Part B: Hearing 149. Functional Anatomy and Functions of the Ear 1202 150. Auditory Pathways 1208 151. Mechanism of Hearing 1211 152. Hearing Defects and Hearing Tests Add clinical corelations all the diagrams possible in an image form Add importance of everything and drugs and treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"sensorineural hearing loss" AND treatment
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Part B: Hearing - Complete Notes with Clinical Correlations, Diagrams, Drugs & Treatment
Sources: Ganong's Review of Medical Physiology 26e, Costanzo Physiology 7e, Cummings Otolaryngology
CHAPTER 149: Functional Anatomy and Functions of the Ear
External Ear (Pinna + External Auditory Canal)
- Pinna (auricle): Collects and funnels sound waves; shape is slightly forward-facing, which helps with vertical sound localization. Reflections from the pinna surface change as sounds move up/down - the primary cue for locating sounds in the vertical plane.
- External Auditory Canal (EAC): ~2.5 cm long; S-shaped canal lined with ceruminous glands (wax) that has antibacterial properties and prevents foreign body entry.
- Tympanic Membrane: Translucent fibrous membrane separating the external from the middle ear. Responds to pressure changes by moving in and out, functioning as a resonator that reproduces vibrations of the sound source.
Middle Ear
Contains three ossicles: Malleus → Incus → Stapes
The middle ear achieves sound pressure amplification by:
- Lever action of malleus + incus: multiplies force 1.3×
- Area ratio: The tympanic membrane (~55 mm²) is ~17× larger than the oval window footplate, concentrating pressure. Combined amplification ≈ 22× (about 25 dB).
Protective reflex (acoustic/tympanic reflex): Loud sounds trigger contraction of:
- Tensor tympani (CN V3): pulls manubrium of malleus inward
- Stapedius (CN VII): pulls stapes footplate outward
Both reduce sound transmission and protect the cochlea from damage. The reflex has a latency of ~150 ms, so it cannot protect against sudden impulse sounds (e.g., gunshots).
Eustachian (pharyngotympanic) tube: Connects middle ear to nasopharynx. Normally closed; opens during swallowing or yawning to equalize pressure.
The Cochlea (Inner Ear)
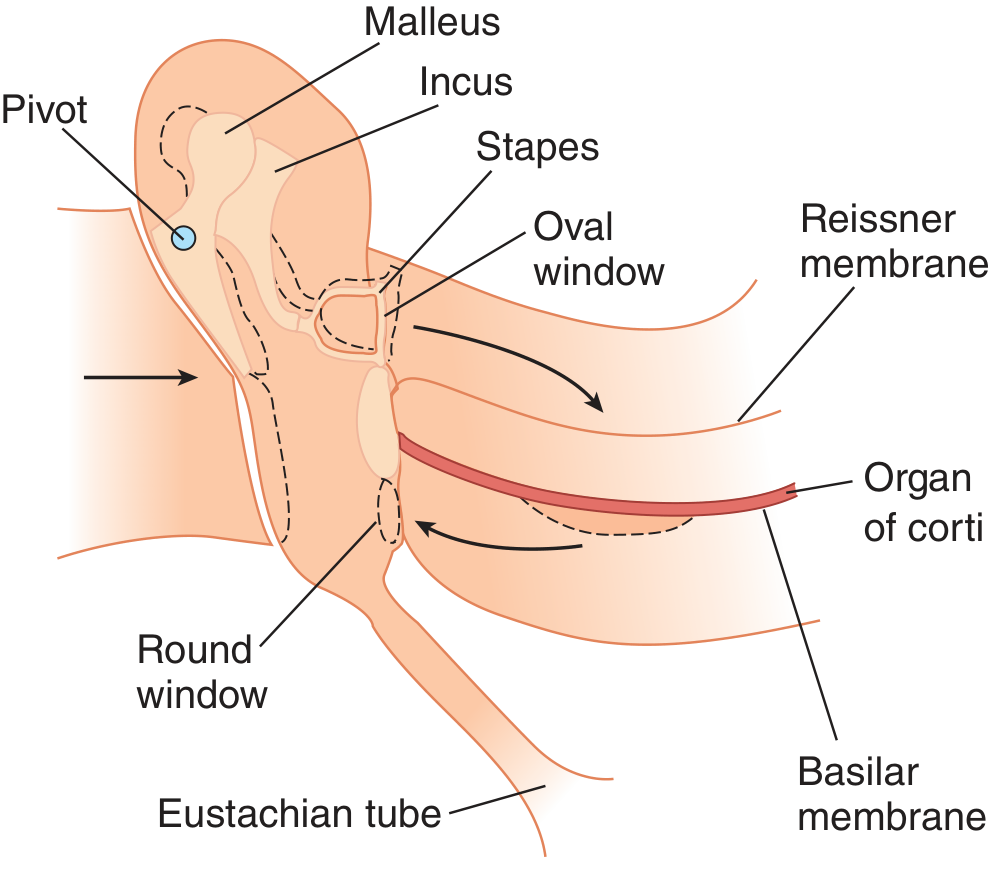
The cochlea is a coiled bony canal with 2.5 turns. In cross-section it has three scalae (chambers):
| Compartment | Fluid | Key Electrolytes |
|---|---|---|
| Scala vestibuli (above Reissner) | Perilymph | Na⁺ 150, K⁺ 5, Cl⁻ 125 mEq/L |
| Scala media (cochlear duct) | Endolymph | Na⁺ 1, K⁺ 150, Cl⁻ 130 mEq/L |
| Scala tympani (below basilar membrane) | Perilymph | Na⁺ 150, K⁺ 3, Cl⁻ 125 mEq/L |
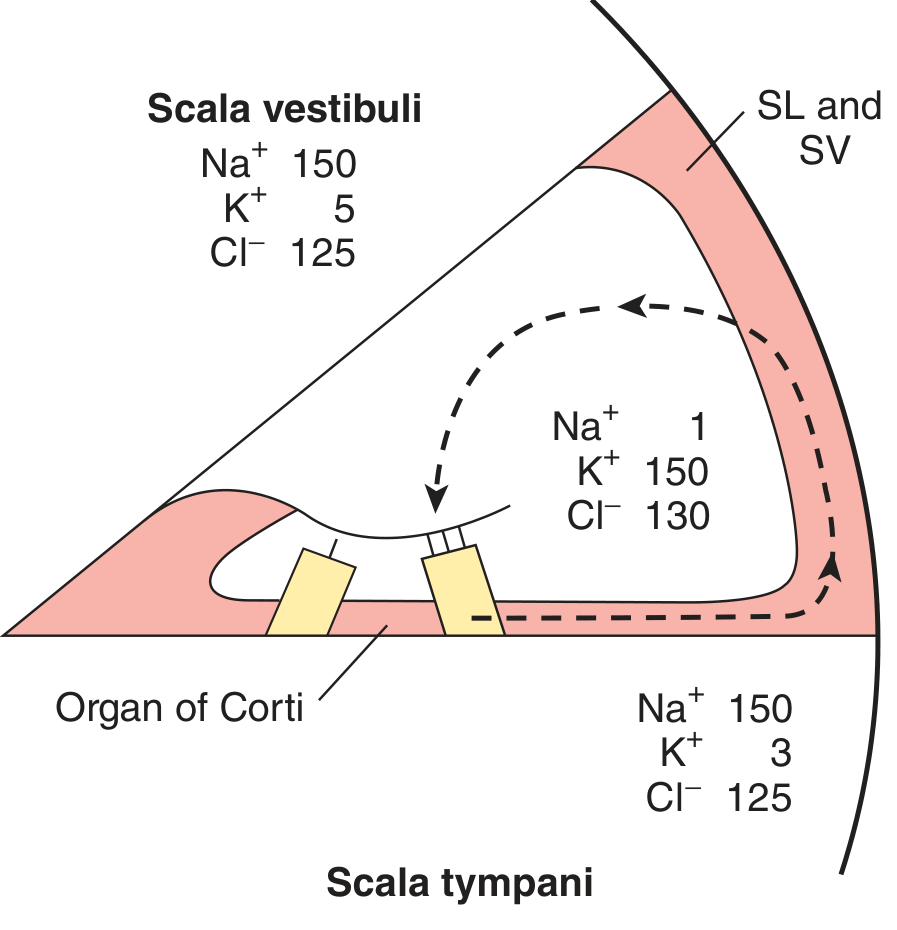
Endocochlear potential: +80 mV inside scala media (due to stria vascularis K⁺ pump). This large positive potential is the driving force for K⁺ into hair cell stereocilia during stimulation.
Stria vascularis: Secretes endolymph and maintains its ionic composition. Site of damage by loop diuretics (furosemide) and aminoglycosides.
Organ of Corti
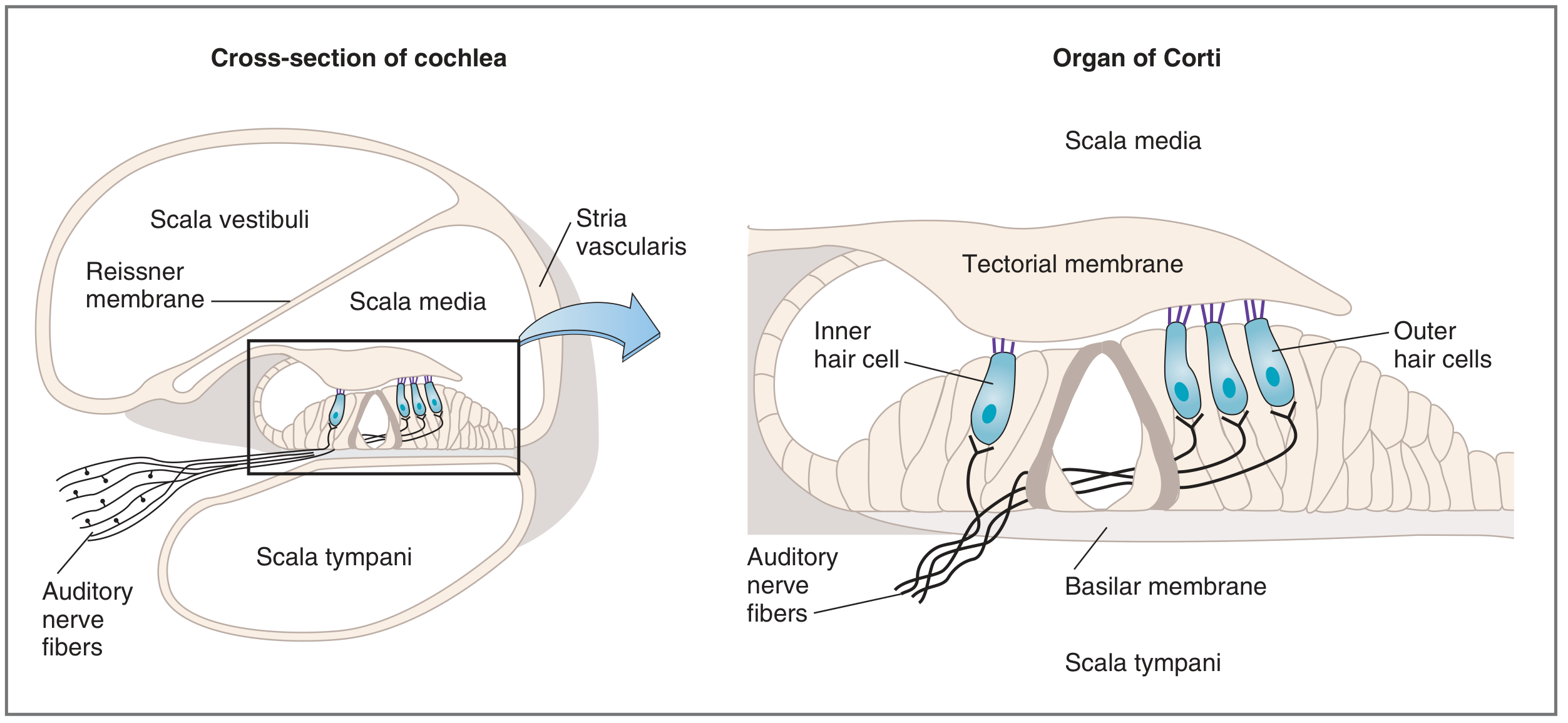
The organ of Corti sits on the basilar membrane and is bathed in endolymph of the scala media. It contains:
| Cell Type | Number | Arrangement | Function |
|---|---|---|---|
| Inner hair cells (IHC) | ~3,500 | Single row | Primary sensory transducers - generate action potentials |
| Outer hair cells (OHC) | ~12,000 | 3 parallel rows | Electromotile amplifiers - increase amplitude & clarity |
- Hair cell cilia (stereocilia): Tip links connect adjacent stereocilia. Deflection toward taller stereocilia opens mechanically gated K⁺/Ca²⁺ channels.
- Tectorial membrane: Overlies and contacts the tallest stereocilia of OHCs (IHCs may be stimulated by fluid movement).
- Basilar membrane: Wider and more flexible at apex; narrower and stiffer at base.
- Base (near oval window): best for high-frequency sounds
- Apex: best for low-frequency sounds
- Spiral ganglion: Cell bodies of bipolar neurons of CN VIII, located in the modiolus.
Outer Hair Cell Motor Protein: Prestin
OHC depolarization → cells shorten; hyperpolarization → cells lengthen. This electromotility depends on the protein prestin and amplifies sound vibrations up to ~1000-fold. Mutations in prestin cause moderate sensorineural hearing loss (DFNB61).
Clinical Correlation - Meniere's Disease: Endolymphatic hydrops (excess endolymph) distorts the scala media, damaging both IHCs and OHCs. Presents with episodic vertigo, tinnitus, low-frequency sensorineural hearing loss, and aural fullness. The high K⁺ in endolymph leaking into perilymph (K⁺ intoxication) poisons hair cells.
Clinical Correlation - Otosclerosis: Sclerotic bone fixates the stapes footplate at the oval window → conductive hearing loss. Treated by stapedectomy/stapedotomy with prosthesis implant.
Clinical Correlation - Otitis Media: Fluid accumulation in middle ear reduces ossicular mobility → conductive hearing loss. Treated with antibiotics (amoxicillin first-line); myringotomy ± tympanostomy tubes for recurrent cases.
CHAPTER 150: Auditory Pathways
Ascending Auditory Pathway
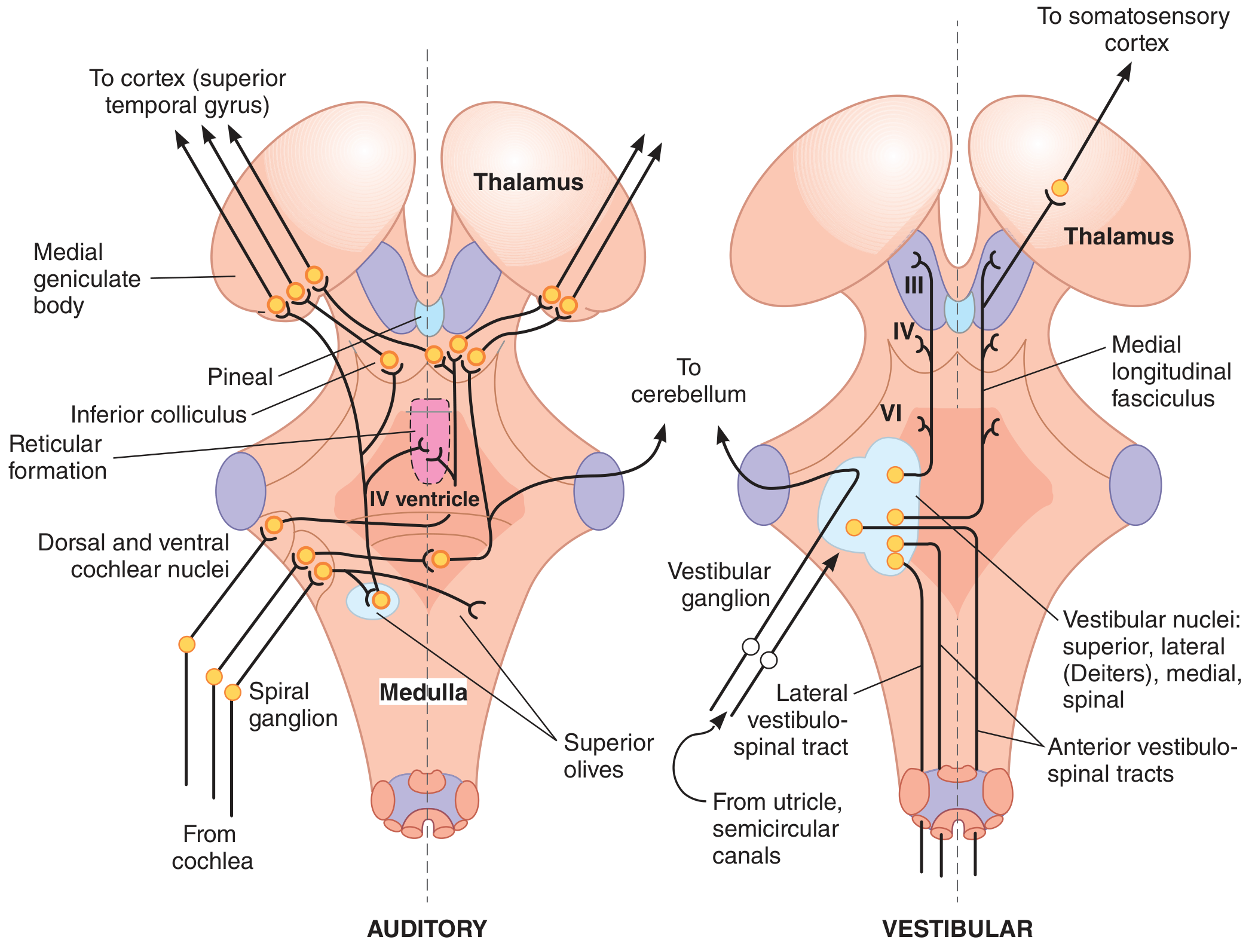
Relay stations in order:
- Spiral ganglion (CN VIII) - bipolar neurons; cell bodies in the modiolus of cochlea
- Cochlear nuclei (medulla, at pontomedullary junction) - dorsal and ventral divisions; ALL fibers synapse here first
- Superior olivary complex (pons) - first site of binaural convergence; important for sound localization (interaural time differences <20 μs detected here)
- Nucleus of lateral lemniscus (pons)
- Inferior colliculus (midbrain tectum) - auditory reflex center (startle reflex to sound)
- Medial geniculate body (MGB) (thalamus) - last subcortical relay
- Primary auditory cortex (A1) - Heschl's gyri on superior temporal plane (Brodmann areas 41 & 42)
Key features:
- Pathway is predominantly contralateral (most fibers cross at the trapezoid body)
- However, bilateral representation exists because fibers cross at multiple levels
- Result: unilateral cortical lesions cause minimal hearing loss (both ears still relay to surviving cortex)
- Tonotopic organization is preserved throughout the entire pathway (place principle)
Efferent (Descending) Pathway
- Olivocochlear bundle (bundle of Rasmussen): Efferent fibers from superior olivary complex → organ of Corti (primarily to OHC bases)
- Neurotransmitter: Acetylcholine (inhibitory on OHCs)
- Function: Modulates OHC sensitivity - blocks background noise, improves signal-to-noise ratio
Auditory Cortex Functions
- Tonotopic map: Low frequencies processed anterolaterally; high frequencies posteromedially
- Sound pattern recognition: Musical melodies, speech processing (Wernicke's area overlaps)
- Sound localization: Binaural comparison (lesions severely disrupt localization)
- Auditory association areas (Brodmann 22): Interpret meaning of sounds
Clinical Correlation - Cortical deafness: Bilateral lesions of primary auditory cortex cause cortical deafness. Patient can have normal audiogram but cannot process meaning of sound. Wernicke's aphasia (dominant hemisphere area 22 lesion) = inability to understand spoken language despite hearing it.
Clinical Correlation - Acoustic neuroma (Vestibular schwannoma): Benign tumor of CN VIII Schwann cells at cerebellopontine angle. Presents with unilateral progressive SNHL, tinnitus, then facial numbness and imbalance. Diagnosed with MRI gadolinium. Treatment: microsurgery (translabyrinthine, retrosigmoid, or middle fossa approach) or stereotactic radiosurgery (Gamma Knife).
CHAPTER 151: Mechanism of Hearing
Sound Waves and Properties
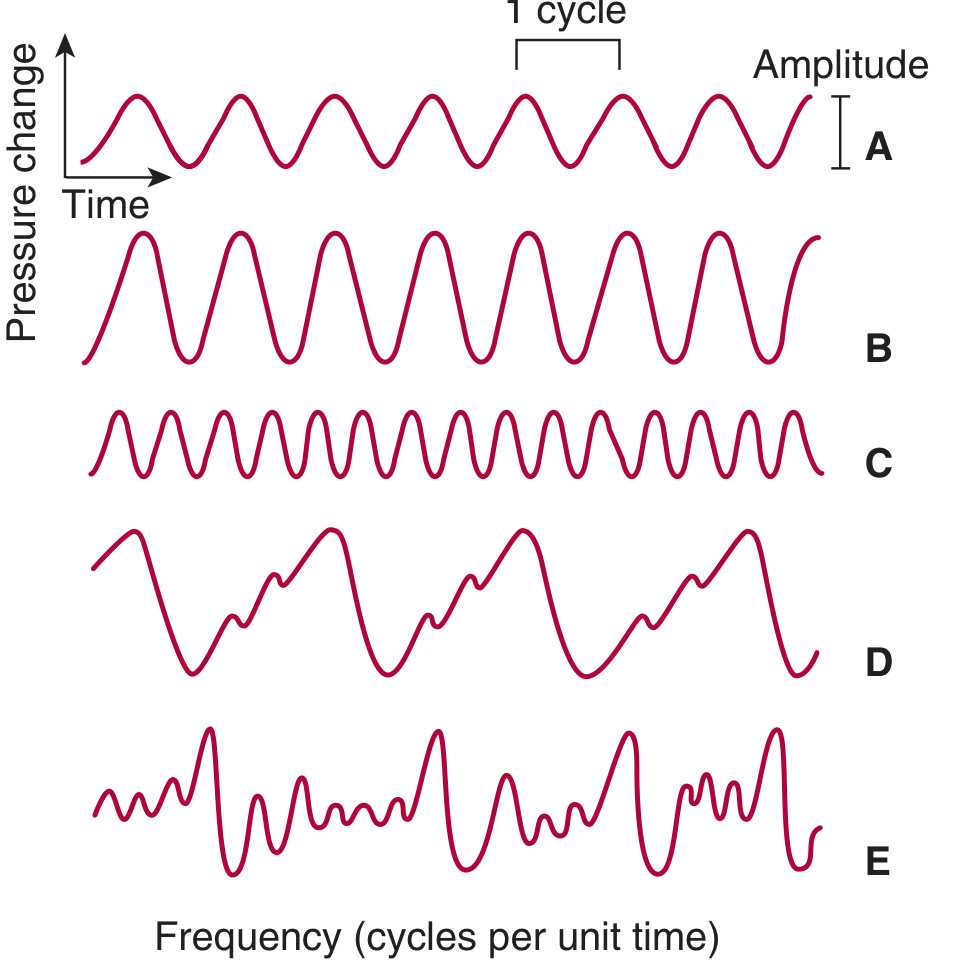
- Loudness = amplitude of pressure wave → measured in decibels (dB)
- 0 dB = threshold reference (0.000204 dyne/cm² or 20 μPa)
- 0–140 dB range = 10⁷-fold variation in pressure
- 0 dB does not mean no sound; it means equal to the reference standard
- Pitch = frequency (Hz) of the wave
Decibel scale of common sounds:
| dB Range | Examples |
|---|---|
| 120-160 dB | Firearms, jet engine takeoff (PAINFUL) |
| 90-110 dB | Subway, chainsaw, bass drum |
| 60-80 dB | Alarm clock, conversation, traffic |
| 40-50 dB | Normal room noise, moderate rain |
| 30 dB | Whisper, library (FAINT) |
| >85 dB | Threshold for noise-induced hearing loss |
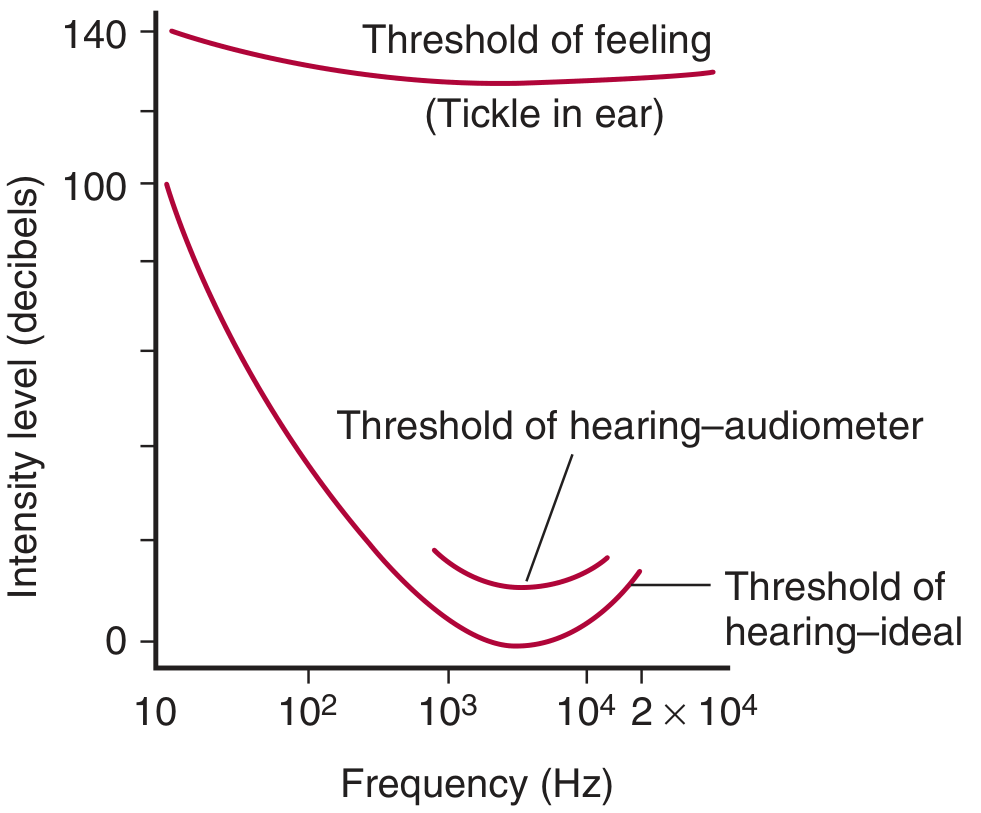
- Frequency range of human hearing: 20 to 20,000 Hz
- Best hearing sensitivity: 1,000 to 4,000 Hz range (speech frequencies)
- Male conversational voice: ~120 Hz; Female: ~250 Hz
- Masking: One sound reduces ability to hear others by causing relative refractoriness in stimulated fibers
Human Audibility Curve
Sound Transmission - Step-by-Step
Step 1: External ear → Tympanic membrane
Sound waves travel at 344 m/s in air (at 20°C). Strike the tympanic membrane, causing it to vibrate in and out.
Step 2: Middle ear ossicular chain
Tympanic membrane → Malleus (manubrium) → Incus (long process) → Stapes (footplate presses on oval window)
Malleus rocks on an axis at the junction of its long and short processes; the short process transmits vibrations to the incus. This creates the lever action that amplifies force 1.3×.
Step 3: Oval window → Cochlear fluid displacement
Stapes footplate pushes perilymph of scala vestibuli. Since fluid is incompressible, the round window membrane must bulge outward to accommodate the volume change.
Step 4: Traveling wave on basilar membrane
Movements of stapes set up traveling waves in perilymph. Wave amplitude increases to a maximum at a location determined by frequency (tonotopy = place principle):
- High frequencies (>4000 Hz): maximum at base (narrow, stiff basilar membrane)
- Low frequencies (<500 Hz): maximum at apex (wide, compliant basilar membrane)
- ~1000 Hz: ~30 mm from base (~midway along membrane)
This is von Bekesy's traveling wave theory (Nobel Prize 1961).
Step 5: Hair cell transduction
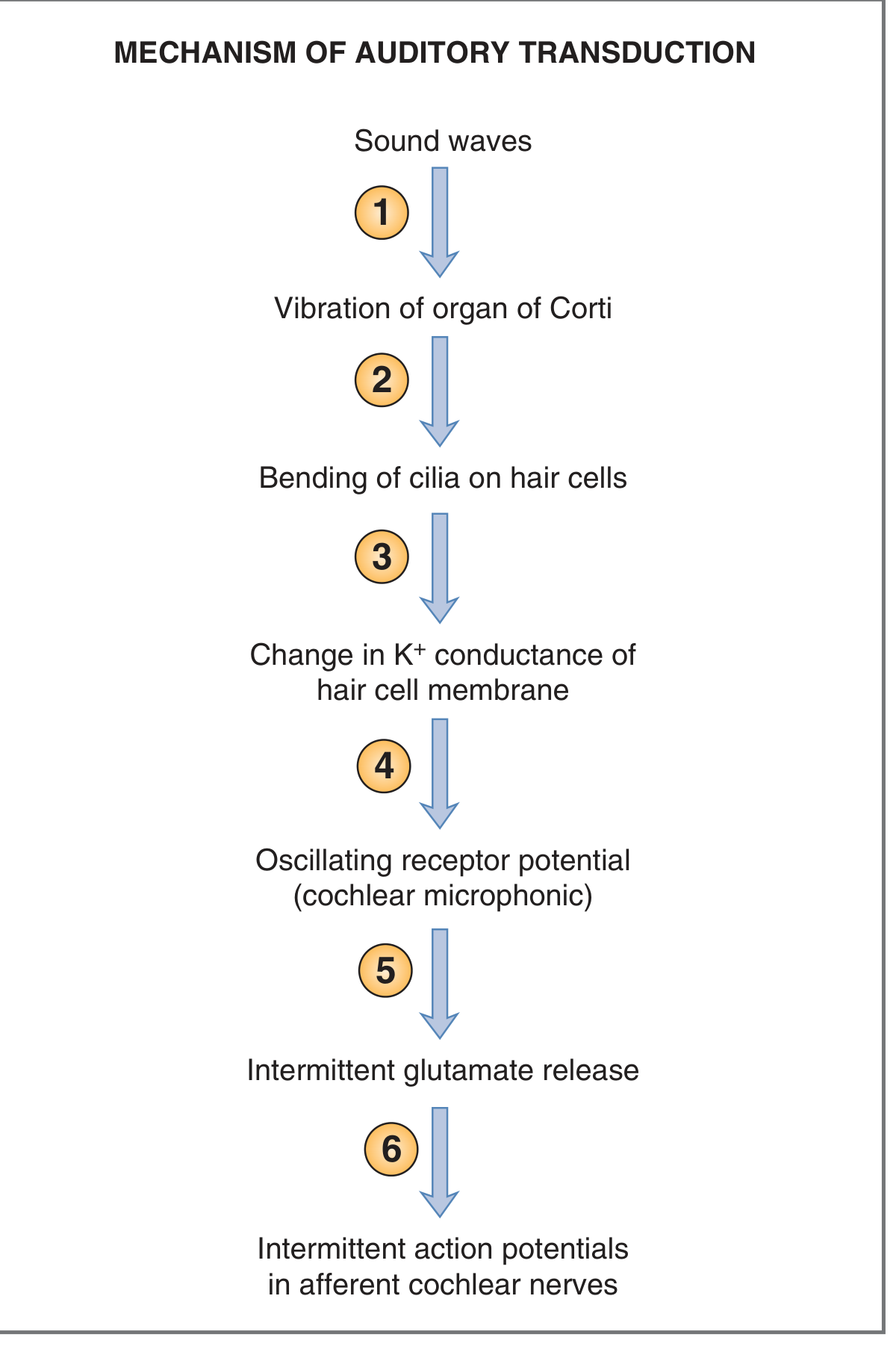
When the basilar membrane deflects upward:
- Organ of Corti moves relative to tectorial membrane
- Stereocilia deflect toward the tallest cilia (toward modiolus)
- Tip links pull open mechanically-gated K⁺ channels in stereocilia tips
- K⁺ flows IN from endolymph (driven by +80 mV endocochlear potential + high K⁺ in endolymph)
- Hair cell depolarizes → voltage-gated Ca²⁺ channels open at base
- Ca²⁺ triggers glutamate release onto afferent CN VIII dendrites
- Action potentials travel to cochlear nuclei
Deflection in opposite direction hyperpolarizes the cell and closes K⁺ channels.
The oscillating receptor potential that mirrors sound frequency = Cochlear Microphonic (Wever-Bray phenomenon).
K⁺ Recycling (Cochlear Battery)
K⁺ enters hair cells from endolymph → exits into perilymph at base of hair cell → taken up by supporting cells → passes through gap junctions to spiral ligament → stria vascularis pumps K⁺ back into scala media. This recycling maintains the endocochlear potential and is disrupted by mutations in connexin 26 (GJB2) - the most common cause of congenital hearing loss.
Sound Localization
- Below 3000 Hz: Detected by interaural time difference (as little as 20 μs, detected by superior olivary neurons)
- Above 3000 Hz: Detected by interaural intensity (loudness) difference
- Vertical plane: Detected by pinna shape and sound reflections
- Cortical lesions markedly disrupt localization
CHAPTER 152: Hearing Defects and Hearing Tests
Classification of Hearing Loss
| Feature | Conductive Hearing Loss | Sensorineural Hearing Loss |
|---|---|---|
| Location | External or middle ear | Cochlea (hair cells) or CN VIII/central |
| Frequencies affected | All equally | Often specific frequencies; high-frequency typical |
| Bone conduction | Normal or better | Reduced |
| Rinne test | BC > AC (negative Rinne) | AC > BC (positive Rinne, worse than normal) |
| Weber test | Lateralizes to affected ear | Lateralizes to unaffected ear |
| Speech discrimination | Good (loud enough) | Often poor |
Causes of Conductive Hearing Loss
- Cerumen impaction (ear wax)
- Otitis externa ("swimmer's ear" - Pseudomonas, S. aureus)
- Otitis media - fluid accumulation/scarring/tympanic perforation
- Otosclerosis: Abnormal sclerotic bone fixates stapes footplate at oval window
- Ossicular chain disruption (trauma, cholesteatoma)
- Exostoses/osteoma of EAC
Causes of Sensorineural Hearing Loss (SNHL)
- Noise-induced: Most common preventable cause; OHCs most vulnerable; 4000 Hz "notch" on audiogram is characteristic
- Presbycusis: Age-related, gradual cumulative hair cell loss; bilateral, symmetric, high-frequency
- Ototoxic drugs (see below)
- Acoustic neuroma/vestibular schwannoma
- Viral labyrinthitis (mumps, measles, CMV)
- Sudden SNHL (idiopathic - treat urgently with corticosteroids)
- Genetic mutations - connexin 26 (most common congenital), prestin, myosin mutations
- Autoimmune inner ear disease
- Meniere's disease (endolymphatic hydrops)
Ototoxic Drugs - Key Table
| Drug Class | Examples | Mechanism | Notes |
|---|---|---|---|
| Aminoglycoside antibiotics | Streptomycin, Gentamicin, Amikacin, Neomycin, Tobramycin | Block mechanosensitive K⁺ channels in stereocilia; primarily damage OHCs | Risk increased with prolonged use, renal failure, concurrent loop diuretics |
| Loop diuretics | Furosemide, Ethacrynic acid | Damage stria vascularis; disrupt endolymph ionic composition | Usually reversible if stopped; ethacrynic acid most ototoxic |
| Platinum-based chemotherapy | Cisplatin, Carboplatin | Reactive oxygen species damage OHCs and stria vascularis | Often irreversible; monitor with serial audiograms |
| Salicylates | Aspirin (high dose >6-8 g/day) | Inhibit prestin (OHC motor protein); reduce endocochlear potential | Usually reversible on discontinuation |
| Quinine | Quinine | Similar to salicylates | Usually reversible |
| Vancomycin | Vancomycin | Synergistic toxicity with aminoglycosides | Particularly dangerous combination |
Clinical Tip: The combination of aminoglycoside + loop diuretic + cisplatin is extremely ototoxic. Always check renal function and use trough monitoring for aminoglycosides.
Tuning Fork Tests (512 Hz tuning fork preferred)
| Test | Normal | Conductive Loss (affected ear) | SNHL (affected ear) |
|---|---|---|---|
| Rinne | AC > BC (Positive) | BC > AC (Negative Rinne) | AC > BC (Positive but reduced) |
| Weber | No lateralization (midline) | Lateralizes to affected ear | Lateralizes to unaffected (better) ear |
| Schwabach | Normal duration vs examiner | Prolonged (bone conduction preserved) | Shortened |
| Bing | Occlusion increases perceived loudness (BC) | No change (negative Bing) | Increases (positive Bing) |
| Gelle's | Pressure changes alter BC | No change (negative) in otosclerosis | Normal alteration |
Rinne test interpretation:
- Positive Rinne (AC > BC) = normal OR sensorineural loss
- Negative Rinne (BC > AC) = conductive loss or false-negative (dead ear - sound heard by contralateral ear via skull transmission)
- A gap of >20 dB between BC and AC thresholds on audiometry suggests conductive component
Weber test:
- Conductive loss: Affected ear is "quieter" from outside, but bone-conducted sound through skull reaches it better = lateralizes to worse ear
- SNHL: Cochlea on affected side is damaged; normal cochlea receives the signal = lateralizes to better ear
Audiometry
An audiometer presents pure tones via earphones at different frequencies, plotting hearing threshold at each frequency as a percentage of normal. Key features:
- Air conduction (AC) tests entire pathway (external + middle + inner + neural)
- Bone conduction (BC) tests cochlea + neural pathway only (bypasses external and middle ear)
- Air-bone gap: BC threshold better than AC threshold by ≥10 dB → conductive component
- Speech audiometry: Tests word recognition score (WRS/SDS) - poor in SNHL
Audiogram patterns:
- Conductive loss: Flat loss across frequencies; BC normal; air-bone gap present
- Presbycusis: Bilateral symmetric high-frequency (>2 kHz) sloping SNHL
- Noise-induced: Notch at 4000 Hz (4 kHz notch), with partial recovery at 8 kHz
- Meniere's disease: Low-frequency SNHL (early stages)
- Acoustic neuroma: Unilateral asymmetric SNHL, poor speech discrimination disproportionate to pure tone loss
Other Hearing Tests
| Test | Principle | Use |
|---|---|---|
| Tympanometry (impedance audiometry) | Measures eardrum compliance at different ear canal pressures | Type B flat = middle ear effusion; Type C = Eustachian tube dysfunction; Type A = normal |
| Acoustic reflex testing | Tests stapedius reflex arc (CN VII loop) | Absent reflex = middle ear disease or CN VII palsy |
| Otoacoustic emissions (OAEs) | OHCs generate sounds in response to clicks; recorded in canal | Newborn hearing screening; absent in SNHL >30 dB |
| Auditory brainstem response (ABR/BERA) | Records electrical potentials from cochlea to midbrain (waves I-V) | Objective hearing threshold; screening in infants; diagnosing acoustic neuroma |
| Electrocochleography (ECochG) | Records cochlear microphonic, summating potential, and action potential | Diagnosis of Meniere's disease (elevated SP/AP ratio >0.35) |
ABR Wave Generators:
- Wave I: Distal CN VIII (spiral ganglion)
- Wave II: Proximal CN VIII
- Wave III: Cochlear nucleus
- Wave IV: Superior olive
- Wave V: Lateral lemniscus / inferior colliculus
- Wave VI/VII: Medial geniculate body / auditory cortex
Acoustic neuroma prolongs or abolishes interpeak latency I-V.
Treatment of Hearing Loss
Conductive Hearing Loss
- Cerumen: Ear drops (carbamide peroxide, sodium bicarbonate, olive oil) or mechanical removal/irrigation
- Otitis media: Amoxicillin (first-line), amoxicillin-clavulanate (resistant strains); tympanostomy tubes for chronic effusion
- Otitis externa: Topical antibiotic + steroid drops (e.g., ciprofloxacin + dexamethasone)
- Otosclerosis: Stapedectomy/stapedotomy (Teflon or wire prosthesis); sodium fluoride may slow bone resorption; hearing aids
- Ossicular chain reconstruction: Prostheses (PORP/TORP) in tympanoplasty
Sensorineural Hearing Loss
- Sudden SNHL: High-dose systemic corticosteroids (prednisone 1 mg/kg/day for 10-14 days) or intratympanic steroid injection (dexamethasone or methylprednisolone) - guidelines from Kitoh et al. 2024, PMID 38968877
- Aminoglycoside-induced: Discontinue drug; no proven rescue therapy; prevention with careful dosing and monitoring
- Noise-induced: Prevention (hearing protection >85 dB); no proven reversal; N-acetylcysteine and magnesium studied as protective agents
- Autoimmune inner ear disease: Corticosteroids; methotrexate in refractory cases
- Meniere's disease:
- Acute attacks: Vestibular suppressants (meclizine, diazepam), antiemetics (prochlorperazine)
- Prophylaxis: Low-sodium diet, diuretics (hydrochlorothiazide/triamterene), betahistine (may improve endolymphatic circulation)
- Surgical: Endolymphatic sac decompression; intratympanic gentamicin (chemical labyrinthectomy); labyrinthectomy; vestibular neurectomy
Rehabilitation/Devices
- Hearing aids: Amplify sound; most suitable for mild-moderate hearing loss; analog or digital (digital preferred - converts sound to numerical code for selective amplification by frequency)
- Cochlear implants: For severe-profound bilateral SNHL; approved for children as young as 12 months. Components: Microphone → speech processor → transmitter/receiver → electrode array → auditory nerve. As of 2012, >324,000 implanted worldwide. Bypass damaged hair cells, directly stimulate spiral ganglion neurons.
- Bone-anchored hearing aids (BAHA): Titanium implant in skull transmits bone-conducted sound; used in conductive/mixed loss and single-sided deafness
- Middle ear implants: Vibrate ossicles directly
Key Clinical Correlations Summary
| Condition | Anatomy/Physiology Basis | Key Test Finding | Treatment |
|---|---|---|---|
| Otosclerosis | Stapes footplate fixation | Negative Rinne; Carhart's notch on audiogram; absent acoustic reflex | Stapedectomy; sodium fluoride; hearing aid |
| Noise-induced HL | OHC damage at 4 kHz region | 4 kHz notch on audiogram; normal OAEs initially then absent | Prevention; hearing protection; cochlear implant if severe |
| Presbycusis | Progressive OHC + neuronal loss | Bilateral symmetric high-freq SNHL | Hearing aids; cochlear implant |
| Acoustic neuroma | CN VIII compression, CPA | Asymmetric SNHL; poor WRS; prolonged ABR wave I-V | Microsurgery or Gamma Knife radiosurgery |
| Meniere's disease | Endolymphatic hydrops | Low-freq SNHL; elevated ECochG SP/AP ratio | Low-salt diet + diuretics + betahistine; IT gentamicin |
| Connexin 26 mutation | K⁺ recycling failure | Congenital bilateral SNHL; autosomal recessive | Cochlear implant (excellent outcomes) |
| Sudden SNHL | Vascular/viral injury to cochlea | Unilateral SNHL >30 dB over ≤72 hrs | Urgent systemic/intratympanic steroids |
| Cisplatin ototoxicity | OHC ROS damage | High-freq bilateral SNHL; absent OAEs | Prevent; amifostine (controversial); cochlear implant |
Recent Evidence (PubMed 2023-2024)
- A 2024 Japanese clinical practice guideline for acute SNHL (PMID 38968877) recommends systemic corticosteroids as standard first-line, with intratympanic steroids for patients who cannot tolerate systemic therapy or as salvage.
- A 2024 meta-analysis (PMID 38506449) on bilateral sudden SNHL found prognosis is worse than unilateral cases, reinforcing the importance of early aggressive treatment.
- COVID-19 is associated with SNHL and tinnitus; an umbrella review (PMID 37093291) found moderate-quality evidence linking SARS-CoV-2 with auditory dysfunction, possibly via vascular/inflammatory mechanisms.
Importance Summary (Exam Focus Points)
- Endocochlear potential (+80 mV) is the driving force for hair cell transduction - maintained by stria vascularis K⁺ pump
- Tonotopy (place principle): High frequencies → base of cochlea; Low frequencies → apex
- Inner hair cells = primary signal generators; Outer hair cells = amplifiers (prestin motor)
- Auditory pathway is bilateral above cochlear nucleus → unilateral central lesions cause minimal hearing loss
- Inferior colliculus = auditory reflex center (startle); superior olive = sound localization (binaural)
- Rinne negative (BC>AC) = conductive loss in that ear
- Weber lateralizes to worse ear in conductive, better ear in SNHL
- 4 kHz notch on audiogram = pathognomonic for noise-induced hearing loss
- Connexin 26 = most common genetic cause of congenital deafness
- Sudden SNHL = medical urgency - treat within 2 weeks with steroids for best outcomes
- Aminoglycosides + loop diuretics = synergistic ototoxicity - avoid combination
- Cochlear implants work by directly stimulating spiral ganglion neurons, bypassing all hair cells
This is a shared conversation. Sign in to Orris to start your own chat.