is the hallmark of radial nerve palsy.
Anatomy of the Radial Nerve
The radial nerve arises from the posterior cord of the brachial plexus (C5–C8, T1) and is the largest nerve in the upper extremity.
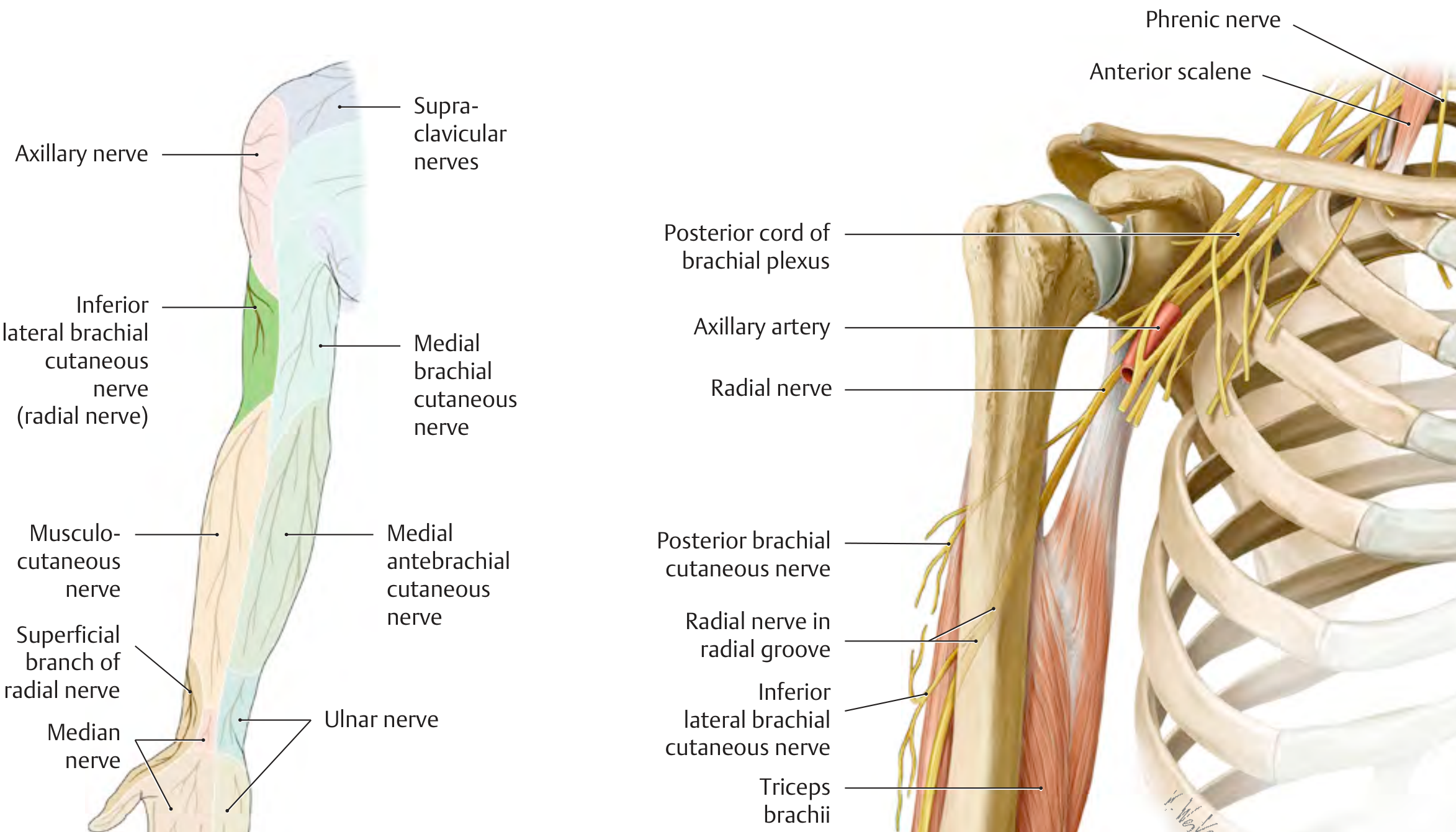
Key course:
- Axilla / Posterior cord → gives branches to all three heads of triceps and anconeus
- Spiral groove (radial groove) of humerus → most vulnerable site; gives posterior cutaneous nerves of arm and forearm
- Anterior to lateral epicondyle → innervates brachioradialis, ECRL, ECRB, supinator
- Radial tunnel / supinator canal → divides into two terminal branches:
- Superficial radial nerve — purely sensory (dorsal lateral hand, thumb, index, middle fingers)
- Posterior interosseous nerve (PIN) — purely motor (wrist/finger extensors)
— Bradley and Daroff's Neurology in Clinical Practice; General Anatomy and Musculoskeletal System, Thieme Atlas
Causes by Level of Radial Nerve Injury
1. Axillary / Proximal Lesion
| Cause | Notes |
|---|---|
| Improper crutch use ("crutch palsy") | Pressure in axilla |
| Sleeping partner's head on arm ("honeymoon palsy") | |
| Shoulder joint dislocation / fracture of proximal humerus | |
| Shoulder joint replacement |
Features: Wrist drop + triceps weakness (loss of elbow extension) + loss of triceps reflex + sensory loss over triceps, lateral arm, extensor forearm, dorsum of hand
2. Spiral Groove / Mid-Arm Lesion (most common)
| Cause | Notes |
|---|---|
| "Saturday night palsy" | Arm draped over chair/bench during drunken sleep; compresses nerve against humerus |
| "Park bench palsy" | Arm draped over park bench back |
| Humeral shaft fracture | Occurs in up to 15% of humerus shaft fractures |
| Improper positioning under general anaesthesia | |
| Exuberant callus after fracture | |
| Tendon expansion from lateral head of triceps |
Features: Wrist drop without triceps weakness (triceps branches exit before the spiral groove) + sensory loss over dorsum of hand
"The most common complication [of humeral shaft fracture], radial nerve injury, occurs in up to 15% of humerus fractures." — Rosen's Emergency Medicine
"Most radial nerve injuries are neuropraxias, or stretching of the nerve." — Schwartz's Principles of Surgery
3. Midlevel / Radial Tunnel
- Chronic compression in the lateral intermuscular septum or radial tunnel (bridging vessels, connective tissue septa)
- Features: Wrist drop + sensory disturbances
4. Posterior Interosseous Nerve (PIN) Lesion — Distal
Compression/injury occurs at the arcade of Frohse (proximal edge of the supinator muscle).
| Cause | Notes |
|---|---|
| Trauma / fracture/dislocation of radius | |
| Soft tissue masses (lipoma, ganglion) | |
| Rheumatoid arthritis (synovial proliferation) | |
| Neuralgic amyotrophy (Parsonage-Turner syndrome) | Acute pain then weakness |
Features:
- No true wrist drop (wrist extension is preserved, but weak/radially deviated)
- Radial deviation of wrist on extension — pathognomonic (ECU weak, ECRL spared)
- Dropped fingers — inability to extend at MCP joints
- No sensory loss (superficial branch already given off before the arcade)
5. Superficial Radial Nerve (Distal Sensory Branch Only)
Cheiralgia paresthetica — compression by:
- Tight wristbands, handcuffs
- IV cannulation, wrist surgery, de Quervain tenosynovitis
Features: Pure sensory — paresthesia/pain over dorsoradial hand; no motor loss (no wrist drop)
Summary Table: Lesion Level vs. Clinical Features
| Level | Triceps | Wrist Extension | Finger Extension | Brachioradialis | Sensory Loss | Triceps Reflex |
|---|---|---|---|---|---|---|
| Axilla | Weak | Lost | Lost | Weak | Arm + forearm + hand | Lost |
| Spiral groove | Intact | Lost | Lost | Weak | Dorsum of hand | Intact |
| Radial tunnel | Intact | Lost (partial) | Lost | Weak | Dorsum of hand | Intact |
| PIN (arcade of Frohse) | Intact | Intact (radial deviation) | Lost | Intact | None | Intact |
| Superficial radial | Intact | Intact | Intact | Intact | Dorsoradial hand only | Intact |
Differential Diagnosis of Wrist Drop
Though radial nerve palsy is the classic cause, always exclude:
| Condition | Distinguishing Features |
|---|---|
| C7 root lesion | Also affects triceps, wrist flexors (FCR), finger extensors; sensory loss in C7 dermatomal distribution; neck pain/radiculopathy |
| Posterior cord brachial plexus | Also involves axillary nerve (deltoid weakness, shoulder numbness) |
| Central (UMN) lesion | Spastic wrist drop with hyperreflexia, Babinski sign; stroke/tumour |
| Lead neuropathy | Classic cause of bilateral wrist drop; selective radial neuropathy from heavy metal toxicity |
| Multifocal motor neuropathy (MMN) | Radial nerve often involved; raised anti-GM1 antibodies |
Investigation
- Nerve conduction studies + EMG — essential to confirm site, extent, and prognosis; conduction block across spiral groove = demyelinating (good prognosis); low-amplitude CMAP = axon loss (slower recovery)
- Ultrasound of radial nerve — enlarged nerve (CSA >5.75 mm²) at spiral groove is highly specific for radial neuropathy
- MRI — if PIN lesion suspected (exclude mass lesion, synovitis)
- X-ray / CT humerus — if fracture-related
Prognosis & Management
- Saturday night palsy / compression neuropraxia: usually resolves in 6–8 weeks (demyelinating)
- Humeral fracture-associated axon loss: recovery takes months; surgical exploration if no recovery by 3–4 months
- PIN lesions from rheumatoid arthritis: local corticosteroid injection ± surgical decompression/synovectomy
- Wrist splint in dorsiflexion: maintains functional position, prevents contracture, and allows grip while awaiting recovery
This is a shared conversation. Sign in to Orris to start your own chat.