labor delivery ectopic pregnancy molar pregnancy miscarriages abruption previa Pas anatomy hypertensive. disorders during pregnancy detail information according to Williams obstetrics book
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
All 10 topics covered. Here are a few high-yield clinical pearls to complement the detailed content above:
High-Yield Clinical Pearls
Labor
- Active phase now defined as beginning at 6 cm (not 4 cm) per contemporary evidence — do not diagnose active-phase arrest before 6 cm
- Prolonged latent phase is not an indication for cesarean section
- Maternal obesity significantly slows labor — allow extra time before labeling dystocia
Ectopic Pregnancy
- A single hCG level can never exclude ectopic; serial levels are essential
- hCG discriminatory zone (1,500–2,000 IU/L): if above this and no IUP seen on TVS → high suspicion for ectopic
- 20% of ectopic patients are hemodynamically unstable on presentation → don't delay surgical intervention
Molar Pregnancy
- Preeclampsia before 24 weeks is virtually pathognomonic for molar pregnancy
- Always avoid pregnancy for 1 year after complete mole to allow reliable hCG monitoring
Abruption vs. Previa
| Abruption | Previa | |
|---|---|---|
| Pain | Yes (uterine tenderness) | No (painless) |
| Bleeding color | Dark | Bright red |
| Uterine tone | Rigid/hypertonic | Soft |
| US diagnosis | Low sensitivity | High sensitivity |
PAS
- Risk of accreta with placenta previa + 3 prior cesareans = up to 61%
- Attempting manual placental removal → catastrophic hemorrhage
- Planned cesarean hysterectomy with placenta left in situ is the definitive treatment
Hypertensive Disorders
- MgSO₄ prevents seizures in preeclampsia — it is not an antihypertensive
- First sign of MgSO₄ toxicity: loss of deep tendon reflexes (at ~7–10 mg/dL)
- Respiratory arrest at ~15 mg/dL; cardiac arrest at ~20 mg/dL
- ACE inhibitors and ARBs are absolutely contraindicated in pregnancy
- HELLP can present without severe HTN or proteinuria — always check LFTs and platelets in any pregnant patient with RUQ/epigastric pain
What is Pas when it occurs and when female should convince detail information according to William obstetrics
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Excellent — I now have very detailed content from Creasy & Resnik's, Miller's Anesthesia, and Grainger & Allison's radiology on PAS. I also have the specific risk table. Let me now compile the complete, detailed answer.
Note: Williams Obstetrics is not in this digital library. The information below comes from Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (the most comparable authoritative reference), supplemented by Miller's Anesthesia and Grainger & Allison's Diagnostic Radiology — all of which cover PAS in equivalent or greater depth.
Placenta Accreta Spectrum (PAS) — Comprehensive Detail
DEFINITION
Placenta accreta spectrum (PAS) — formerly called "morbidly adherent placenta" — is abnormal invasion of trophoblasts (placental tissue) into or through the myometrium beyond the normal boundary established by the Nitabuch fibrinoid layer (the normal decidua basalis). In PAS, the decidua basalis is absent or deficient, so nothing stops the placenta from attaching directly to or invading the uterine muscle.
"Placenta accreta occurs when trophoblast is attached to the myometrium without intervening decidua; that is, invasion beyond the normal boundary established by the Nitabuch fibrinoid layer." — Creasy & Resnik's Maternal-Fetal Medicine
THREE DEGREES OF INVASION
| Type | Invasion | Frequency |
|---|---|---|
| Placenta Accreta | Placenta and myometrium in direct contact (no invasion through it) | 82–84% |
| Placenta Increta | Placenta invades into the full thickness of the myometrium but not beyond the serosa | 12–13% |
| Placenta Percreta | Placenta penetrates through the uterine serosa and may invade adjacent organs (bladder, bowel, ovaries, other pelvic structures) | 3–6% |
Important: PAS is not homogeneous — foci of accreta, increta, and percreta can coexist in the same placenta.
WHEN DOES PAS OCCUR? (Incidence & Pathogenesis)
Incidence
- Affects approximately 1 in 300–500 pregnancies
- In developed countries: ~0.17–0.34% of deliveries
- Incidence has risen 10-fold over the past 50 years, driven almost entirely by the rising cesarean delivery rate
Why Does It Happen?
The fundamental mechanism is defective decidualization at a site of prior uterine injury:
- Normal uterine surgery (especially cesarean section) creates a scar in the lower uterine segment
- The scar disrupts the normal endometrial-myometrial interface
- When the placenta implants over this scar, there is absent or deficient decidua basalis (the normal barrier layer)
- Without the Nitabuch layer, trophoblasts invade directly into myometrium — or beyond
- The degree of invasion depends on the depth and extent of the defect
Other contributing mechanisms:
- Abnormal trophoblast biology (excessive invasive tendency)
- Uterine tissue remodeling that exposes vascular myometrium to implantation
- The lower uterine segment has inherently thinner decidua — making it especially vulnerable
RISK FACTORS — WHEN IS A WOMAN AT RISK?
Primary Risk Factors
The single most important combination: Placenta previa + prior cesarean delivery
Risk Table (% Risk of Placenta Accreta by Prior Cesareans + Previa Status)
| Prior Cesareans (Pregnancy Number) | With Placenta Previa | Without Placenta Previa |
|---|---|---|
| 1st cesarean (primary) | 3.3% | 0.03% |
| 2nd cesarean | 11% | 0.2% |
| 3rd cesarean | 40% | 0.1% |
| 4th cesarean | 61% | 0.8% |
| 5th cesarean | 67% | 0.8% |
| ≥6th cesarean | 67% | 4.7% |
From Society for Maternal-Fetal Medicine (SMFM), cited in Creasy & Resnik's Maternal-Fetal Medicine
A woman with 3 prior cesareans and a current placenta previa has a >60% chance of PAS.
Additional Risk Factors
- Prior uterine curettage (D&C) — damages the endometrial lining
- Prior myomectomy (especially if uterine cavity entered)
- Endometrial ablation
- Prior uterine rupture or repair
- Pelvic radiation
- In vitro fertilization (IVF)
- Short interpregnancy interval
- Advanced maternal age
- Smoking, increased parity
WHEN TO SUSPECT PAS — CLINICAL SCENARIOS
A woman should be suspected of having PAS and evaluated accordingly when she has any combination of the following:
High Suspicion Criteria
- Placenta previa in a woman with ≥1 prior cesarean — this is the highest-risk scenario
- Placenta overlying or near a prior uterine scar (even without previa)
- Prior D&C or uterine surgery + anterior low-lying placenta
- Unexplained painless vaginal bleeding in a woman with prior cesarean
- Abnormal ultrasound findings at routine anatomy scan (see Imaging below)
DIAGNOSIS
Timing
- Ideally diagnosed prenatally (2nd trimester anatomy scan or earlier in high-risk patients)
- First-trimester diagnosis is possible and accurate, especially in cesarean scar ectopic pregnancy (the precursor lesion)
- All women with clinical risk factors should be referred for obstetric ultrasound at a unit with appropriate expertise
Ultrasound (Primary Diagnostic Tool)
Sensitivity ~80–93%; Specificity ~71–97% (varies by center expertise)
Important caveat: When experts were blinded to clinical status, sensitivity was only 55% — features of accreta can be present in normal placentas.
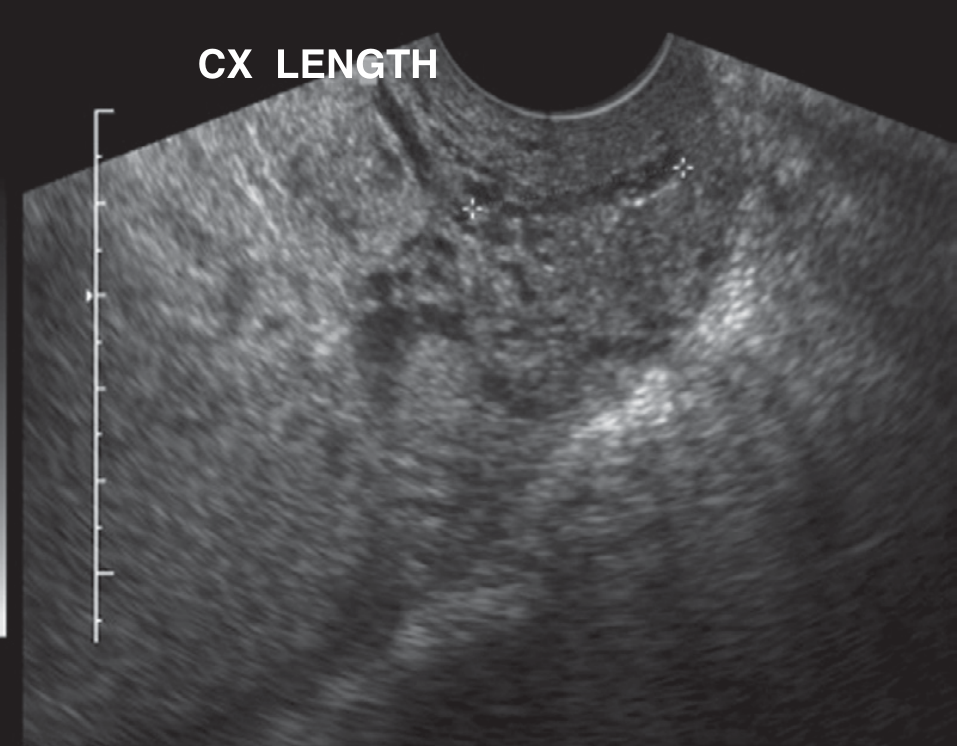
Key Ultrasound Markers (SMFM Consensus Definitions)
| Marker | Finding |
|---|---|
| Loss of hypoechoic zone | Absence of the normal retroplacental "clear zone" (represents decidua basalis) between placenta and myometrium |
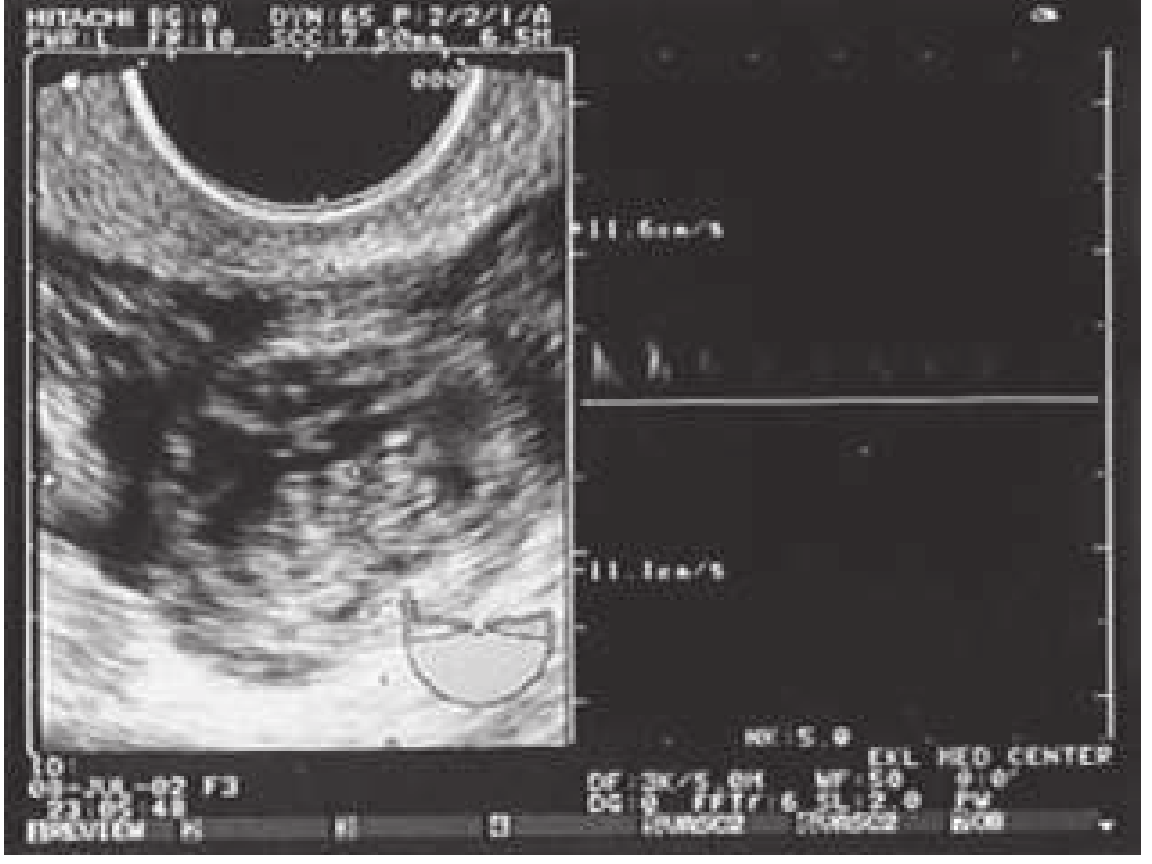
| Placental lacunae | Irregular, hypoechoic ("Swiss cheese") spaces within the placenta containing turbulent vascular flow; large size + irregular borders + high velocity (>15 cm/s) = high risk |
| Abnormal uteroplacental interface | Thinning of retroplacental myometrium (<1 mm), partial or complete interruption along posterior bladder wall |
| Bridging vessels | Vessels extending from placenta across the myometrium and beyond the uterine serosa ("tornado vessels" with multidirectional flow) |
| Placental bulge | Placental tissue distorting and bulging the uterine contour outward |
| Exophytic mass | Placental tissue extruding beyond the uterine serosa |
| Bladder wall interruption | Loss of integrity of posterior bladder wall (suggests percreta with bladder invasion) |
| Turbulent color Doppler flow | Increased, disorganized vascularity at the placenta-uterus interface |
US features by type (most common):
- Accreta: Bridging vessels (71%)
- Increta/Percreta: Placental lacunae + loss of hypoechoic zone + bladder tenting
"The same sonographic features may be identified as early as the first trimester. First-trimester diagnosis is particularly accurate in the setting of cesarean scar ectopic pregnancy." — Creasy & Resnik's Maternal-Fetal Medicine
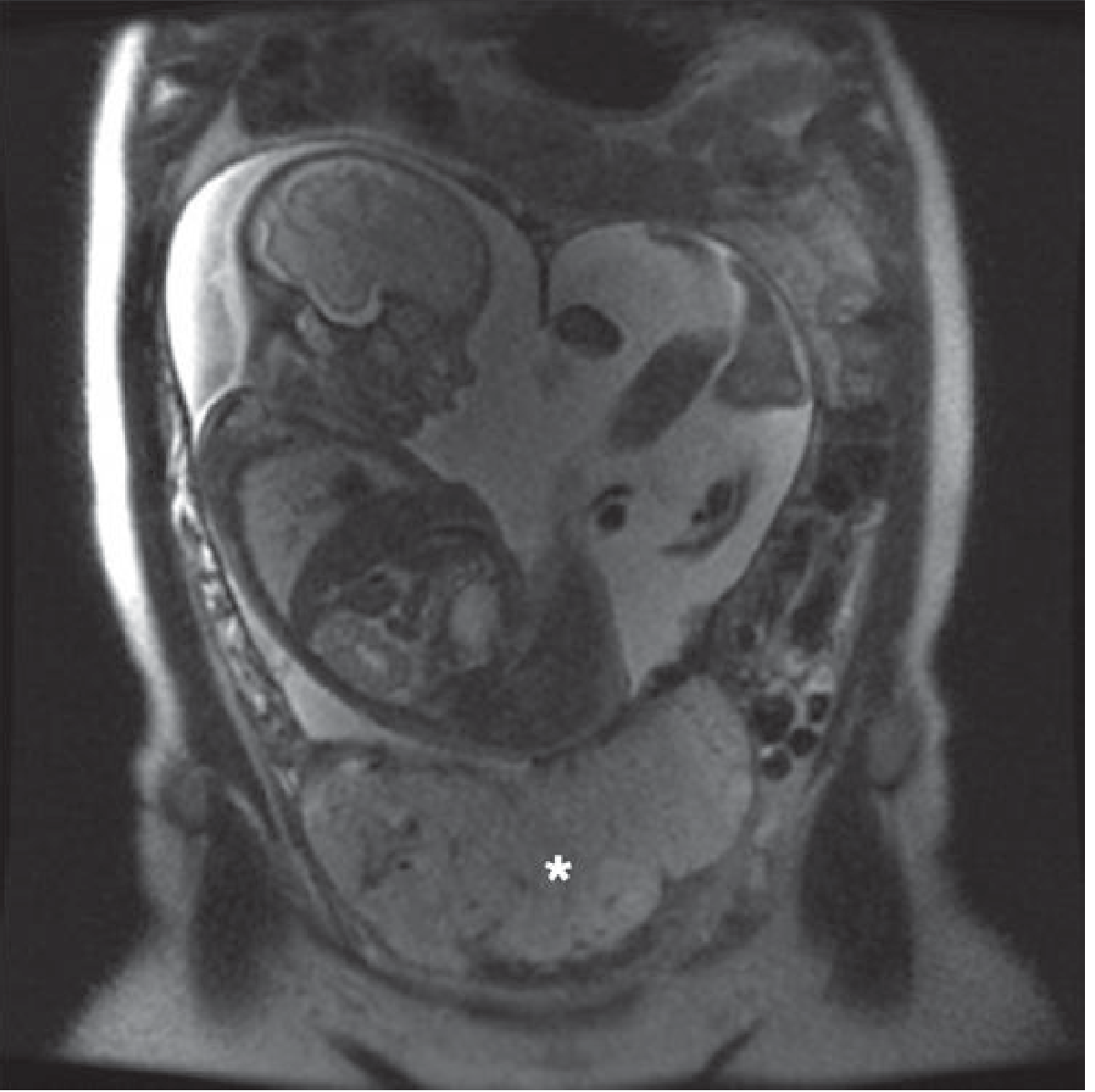
MRI
- Adjunct to ultrasound — especially useful for:
- Posterior placentas (ultrasound poorly visualizes posterior wall)
- Assessing depth of invasion (increta vs. percreta)
- Bladder or parametrial involvement
- When ultrasound findings are inconclusive
- MRI features: heterogeneous placental signal, uterine bulge, myometrial thinning (<1 mm) or focal interruption, low T2 signal intensity intraplacental bands, disorganized placental vasculature, loss of uteroplacental zone, bladder tenting/invasion
- Sensitivity ~80%; Specificity ~65% (slightly lower than good-quality ultrasound)
- Combined US + MRI sensitivity: 93%
- No gadolinium contrast required; MRI without gadolinium is safe in pregnancy at any trimester
CLINICAL CONSEQUENCES AND COMPLICATIONS
What Happens at Delivery (if Undiagnosed or Unprepared)
At delivery, the placenta does not separate from the uterine wall normally. Attempts at manual extraction cause the placenta to fragment without complete separation → massive, uncontrollable hemorrhage → life-threatening emergency.
Major Complications
| Complication | Detail |
|---|---|
| Massive hemorrhage | Primary danger; average blood loss 3–5 L; can exceed 10 L |
| DIC | From massive hemorrhage consuming clotting factors |
| Peripartum hysterectomy | PAS is the most common indication for emergency peripartum hysterectomy |
| Bladder/ureter injury | Especially with percreta |
| Maternal death | Overall ~3%; rises to ~20% with bladder involvement (percreta) |
| Preterm birth | From iatrogenic early delivery or bleeding episodes |
| Fetal growth restriction | OR = 5.05 compared with controls |
WHEN SHOULD DELIVERY OCCUR? (Timing of Delivery)
This is a critical management decision. The goal is to deliver before onset of labor or uncontrolled bleeding — both of which dramatically increase hemorrhagic risk.
Recommended Timing
| Clinical Scenario | Recommended Delivery Gestation |
|---|---|
| Suspected/confirmed PAS (accreta/increta) | 34–35 weeks after corticosteroids for fetal lung maturity |
| PAS with bladder or organ involvement (percreta) | 34–36 weeks (some centers 34 weeks given bleeding risk) |
| Antenatally diagnosed, stable | Elective cesarean at 34–35 weeks (Creasy & Resnik) or 34–36 weeks (Miller's; SMFM) |
| Onset of labor or uncontrolled bleeding | Emergency delivery regardless of gestation |
"We plan for delivery at 34 to 35 weeks after maternal corticosteroid administration. With this approach, our neonatal outcomes have been favorable. Delivery is performed without amniotic fluid confirmation of fetal lung maturity." — Creasy & Resnik's Maternal-Fetal Medicine
Why not wait until term?
- Risk of massive hemorrhage increases as pregnancy advances and vascularity increases
- Unplanned emergency delivery (in labor or with acute hemorrhage) carries dramatically higher morbidity/mortality than planned elective surgery
- Corticosteroids (betamethasone) administered 48 hours before planned delivery to promote fetal lung maturity at 34–35 weeks
Counseling Before Delivery
Women should be counseled about:
- Planned cesarean hysterectomy as the definitive procedure (placenta left in situ)
- Expected massive blood loss requiring transfusion
- Risk of hysterectomy (loss of fertility)
- Risk of urologic injury (bladder, ureter — especially percreta)
- Possible ICU admission
- Neonatal prematurity and NICU stay
- Option of conservative management (uterus-sparing) and its risks
WHEN SHOULD CONSERVATIVE (UTERUS-SPARING) MANAGEMENT BE CONSIDERED?
Some women strongly desire preservation of fertility. Conservative management (leaving the placenta in situ with the uterus preserved) may be considered in:
Appropriate Candidates for Conservative Management
- Small, focal accreta (not extensive)
- Fundal location (after myomectomy or classic cesarean) — away from the bladder
- Posterior placenta (where hysterectomy is technically more complex)
- Strong patient desire to preserve fertility after thorough counseling
- Hemodynamically stable patient
Conservative Management Protocol
- Fundal hysterotomy (avoiding the placenta) → deliver baby → clamp cord
- Placenta left completely in situ — do NOT attempt removal
- Uterus closed
- Uterine artery embolization (UAE) postoperatively (most common adjunct)
- Serial hCG monitoring and imaging to track placental resorption
- Methotrexate is NOT recommended — no proven efficacy + risk of complications (including death reported)
Outcomes of Conservative Management
- 18 of 167 women required primary hysterectomy for intraoperative bleeding
- Another 18 required delayed hysterectomy
- Severe morbidity in 10 women; 1 death from methotrexate complications
- Of 15 subsequent pregnancies: 6 first-trimester losses, 4 preterm births, 2 recurrent accretas
- Risk may be higher in true histologically confirmed accretas (many conservative cases lacked histologic confirmation)
"Conservative management should be undertaken with extreme caution and appropriate counseling regarding risks." — Creasy & Resnik's Maternal-Fetal Medicine
DEFINITIVE MANAGEMENT — CESAREAN HYSTERECTOMY
Where: Center of Excellence (Level III or IV Maternal Care Facility)
"Outcomes are improved and the chances of complications diminished when accretas are managed at regional referral centers or 'centers of excellence.'" — Creasy & Resnik's Maternal-Fetal Medicine
Multidisciplinary Team Required
- Maternal-Fetal Medicine (MFM) specialist
- Experienced pelvic/gynecologic oncology surgeon (capable of wide resection)
- Urology (if bladder involvement expected)
- Interventional Radiology (IR)
- Anesthesiology (obstetric anesthesia team)
- Blood bank / Transfusion medicine (massive transfusion protocol)
- Neonatology
- ICU team
Surgical Steps
- Fundal hysterotomy (classical/vertical incision avoiding the placenta) → deliver baby
- Cord clamped immediately
- Placenta left completely in situ (no attempt to remove it)
- Proceed to total abdominal hysterectomy with placenta inside
- Wide resection of lower uterine segment and parametrial tissues as needed
- Bladder dissection if percreta with bladder involvement
Blood Loss Reduction Strategies
- Cell salvage (autotransfusion) intraoperatively
- Massive transfusion protocol (packed RBCs + FFP + platelets in 1:1:1 ratio)
- Balloon occlusion of internal iliac arteries, common iliac arteries, or aorta:
- Preoperative IR placement of balloon-tipped catheters retrograde
- Inflated just before uterine incision to reduce pelvic blood flow
- Reduces blood loss during resection of lower uterine segment
- Efficacy varies; preferred: common iliac balloons (cover most extrauterine supply)
- Caution: uterine artery balloon inflation before delivery can cause fetal anoxia
- Selective embolization of uterine vessels near time of delivery
SUMMARY: KEY CLINICAL POINTS
| Question | Answer |
|---|---|
| What is PAS? | Abnormal trophoblast attachment/invasion into or through the uterine myometrium |
| When does it occur? | Most common when placenta previa overlies a prior cesarean scar |
| Highest risk situation? | Placenta previa + ≥3 prior cesareans → >60% risk of accreta |
| When to suspect it? | Any prior C/S with anterior low-lying/previa placenta; abnormal US |
| When to diagnose? | 2nd trimester ultrasound in all at-risk women; MRI as adjunct |
| When to deliver? | 34–35 weeks gestation — planned, elective, before labor begins |
| How to deliver? | Planned cesarean hysterectomy; placenta left in situ; multidisciplinary team |
| When to consider conservative Rx? | Focal accreta, fundal location, strong desire for fertility, after thorough counseling |
| Leading complication? | Massive hemorrhage → DIC; most common cause of peripartum hysterectomy |
| Maternal mortality? | ~3% overall; up to 20% if bladder involved (percreta) |
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Miller's Anesthesia, 10th ed.; Grainger & Allison's Diagnostic Radiology; Textbook of Family Medicine, 9th ed.
Abruptions
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from Creasy & Resnik's (the primary source), Rosen's Emergency Medicine, and Textbook of Family Medicine. Here is the full detailed response:
Source note: Williams Obstetrics is not available in this digital library. All content below is drawn from Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (the authoritative equivalent) and corroborated by Rosen's Emergency Medicine and Textbook of Family Medicine, 9th ed.
Placental Abruption (Abruptio Placentae) — Complete Detailed Reference
DEFINITION
Abruptio placentae is the premature separation of a normally sited placenta from the uterine wall before delivery of the fetus, after 20 weeks' gestation.
It is distinguished from placenta previa by the fact that the placenta is normally implanted — the problem is not location, but early, pathological detachment.
"Abruptio placentae is the premature separation of a normally sited placenta before birth, after 20 weeks' gestation. It is a particularly hazardous condition associated with significant maternal and fetal morbidity and mortality." — Creasy & Resnik's Maternal-Fetal Medicine
INCIDENCE AND EPIDEMIOLOGY
| Statistic | Value |
|---|---|
| Clinically recognized abruption | ~1% of all pregnancies (1 in 100) |
| Subclinical (found on placental exam) | ~4% of all deliveries |
| Abruption causing fetal death | ~1 in 420 deliveries |
| Peak gestational age of incidence | 24–26 weeks (spontaneous highest here) |
| Contribution to preterm births | ~10% of all preterm births |
| Rate increase in US in recent decades | ~25% increase in clinically detected abruption; disproportionately higher in Black women |
Key point: most subclinical (minor, marginal) abruptions are never recognized and have no clinical consequence — they are found only on placental examination after delivery.
PATHOGENESIS — HOW DOES IT HAPPEN?
The Core Mechanism

- Hemorrhage occurs between the decidua basalis and the placenta (retroplacental hematoma)
- The hematoma dissects the decidua apart → progressively separates the placenta from the uterine wall
- The separated area loses its function — no gas exchange, no fetal nutrition in that zone
- Process may be self-limited (minor separation, small hematoma) or progressive (expanding hematoma → greater separation → fetal compromise)
How Bleeding Presents
- External (revealed) bleeding: dissection reaches the placental edge, tracks between the fetal membranes and uterine wall, exits through the cervix → visible vaginal bleeding
- Concealed (occult) bleeding: blood is trapped behind the placenta — no external bleeding despite massive internal hemorrhage
- Mixed: combination of both (most common)
Underlying Vascular Events
- Primary cause: vasospasm of abnormal maternal arterioles in the decidua
- Some cases: venous hemorrhage into areas of necrotic decidua secondary to thrombosis
- Evidence of preexisting placental pathology: poor trophoblastic invasion, abnormal uterine artery Doppler flow, inadequate spiral artery remodeling — all linking abruption to preeclampsia and IUGR as a common placental disorder
- Marker: women destined to have abruption have low levels of pregnancy-associated plasma protein A (PAPP-A) — may be detected at first-trimester screening
Couvelaire Uterus
When abruption is severe and extensive:
- Retroplacental blood penetrates the full thickness of the myometrium into the peritoneal cavity
- Myometrium becomes infiltrated with blood → purple, bruised, board-like uterus (Couvelaire uterus / uteroplacental apoplexy)
- Myometrium becomes weakened and atonic → risk of uterine rupture (rare) and postpartum hemorrhage
- In near-complete or complete abruption with Couvelaire uterus → fetal death is inevitable without immediate cesarean delivery
DIC Cascade
As abruption expands:
- Massive hemorrhage activates the coagulation cascade
- Ongoing bleeding → consumption of clotting factors → DIC
- Maternal hypovolemia + poor tissue perfusion → aggravates DIC
- Downward spiral: hemorrhage → DIC → more bleeding → hemorrhagic shock
RISK FACTORS
Strongest Risk Factors
| Risk Factor | Relative Risk / Detail |
|---|---|
| Prior abruption | Up to 20-fold increased risk; with two prior abruptions → 25% recurrence risk |
| Chronic hypertension | 5-fold increase; 8-fold with superimposed preeclampsia |
| Preeclampsia | Strongly linked; shared pathologic mechanisms |
| Cocaine use | Vasospasm → acute hypertension → abruption; up to 10% of cocaine users in pregnancy experience abruption |
| Cigarette smoking | Up to 2.5× increased risk; dose-response relationship; doubles perinatal mortality; risk elevated even if smoking stopped before pregnancy |
Additional Risk Factors
| Risk Factor | Mechanism / Detail |
|---|---|
| Maternal age <20 or >35 | Both extremes associated |
| Parity ≥3 | Small but positive correlation |
| Maternal trauma | Shearing of non-elastic placenta from elastic uterine wall; MVAs most common traumatic cause; abruption may not be apparent for up to 24 hours after trauma |
| Intimate partner violence | Affects 4–8% of pregnancies; torso injuries in 21.5% of IPV cases |
| Uterine fibroids | ~Doubles the risk of abruption |
| Thrombophilias | Hyperhomocysteinemia established association; Factor V Leiden — unclear |
| Sudden uterine decompression | Delivery of first twin, membrane rupture in polyhydramnios |
| Premature rupture of membranes (pPROM) | Strongly associated (both causal and consequential) |
| Subchorionic hematoma (SCH) early pregnancy | Increased risk of later abruption |
| Alcohol use | Associated |
| Retroplacental needle puncture | (e.g., from amniocentesis) |
| Low PAPP-A (<5th percentile) at 1st trimester screen | Marker of increased abruption risk |
| Abnormal uterine artery Doppler (11–14 weeks) | Elevated resistance associated with increased risk |
"The most important risk factor for abruption is a history of abruption in a prior pregnancy." — Creasy & Resnik's Maternal-Fetal Medicine
"40–50% of women with abruptio placentae have underlying hypertension." — Textbook of Family Medicine 9e
CLINICAL CLASSIFICATION — SEVERITY SPECTRUM
Abruption covers a broad clinical spectrum, from subclinical to catastrophic:
Grade 0 — Subclinical / Asymptomatic
- No symptoms
- Retroplacental clot identified only on placental examination after delivery
- No maternal or fetal compromise
Grade 1 — Mild Abruption
- Slight vaginal bleeding (may be absent — concealed)
- Mild uterine tenderness, little or no irritability
- No fetal distress
- Normal maternal vital signs
- Normal coagulation studies
- No maternal hemodynamic instability
Grade 2 — Moderate Abruption
- Moderate vaginal bleeding (or significant concealed hemorrhage)
- Increased uterine irritability ± tetanic contractions
- Fetal distress present (FHR abnormalities)
- Maternal tachycardia
- Declining fibrinogen levels
- No overt maternal shock
Grade 3 — Severe Abruption (~15% of cases)
- Massive bleeding (overt or concealed) → maternal hypotension/shock
- Tetanically contracted, extremely painful, board-like uterus
- Fetal death
- Fibrinogen <150 mg/dL (overt DIC)
- Maternal coagulopathy
- Risk of Couvelaire uterus, renal cortical necrosis, pituitary necrosis (Sheehan syndrome)
"Massive, concealed abruption often manifests with severe pain, a hard tonically contracting uterus, and a dead fetus; such a picture may occur in association with severe preeclampsia or recent use of cocaine." — Creasy & Resnik's Maternal-Fetal Medicine
CLINICAL FEATURES — SIGNS AND SYMPTOMS
| Feature | Frequency |
|---|---|
| Vaginal bleeding (dark, may be scanty despite large concealed bleed) | 70–80% |
| Uterine/abdominal pain and tenderness | 66% |
| Fetal distress | 60% |
| Uterine contractions (often 1–2 min apart, elevated baseline tone) | ~33% |
| Back pain (posteriorly located placenta) | Variable |
| Occult (concealed only — no external bleeding) | ~10–20% |
| Nausea, vomiting | Variable |
Special Presentations
- Posterior placenta: severe back pain may be the only symptom; worsened by anterior abdominal palpation pushing fetus into placenta
- Idiopathic preterm labor: abruption should always be considered when no other cause for preterm labor is found
- Traumatic abruption: may have no symptoms for up to 24 hours after trauma (MVA, fall, IPV)
- Chronic abruption-oligohydramnios sequence (CAOS): recurrent bleeding from chronic retroplacental bleeding → oligohydramnios develops without evidence of ruptured membranes; all patients deliver preterm (average 28 weeks)
Critical point: The amount of visible vaginal bleeding is an unreliable guide to the severity of abruption. A woman with minimal external bleeding may have massive concealed hemorrhage.
DIAGNOSIS
Primary: Clinical Diagnosis
"Abruptio placentae is a clinical diagnosis. Painful vaginal bleeding in the third trimester is the hallmark." — Textbook of Family Medicine 9e
No single test confirms abruption. Diagnosis rests on the clinical picture: bleeding + pain + uterine tenderness + contractions + fetal distress.
Ultrasound
- Primary role: exclude placenta previa (not confirm abruption)
- Sensitivity for abruption: low — at least 50% of abruptions produce NO findings on ultrasound
- Fresh blood is isoechoic or hyperechoic relative to the placenta → invisible in acute phase
- As hematoma ages (over days): becomes hypoechoic → sonolucent (typically by 2 weeks)
- "Jello sign": intrauterine clot jiggles when bounced by the transducer
- Absence of US findings never excludes abruption
Cardiotocography (CTG / Electronic Fetal Monitoring)
- Most sensitive test for detecting fetal compromise
- 100% negative predictive value for adverse outcomes when monitoring is reassuring
- FHR abnormalities: variable decelerations, late decelerations, poor variability, prolonged bradycardia, sinusoidal pattern → reflect fetal asphyxia
- Uterine contractions may be present that are not clinically felt — especially post-trauma
- Should begin immediately and be continuous
Laboratory Studies — Complete Panel
| Test | Normal Value in Pregnancy | Significance in Abruption |
|---|---|---|
| Fibrinogen | 400–650 mg/dL | Usually decreased; <200 mg/dL = severe DIC; <150 mg/dL = severe abruption |
| Fibrin degradation products (FDP) | <10 µg/mL | Almost always elevated; most sensitive lab test for DIC |
| Platelet count | >140,000/mm³ | Usually decreased with severe abruption |
| PT/PTT | PT 10–12s; PTT 24–38s | Normal to prolonged |
| Thrombin time | 16–20s | Parallels fall in fibrinogen; good marker of severity |
| Whole blood clotting time | Clot in 4–8 min | Abnormal clot formation = severe factor deficiency |
| D-dimer | Elevated | Elevated in DIC |
| RBC morphology | Normal | Fragmentation/schistocytes = microangiopathic hemolysis → risk of renal cortical necrosis |
| Hemoglobin / Hematocrit | Baseline | Monitor for blood loss |
| Kleihauer-Betke | Negative | Not diagnostic of abruption (may be negative with proven abruption); only useful to guide Rh immune globulin dosing in Rh-negative women |
"Fibrin degradation products are almost always elevated — the most sensitive lab test." "The wall clot test: take blood in a tube — if it doesn't clot in 6 minutes or the clot lyses within 30 minutes → severely abnormal coagulation."
FETAL AND NEONATAL CONSEQUENCES
| Outcome | Detail |
|---|---|
| Fetal distress / death | ~15% of abruptions; risk proportional to percentage of placental surface involved and rapidity of separation |
| If >50% placenta involved | Fetal death is likely |
| Perinatal asphyxia | Increased vs. gestational age-matched controls |
| Intraventricular hemorrhage (IVH) | Higher rates in survivors |
| Periventricular leukomalacia | Higher rates |
| Cerebral palsy | Higher rates |
| IUGR | Most pregnancies with abruption deliver infant weighing <10th percentile — suggests shared pathology (placental dysfunction) |
| Preterm birth | 10% of all preterm births caused by abruption |
| Fetomaternal transfusion | Can occur with abruption → check Kleihauer-Betke in Rh-negative |
"20% of all fetal deaths from abruption occur after presentation to the hospital, and 30% of those deaths occur within 2 hours after admission." — Creasy & Resnik's Maternal-Fetal Medicine
MATERNAL COMPLICATIONS
| Complication | Detail |
|---|---|
| Hemorrhagic shock | From blood loss (visible + concealed) |
| DIC | From massive decidual hemorrhage releasing thromboplastin; fibrinogen consumption |
| Couvelaire uterus | Myometrial blood infiltration → atonic uterus → PPH |
| Postpartum hemorrhage (PPH) | From atonic Couvelaire uterus |
| Acute renal failure / renal cortical necrosis | From prolonged hypoperfusion + DIC microthrombi |
| Sheehan syndrome | Pituitary necrosis from severe/prolonged shock (rare) |
| Amniotic fluid embolism | Placental separation predisposes |
| Maternal death | From coagulopathy or exsanguination |
DIFFERENTIAL DIAGNOSIS
| Diagnosis | Distinguishing Features |
|---|---|
| Placenta previa | Painless, bright red bleeding; soft uterus; confirmed by US |
| Uterine rupture | Sudden cessation of contractions; fetal parts palpable abdominally; hypovolemia |
| Preeclampsia complication | May coexist; check for HTN, proteinuria, RUQ pain |
| Preterm labor | Contractions but no uterine tenderness or bleeding, normal FHR |
| Pyelonephritis | Fever, costovertebral angle tenderness, no bleeding |
| Appendicitis | RLQ pain, no bleeding, no uterine tenderness diffusely |
| Ovarian torsion | Adnexal mass, no uterine tenderness |
| Cervical/vaginal lesion | Bright red blood from os; no uterine tenderness; US normal |
"All patients with painless second-trimester vaginal bleeding should be assumed to have placenta previa until proven otherwise by ultrasound before considering abruption."
MANAGEMENT
Guiding Principle
"The key to optimizing maternal and fetal outcomes in abruptio placentae is the individualization of care. Precise management depends on the extent of maternal and fetal compromise and the gestational age." — Creasy & Resnik's Maternal-Fetal Medicine
Immediate Stabilization — All Cases
- Two large-bore IV lines (large-gauge; central line or arterial line if hemodynamically unstable)
- Continuous electronic fetal monitoring — start immediately, maintain continuously
- Indwelling urinary catheter — to monitor urine output closely (target >30 mL/hr)
- Supplemental oxygen
- Left lateral tilt (reduce aortocaval compression)
- Obstetric team + anesthesia notified immediately
Laboratory Workup
- CBC with platelets
- Type and crossmatch
- PT, PTT, fibrinogen, thrombin time, FDP/D-dimer
- BMP (renal function)
- Wall clot test (bedside: blood in red-top tube → should clot within 6 min)
- Kleihauer-Betke (only for Rh dosing, not diagnosis)
- Baseline fibrinogen is the most important serial monitor
Imaging
- Ultrasound: exclude placenta previa; may or may not show retroplacental clot
- CTG: begin immediately; most sensitive indicator of fetal status
Decision Tree Based on Clinical Scenario
Scenario 1: Severe Abruption (Grade 3) — Any Gestation
→ Immediate delivery
- Usually by emergency cesarean section — unless patient is in advanced active labor with imminent vaginal delivery
- Massive transfusion protocol:
- Packed RBCs
- Fresh frozen plasma (FFP) — replace clotting factors
- Platelets (if <50,000 or actively bleeding)
- Cryoprecipitate (if fibrinogen <200 mg/dL)
- Fibrinogen concentrate if available
- Target fibrinogen >200 mg/dL to reduce bleeding
- Treat DIC aggressively
- If Couvelaire uterus → at risk for uterine atony postoperatively → have oxytocin, ergometrine, carboprost ready
- If Rh-negative → administer Rh immune globulin 300 µg within 72 hours
Scenario 2: Moderate/Severe Abruption with Fetal Compromise — Any Gestation
→ Immediate delivery (cesarean)
- Do not delay for steroid administration
- Same resuscitation as above
Scenario 3: Abruption ≥34 Weeks — Stable Mother, No Severe Fetal Distress
→ Deliver without delay
"If the event occurs after 34 weeks' gestation, delivery should not be delayed, because the risks of conservative management outweigh any considerations of prematurity." — Creasy & Resnik's Maternal-Fetal Medicine
- Route: vaginal if labor progressing and fetal status allows; cesarean if indicated
- Amniotomy often performed — confirms bleeding is not from previa, may hasten labor, allows IUPC placement
Scenario 4: Abruption 20–34 Weeks — Stable Mother AND Fetus
→ Cautious conservative management (expectant)
- Hospital admission mandatory
- Continuous CTG monitoring
- Serial laboratory work (fibrinogen q4–6h)
- Betamethasone 12 mg IM × 2 doses 24 hours apart for fetal lung maturity
- Serial growth ultrasounds + Doppler studies
- Tocolysis: use with extreme caution (magnesium sulfate if needed for lung maturity/neuroprotection; avoid beta-agonists which can mask tachycardia of blood loss)
- Patient counseled re: risk of evolving abruption — may need emergency delivery at any time
"The patient should be monitored closely because she continues to be at risk of an evolving process."
Scenario 5: Post-Trauma (MVA, Fall, IPV) — Any Gestation
- Asymptomatic after trauma: CTG monitoring for minimum 6 hours; if reassuring → can discharge
- Bleeding or contractions after trauma: monitor for at least 24 hours; abruption may be delayed in presentation
- Kleihauer-Betke for Rh dosing
- Serial fibrinogen and coagulation studies
Coagulation Management Table
| Finding | Action |
|---|---|
| Fibrinogen 200–400 mg/dL | Monitor closely; serial levels every 2–4 hours |
| Fibrinogen 100–200 mg/dL | Cryoprecipitate (each unit raises fibrinogen ~10 mg/dL); FFP |
| Fibrinogen <100 mg/dL | Massive DIC — cryoprecipitate + FFP + platelets + urgent delivery |
| Platelets <50,000 + bleeding | Platelet transfusion |
| Prolonged PT/PTT | FFP (10–15 mL/kg) |
| Elevated FDP + low fibrinogen | Overt DIC — treat aggressively |
RECURRENCE AND COUNSELING
| Situation | Recurrence Risk |
|---|---|
| One prior abruption | Up to 20-fold increased risk vs. general population |
| Two prior abruptions | ~25% recurrence risk |
Counseling Points for Future Pregnancies
- Risk of recurrence is substantial — must be disclosed
- Modifiable risk factors should be addressed before conception:
- Stop smoking (even stopping before pregnancy carries some residual risk)
- Avoid cocaine and other vasoactive substances
- Optimize blood pressure control (preconception visit for hypertensive patients)
- Treat thrombophilias (e.g., aspirin for APS)
- Low-dose aspirin (81 mg/day from 12 weeks) — reduces risk in women with prior preeclampsia/abruption through antiplatelet and anti-inflammatory effects
- First-trimester PAPP-A screening and uterine artery Doppler may identify high-risk women earlier
- Early ultrasound surveillance for IUGR, abnormal Doppler
- Antenatal fetal surveillance from 28–32 weeks in women with prior abruption
SUMMARY AT A GLANCE
| Feature | Abruption | Previa |
|---|---|---|
| Pain | Yes — uterine, colicky, constant | No — painless |
| Bleeding color | Dark | Bright red |
| Uterine tone | Rigid/hypertonic | Soft, non-tender |
| Fetal distress | Common | Uncommon initially |
| US diagnosis | Low sensitivity (≥50% miss rate) | High sensitivity |
| Diagnosis method | Clinical | Ultrasound |
| Digital vaginal exam | Allowed (with caution) | Contraindicated |
| Main complication | DIC, hemorrhagic shock, fetal death | Hemorrhage, preterm birth |
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Rosen's Emergency Medicine: Concepts and Clinical Practice; Tintinalli's Emergency Medicine; Textbook of Family Medicine, 9th ed.
Placenta previa
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from all major sources. Here is the complete reference:
Source note: Williams Obstetrics is not in this digital library. Content below is drawn from Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice (primary), Rosen's Emergency Medicine, Morgan & Mikhail's Clinical Anesthesiology, Textbook of Family Medicine 9e, and Grainger & Allison's Diagnostic Radiology — all authoritative peer-level references.
Placenta Previa — Complete Detailed Reference
DEFINITION
Placenta previa occurs when the placenta implants in the lower uterine segment (LUS) such that it covers or lies adjacent to the internal cervical os. It is a leading cause of antepartum hemorrhage.
Modern (Current) Terminology
Traditional subcategories (complete, partial, marginal) are no longer recommended per contemporary consensus.
| Current Term | Definition |
|---|---|
| Placenta previa | Placental edge covers the internal cervical os |
| Low-lying placenta | Placental edge is within ≤2 cm of the internal os but does not cover it |
| Normal placental position | Placental edge is >20 mm from the internal os |
"The previous categories of placenta previa — complete, partial, marginal — are no longer recommended." — Creasy & Resnik's Maternal-Fetal Medicine
However, older classification is still widely used in clinical practice and exams:
| Old Classification | Description |
|---|---|
| Complete (Total) | Placenta completely covers the internal os; ~20% of previas; highest risk of catastrophic hemorrhage |
| Partial | Placenta partially covers the internal os |
| Marginal | Placental edge reaches but does not cover the os |
| Low-lying | Placenta in LUS, within 2 cm of os, but not reaching it |
INCIDENCE
| Statistic | Value |
|---|---|
| Overall incidence | ~1 in 200–250 pregnancies (0.5% of third-trimester pregnancies) |
| Diagnosed on mid-trimester US | ~10% of midtrimester sonograms show apparent previa |
| Resolves before delivery | ~90% of those diagnosed in 2nd trimester resolve by term |
| Incidence increasing | Due to rising cesarean rates, increasing maternal age, and ART |
PATHOGENESIS — WHY DOES IT HAPPEN?
Primary Mechanism
The exact cause is unknown, but two processes explain it:
1. Defective implantation site
- Prior endometrial damage (from curettage, surgery, infection, scarring) → less favorable endometrium in the upper uterus → placenta implants lower where vascularization is accessible
- The LUS has relative endometrial deficiency → abnormally implanted placenta
2. Trophotropism (Placental Growth Toward Better Vascularity)
- The placenta does not physically migrate — it grows preferentially toward better blood supply at the fundus
- Distal portions near the lower segment with poorer blood supply regress and atrophy over time → placenta "moves away" from os
- Simultaneously, differential growth of the LUS pulls the lower placental edge further from the os as pregnancy advances
"The placenta clearly does not move; rather it is likely that the placenta grows toward the better blood supply at the fundus (trophotropism), leaving the distal portions closer to the relatively poor blood supply of the lower segment to regress and atrophy." — Creasy & Resnik's Maternal-Fetal Medicine
Why Does Bleeding Occur?
- As the LUS develops in late pregnancy, the cervix effaces and the lower segment elongates
- Marginal placental sinusoids are torn as the LUS stretches
- Prelabor Braxton-Hicks contractions, cervical dilation, intercourse, or vaginal examination can all provoke bleeding
- Once labor begins, cervical dilation forces progressive placental separation → significant hemorrhage
RISK FACTORS
| Risk Factor | Increased Risk |
|---|---|
| Previous placenta previa | 8× |
| Previous cesarean section | 1.5–15× (increases with each additional C/S) |
| Age >35 years | 4.73× |
| Age >40 years | 9× |
| Previous suction curettage (abortion) | 1.33× |
| Cigarette smoking | 1.4–3.3× |
| Multiparity | 1.1–1.73× |
| Asian race | 1.93× |
| Multiple gestation | Increased (larger placenta) |
| Uterine abnormalities | Increased |
| Prior uterine surgery (myomectomy, etc.) | Increased |
| Infertility treatment / ART | Increased |
| Prior placenta previa | Increased recurrence |
"There is a clear association between placental implantation in the lower uterine segment and prior endometrial damage and uterine scarring from curettage, surgical insult, prior placenta previa, or multiple prior pregnancies." — Creasy & Resnik's Maternal-Fetal Medicine
CLINICAL FEATURES
Classic Presentation
"The classic history for placenta previa is that of painless third-trimester bleeding." — Creasy & Resnik's Maternal-Fetal Medicine
| Feature | Detail |
|---|---|
| Painless vaginal bleeding | Hallmark — bright red, fresh blood |
| Spontaneous onset | No identifiable precipitating cause in most cases |
| Self-limited initially | First bleed usually stops spontaneously — but recurs |
| First bleed timing | Average 27–32 weeks gestation |
| "Herald bleeds" | Several small warning bleeds may precede major hemorrhage |
| No bleeding until labor | Up to 10% of cases have no bleeding until labor begins |
| Abnormal fetal lie | Transverse or breech (placenta occupies lower segment, prevents cephalic engagement) |
| Uterine irritability | ~20% have some, but minor |
Special Presentations
- Complete (central) previa: earlier, more severe bleeding episodes; highest hemorrhage risk
- Posterior previa: may be more difficult to diagnose on transabdominal US; may present with back pain
- Provoked bleeding: after intercourse, speculum examination, or digital vaginal examination
What is NOT Present (distinguishes from Abruption)
- No uterine tenderness
- No hypertonic uterus
- No fetal distress (initially)
- No DIC (unless massive hemorrhage occurs)
DIAGNOSIS
Rule #1 — Critical Safety Point
⚠️ DO NOT perform digital vaginal examination until placenta previa has been excluded by ultrasound. Digital examination can precipitate catastrophic, life-threatening hemorrhage.
Even a speculum exam should be limited to atraumatic partial insertion — only to identify whether blood is coming from the cervical os.
Ultrasound — Diagnostic Method of Choice
Transabdominal Ultrasound (TAS):
- First-line screening tool
- Accuracy 93–98%
- False positives from: full bladder (pushes anterior uterine wall down, mimicking previa), focal uterine contractions
- Inferior to TVS for definitive placental localization
- Posterior placentas difficult to visualize accurately
Transvaginal Ultrasound (TVS) — Gold Standard:
- More accurate than TAS; can precisely measure os-to-placental-edge distance
- Proven safe — concerns about provoking bleeding are unfounded
- Technique: probe inserted under continuous US visualization; avoid placing probe into a dilated cervix; do not advance beyond the lower vagina
- Bladder must be EMPTY — full bladder causes false-positive diagnosis by pushing uterine walls together
- Translabial (transperineal) scanning is an alternative if TVS unavailable
Translabial ultrasound: place abdominal probe on the perineum — good visualization of cervix-placenta relationship; better than TAS
MRI: used in equivocal cases, posterior placentas, or when PAS is suspected alongside previa.
"Double-Setup" Examination
Used only in rare situations where:
- Significant third-trimester bleeding
- Ultrasound unavailable
- Diagnosis not established
Procedure:
- Patient taken to operating room
- Full preparation for immediate cesarean delivery
- Vaginal exam starting at vaginal fornices (not directly at cervix)
- If previa detected → proceed immediately to cesarean
- If no previa → continue evaluating for other bleeding causes
PLACENTAL MIGRATION — RESOLUTION OVER TIME
| Gestational Age | Likelihood of Previa Persisting |
|---|---|
| 16–18 weeks | Very high over-diagnosis on TAS; 10× more diagnosed than ultimately deliver with previa |
| 20–24 weeks (2nd trimester anatomy scan) | 90% of apparent previas will resolve by term |
| 28–32 weeks | Intermediate — may still migrate |
| 36 weeks | Final status for delivery planning |
Factors That Predict Persistence to Term
- Degree of overlap: the more the placenta overlies the os, the more likely it is to persist
- Thickness of placental edge: thick posterior edge → less likely to migrate
- Complete (central) previa — much more likely to persist than marginal/low-lying
- Earlier in pregnancy the diagnosis is made → less likely to persist
Recommended Follow-up Protocol (Creasy & Resnik)
- Follow-up US at 32 weeks — re-evaluate placental position
- If significant change is seen → final US at 36 weeks before deciding delivery route
- If no change (still covering os) → plan cesarean delivery
COMPLICATIONS
Maternal
| Complication | Detail |
|---|---|
| Massive hemorrhage / exsanguination | Risk with complete previa; can be fatal for mother and fetus |
| Preterm delivery | From early bleeding requiring emergent delivery |
| Emergency cesarean | In most previa cases |
| Peripartum hysterectomy | If bleeding from LUS implantation site is uncontrollable |
| Postpartum hemorrhage (PPH) | LUS does not contract as effectively as upper uterus → atony at placental bed |
| Placenta accreta spectrum (PAS) | Major association — especially with prior C/S + anterior previa |
| Air embolism | Rare |
Fetal/Neonatal
| Complication | Detail |
|---|---|
| Preterm birth | From iatrogenic early delivery |
| Fetal growth restriction | Possible placental insufficiency from LUS implantation |
| Fetal anomalies | Reported higher rates (reason unknown) |
| Neurodevelopmental delay | Reported association |
| SIDS (sudden infant death syndrome) | Reported small association |
| Abnormal fetal lie | Transverse, oblique, or breech — placenta blocks cephalic engagement |
| Fetal distress | With significant hemorrhage compromising uteroplacental blood flow |
ASSOCIATED CONDITIONS
Vasa Previa — Critical Emergency
- Fetal blood vessels (unsupported by Wharton's jelly) traverse the fetal membranes and overlie or cross the internal cervical os
- Almost always associated with velamentous cord insertion (cord inserts into membranes rather than placenta) or succenturiate (accessory) lobe
- If undiagnosed and membranes rupture → fetal vessels torn → fetal exsanguination in minutes
- Fetal mortality: 33–100% if undiagnosed before labor; 97% survival with antenatal diagnosis and planned cesarean
- Can mimic placenta previa on presentation (vaginal bleeding)
- Diagnosed by: color Doppler TVS showing vessels overlying os; vessels do not change position with maternal repositioning (unlike umbilical cord loop)
- Management: planned cesarean at ~36 weeks; consider hospitalization from 28–32 weeks
Placenta Accreta Spectrum (PAS)
- PAS is the most feared complication of placenta previa
- With complete previa + prior cesarean: risk of PAS up to 61% with ≥3 prior C/S
- Any woman with previa overlying a cesarean scar must be evaluated for PAS
MANAGEMENT
Guiding Principle
Management is individualized based on:
- Gestational age
- Amount of bleeding
- Maternal hemodynamic stability
- Fetal condition
- Whether the placenta has resolved or persists
Step 1: Immediate Assessment (ALL Patients with Suspected Previa)
- Do NOT perform digital vaginal exam
- Admit to labor and delivery
- Continuous electronic fetal monitoring
- Two large-bore IV lines
- Maternal vital signs — frequent monitoring
- Blood: CBC, type and crossmatch, coagulation panel (PT/PTT, fibrinogen, FDP), hematocrit
- Obstetric Hemorrhage Protocol:
- Type & cross 4 units of PRBCs
- Lab stays 4 units ahead of blood use
- 2 units FFP thawed and available
- 1 ten-pack of platelets available
- Wall clot test: tube of blood should clot within 6 minutes
- Rh immune globulin 300 µg if Rh-negative and not yet given at 28 weeks
- Ultrasound to confirm placenta previa and assess fetal well-being
Step 2: Management Based on Clinical Scenario
Scenario A: Massive/Uncontrolled Hemorrhage — Any Gestation
→ Immediate emergency cesarean delivery
- Under general anesthesia if hemodynamically unstable
- Two large-bore IVs, aggressive fluid resuscitation
- Activate massive transfusion protocol
- Deliver regardless of gestational age
Scenario B: Confirmed Previa, Stable, ≥36 Weeks
→ Elective cesarean delivery
"If the diagnosis is clearly placenta previa and the patient is at or beyond 36 weeks' gestation, delivery is appropriate." — Creasy & Resnik's Maternal-Fetal Medicine
- Amniocentesis for lung maturity confirmation not needed
- Plan delivery at or just after 36 weeks — risk of sudden excessive hemorrhage outweighs any fetal benefit of waiting longer
Scenario C: Confirmed Previa, Stable, 34–36 Weeks
→ Expectant management with close monitoring
- Betamethasone for fetal lung maturity (if <34 weeks or borderline)
- Hospital admission until at least 48 hours bleed-free
- Home management may then be considered if:
- Asymptomatic (no active bleeding, no pain)
- Can maintain limited activity at home
- Adequate support system
- Lives close to hospital (immediate access if bleeding recurs)
- A second significant bleed → readmission until delivery
- Expectant management prolongs pregnancy by average 4 weeks after initial bleed
- Avoid intercourse, pelvic rest, reduce activity
Scenario D: Confirmed Previa, Stable, <34 Weeks
→ Expectant management + corticosteroids + tocolysis
- Betamethasone 12 mg IM × 2 doses (q24h) for fetal lung maturity
- Tocolysis — controversial but both β-mimetics and MgSO₄ have been used with apparent prolongation of pregnancy without adverse effects
- Cervical cerclage — evaluated in small studies; no clear benefit; not recommended
- Bed rest, avoid intercourse
- Close fetal and maternal monitoring
Scenario E: Low-Lying Placenta (Edge 1–20 mm from Os)
→ Trial of labor may be possible
"An asymptomatic woman whose placenta lies more than 2 cm from the cervical os can be allowed to labor safely."
- If placental edge >20 mm from os at 36 weeks → safe for vaginal delivery
- If placental edge ≤20 mm or covering os → cesarean delivery required
- Even low-lying placenta (not covering os) → increased risk of postpartum hemorrhage from LUS atony
Step 3: Cesarean Delivery Technique
"Cesarean delivery for placenta previa should be performed by the most experienced team available because of the substantial risk of intraoperative hemorrhage." — Creasy & Resnik's Maternal-Fetal Medicine
Incision planning:
- In most cases: lower uterine segment transverse incision is appropriate
- If anterior placenta overlies the intended incision:
- Immediately clamp the umbilical cord upon entry to prevent blood loss from placental disruption
- Vertical (classical) incision may be preferable — especially with prematurity or transverse lie
- Avoid cutting through the placenta if possible — go around it
Intraoperative hemorrhage control:
After placenta delivery, the lower uterine segment does not contract as effectively as the upper uterus → placental bed atony is common. Employ:
- Oxytocin (high-dose IV)
- Methyergonovine (Methergine) — if not hypertensive
- Carboprost tromethamine (Hemabate) — 15-methyl PGF₂α
- B-Lynch compression suture (brace suture of uterus)
- Local suturing of the placental bed
- Bakri balloon — intrauterine tamponade balloon for PPH control after C/S
- Hysterectomy — last resort for refractory hemorrhage
Anesthesia
- Spinal or epidural (regional) preferred in stable patients
- General anesthesia required for: hemodynamic instability, active massive hemorrhage, need for emergency delivery
FOLLOW-UP ULTRASOUND SCHEDULE
| Gestational Age | Action |
|---|---|
| 2nd trimester (18–20 weeks anatomy scan) | If low-lying/previa found — schedule follow-up |
| 28–32 weeks | Follow-up US — assess migration |
| 36 weeks | Final US — definitive delivery planning |
| Any time before delivery | TVS for precise os-to-edge measurement |
ABRUPTION vs. PREVIA — Comparison
| Feature | Placenta Previa | Abruption |
|---|---|---|
| Pain | None (painless) | Yes — uterine pain/tenderness |
| Bleeding | Bright red, fresh | Dark, old |
| Bleeding onset | Spontaneous, unprovoked | Often sudden; may follow trauma |
| Uterine tone | Soft, non-tender | Rigid, hypertonic |
| Fetal lie | Often abnormal (transverse/breech) | Usually normal |
| Fetal distress | Uncommon initially | Common |
| Ultrasound diagnosis | Highly sensitive | Low sensitivity |
| Digital exam | Absolutely contraindicated | Allowed (with care) |
| DIC | Rare (unless massive hemorrhage) | Common with severe abruption |
| Recurrence risk | 8× in next pregnancy | Up to 20× in next pregnancy |
| Management | Expectant → planned C/S | Emergency delivery if severe |
HIGH-YIELD CLINICAL PEARLS
- Any painless vaginal bleeding after 20 weeks = placenta previa until proven otherwise by ultrasound
- Never perform digital exam until placenta previa excluded — can cause catastrophic hemorrhage
- TVS is safe and more accurate than TAS — do not avoid it out of fear of provoking bleeding; monitor probe insertion on screen
- Empty the bladder before TVS — full bladder gives false-positive previa
- 90% of previas found in 2nd trimester resolve — do not over-counsel early
- Follow-up US at 32 weeks then 36 weeks before delivery decision
- Deliver at 36 weeks for confirmed previa — risk of sudden hemorrhage outweighs prematurity risk after this gestation
- Complete previa with anterior location + prior cesarean = evaluate aggressively for PAS
- The LUS does not contract well after placental delivery → anticipate PPH; have uterotonic agents ready
- A low-lying placenta (even not covering os) still increases PPH risk from LUS atony
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Rosen's Emergency Medicine: Concepts and Clinical Practice; Morgan & Mikhail's Clinical Anesthesiology, 7th ed.; Textbook of Family Medicine, 9th ed.; Grainger & Allison's Diagnostic Radiology.
Ectopic pregnancy
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, detailed content from all key sources. Here is the full reference:
Source note: Williams Obstetrics is not available in this library. Content is drawn from Creasy & Resnik's Maternal-Fetal Medicine, Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, Roberts & Hedges' Clinical Procedures, and Textbook of Family Medicine 9e — all authoritative peer-level references.
Ectopic Pregnancy — Complete Detailed Reference
DEFINITION
An ectopic pregnancy is one in which the fertilized ovum implants anywhere outside the normal endometrial lining of the uterine cavity.
"Ectopic pregnancy occurs when a conceptus implants outside of the uterine cavity; ruptured ectopic pregnancies are a leading cause of maternal death in the first trimester of pregnancy." — Tintinalli's Emergency Medicine
INCIDENCE AND EPIDEMIOLOGY
| Statistic | Value |
|---|---|
| Overall incidence | 1–2% of all pregnancies |
| Among women presenting to ED with 1st trimester pain or bleeding | ~10–16% |
| Cause of maternal death | 3rd leading cause overall; #1 cause in 1st trimester (4–10% of all maternal deaths) |
| Diagnosis delayed in 50% of cases | In one series of 300 cases, 50% had been evaluated at least twice before correct diagnosis |
| Highest incidence age group | 25–34 years |
| Highest rate | Older women and minority groups |
| Heterotopic pregnancy (simultaneous IUP + ectopic) | Historically 1/30,000; now 1/3,000 general population; up to 1/100 with IVF |
ANATOMIC LOCATIONS
| Site | Frequency | Notes |
|---|---|---|
| Fallopian tube (all sites) | ~95% | Most common overall |
| — Ampulla | ~70% of tubal | Most common tubal site; ampulla is widest, most spacious portion |
| — Isthmus | ~12% of tubal | Narrow lumen → ruptures earlier; more acute presentation |
| — Fimbria | ~11% of tubal | May undergo "tubal abortion" out the fimbrial end |
| — Interstitial (cornual) | ~2–3% of tubal | Within the myometrium of the uterine cornu; highest mortality; rich blood supply → massive hemorrhage; may not rupture until 9–16 weeks |
| Abdominal | ~1% | Most from early tubal rupture/abortion with reimplantation in peritoneum; very rarely primary |
| Ovarian | ~0.5% | |
| Cervical | ~0.03% | Predisposing factor: prior D&C, Asherman syndrome; risk of uncontrollable hemorrhage |
| Cesarean scar | Rare but increasing | Implantation at prior uterine scar; can cause massive maternal hemorrhage; diagnosis: empty uterine sac and canal, gestational sac at uterine isthmus on US |
| Heterotopic | Rare | Concurrent IUP + ectopic; markedly increased with ART |
"The vast majority of ectopic pregnancies implant in the ampullary portion of the fallopian tube. The underlying cause is most often damage to the tubal mucosa from previous infection, preventing transport of the ovum to the uterus." — Tintinalli's Emergency Medicine
PATHOPHYSIOLOGY
Normal Fertilization and Implantation
- Fertilization occurs in the ampullary segment of the fallopian tube, approximately 8–9 days after ovulation
- The zygote normally travels along the tube and implants in the endometrium
- Normal peristalsis + ciliary action transport the embryo toward the uterus in 3–4 days
What Goes Wrong in Ectopic Pregnancy
1. Impaired tubal transport (most common mechanism)
- Tubal scarring from prior infection (PID) → damaged mucosal cilia, impaired peristalsis, tubal stricture
- Fertilized ovum stalls in the tube → implants in tubal wall
- Tubal surgery → disrupts normal tubal architecture
2. Embryo-related factors
- Defects in the ovum → premature implantation before it reaches the uterus
- Elevated estradiol or progesterone → inhibits tubal migration
3. Abnormal endometrium (host factors)
- Inhospitable endometrium → embryo more likely to implant ectopically
What Happens After Tubal Implantation
Once the embryo implants in the tube:
- Trophoblasts penetrate the muscular tubal wall — blood seeps into tubal tissue
- Intermittent distention of the tube with blood → intermittent pain
- Blood leaks from fimbriated end into peritoneal cavity (→ hemoperitoneum) or through the tubal wall
- The aborting ectopic may:
- Tubal abortion: expelled out the fimbrial end into the peritoneal cavity (usually ~6 weeks)
- Tubal rupture: tube tears, causing sudden massive hemorrhage (usually 6–10 weeks for ampullary; earlier for isthmic; later for interstitial)
- Death from maternal exsanguination after rupture — can occur within minutes
RISK FACTORS
| Risk Factor | Detail |
|---|---|
| Prior ectopic pregnancy | Subsequent ectopic risk up to 22% depending on treatment |
| Prior PID / salpingitis | Accounts for 50% of ectopic cases; risk 3× after one episode; 6–10× higher than women without PID history |
| Tubal surgery (sterilization, prior ectopic surgery) | Especially laparoscopic partial salpingectomy or electrodestruction; risk highest 5–15 years after procedure especially if done at age <28 |
| IUD (intrauterine device) | IUD prevents most pregnancies but if pregnancy occurs while IUD in situ → high risk of ectopic; PID risk with IUD also contributes |
| Assisted reproduction (ART) | ~4% of IVF pregnancies are ectopic; heterotopic risk up to 1% |
| Cigarette smoking | Alters embryo tubal transport |
| Advanced maternal age (35–44) | Age-related changes in tubal function |
| Prior spontaneous or induced abortion | Scarring, adhesions |
| History of infertility | Often related to tubal pathology |
| Multiple sexual partners | Increases PID risk |
| Prior gonorrhea/Chlamydia | Tubal scarring |
Important: Risk factors absent in almost half of patients — ectopic pregnancy must be considered in any woman of reproductive age with pain and/or vaginal bleeding regardless of risk factor profile.
"Pregnancy in a patient with prior tubal surgery for sterilization is assumed to be an ectopic pregnancy until proven otherwise." — Tintinalli's Emergency Medicine
CLINICAL FEATURES
Classic Triad
- Amenorrhea (delayed menses)
- Abdominal/pelvic pain
- Vaginal bleeding (usually light)
Warning: This classic triad is present in only a minority of cases. The presentation is highly variable.
Symptoms
| Symptom | Frequency / Detail |
|---|---|
| Abdominal pain | 90% of ectopic pregnancies; most common symptom; due to tubal distention or rupture |
| — Unruptured | Dull, crampy, intermittent, lateral; may be mild or moderate |
| — Ruptured | Sudden, sharp, severe, lateralized → peritoneal irritation |
| Amenorrhea | 70% have missed a period; 15–20% have NOT missed a period |
| Vaginal bleeding | Usually scant to mild; heavy bleeding suggests miscarriage but does not exclude ectopic |
| Shoulder pain | Diaphragmatic irritation from blood tracking to upper abdomen; pathognomonic of hemoperitoneum |
| Syncope / dizziness | Significant hemoperitoneum or hemodynamic compromise |
| Rectal pressure | Blood pooling in cul-de-sac irritates rectum |
| Nausea, breast tenderness | Normal pregnancy symptoms may be present |
Physical Examination
| Finding | Detail |
|---|---|
| Adnexal tenderness | Most common pelvic finding |
| Cervical motion tenderness (CMT) | Present in some; not specific (also seen in PID) |
| Adnexal mass | Palpated in only 10–20% of patients |
| Uterine size | Usually normal for gestational age |
| Cervix | May have bluish discoloration (as in normal pregnancy) |
| Tachycardia | Not always present even with significant hemoperitoneum |
| Hypotension | Present in severe cases; may be absent due to compensatory mechanisms |
| Bradycardia | Can occur from vagal stimulation with hemoperitoneum — do not be falsely reassured |
| Peritoneal signs | Rebound tenderness, rigidity — suggests rupture with hemoperitoneum |
| Fever | Rare (distinguishes from PID) |
"Blood in the peritoneal cavity does not consistently correlate with peritoneal irritation, blood pressure, or pulse rate. Bradycardia in the presence of significant intraperitoneal bleeding from a ruptured ectopic pregnancy is not unusual." — Roberts & Hedges' Clinical Procedures
"Vital signs may be normal despite significant hemoperitoneum." — Tintinalli's Emergency Medicine
DIAGNOSTIC APPROACH
The Core Principle
"Because the history and physical examination are insensitive and nonspecific, pelvic ultrasonography and serum hCG are essential to locate the pregnancy in any patient who has abdominal pain or vaginal bleeding and a positive pregnancy test." — Rosen's Emergency Medicine
Step 1: Urine or Serum Pregnancy Test
- First step in any woman of reproductive age with pain or bleeding
- Qualitative urine hCG: highly sensitive; if positive → pursue ultrasound and quantitative hCG
- A single hCG level cannot exclude ectopic pregnancy — even very low levels (<500 mIU/mL) have been associated with ruptured ectopics requiring surgery
Step 2: Transvaginal Ultrasound (TVS) — Primary Diagnostic Tool
Normal hCG Levels at Gestation (for reference):
| Post-Conception Week | β-hCG (mIU/mL) |
|---|---|
| <1 week | 5–50 |
| 1–2 weeks | 50–500 |
| 2–3 weeks | 100–5,000 |
| 3–4 weeks | 500–10,000 |
| 4–5 weeks | 1,000–50,000 |
| 5–6 weeks | 10,000–100,000 |
| 6–8 weeks | 15,000–200,000 |
Discriminatory Zone:
- TVS: IUP should be visible at hCG ≥1,500–2,000 mIU/mL (institution-dependent)
- TAS: IUP should be visible at hCG ≥6,000 mIU/mL
- If hCG above discriminatory zone and no IUP seen on TVS → ectopic pregnancy must be strongly suspected
- However: ectopic pregnancy can occur and rupture at any level of hCG, including <500 mIU/mL
TVS — What to Look For:
| Sonographic Finding | Significance |
|---|---|
| Double decidual sac sign, yolk sac in uterus, fetal pole in uterus | Diagnostic of IUP — ectopic excluded (unless heterotopic) |
| Intrauterine fetal cardiac activity | Diagnostic of viable IUP |
| Cardiac activity in tube / adnexa | Diagnostic of ectopic |
| Ectopic fetal pole (without cardiac activity) | Diagnostic of ectopic |
| Adnexal mass without IUP | Highly suggestive of ectopic |
| Moderate or large cul-de-sac fluid without IUP | Suggestive of ectopic (hemoperitoneum) |
| Free fluid in Morrison's pouch (hepatorenal space) | Significant hemoperitoneum → predicts need for operative intervention |
| Empty uterus | Indeterminate — could be very early IUP, failed IUP, or ectopic |
| Pseudogestational sac (decidual reaction) | May mimic IUP; is actually fluid in uterine cavity from ectopic |
Timing of TVS Findings in Normal Pregnancy:
- Gestational sac: ~4.5 weeks by TVS
- Yolk sac: ~5.5 weeks by TVS
- Fetal pole: ~6.0 weeks by TVS (TAS: ~1 week later than TVS)
Indeterminate US (~20% of ED cases): neither IUP nor definite ectopic seen
- Among patients with indeterminate US: 53% → embryonic demise; 15% → ectopic; only 29% → normal IUP
Critical Point: An IUP on ultrasound does not rule out ectopic in ART patients — heterotopic pregnancy must be considered. For spontaneous conceptions, demonstrating an IUP provides high confidence against ectopic.
Step 3: Serial Quantitative β-hCG Levels
Normal IUP pattern: hCG doubles every 1.8–3 days in first 6–7 weeks
| hCG Pattern | Interpretation |
|---|---|
| Rise ≥66% in 48 hours | Favors viable IUP (~85% of normal IUPs) |
| Rise <66% in 48 hours or plateau | Abnormal pregnancy — ectopic or failing IUP |
| Rapid decline | Favors spontaneous miscarriage |
| Slow decline | Can indicate ectopic pregnancy |
| Any single level (however low) | Cannot exclude ectopic |
"~15% of normal IUPs have a minimal rise in hCG, requiring a third serial test."
"Ruptured ectopic pregnancies requiring surgery have been reported with very low or absent levels of hCG."
Step 4: Serum Progesterone
| Level | Interpretation |
|---|---|
| >25 ng/mL | Likely normal IUP (<2% are ectopic) |
| <15 ng/mL | 81% of ectopics; 93% of abnormal IUPs; only 11% of normal IUPs |
| <5 ng/mL | Effectively excludes viable IUP; failing IUP or ectopic |
- Not a standard ED tool but useful adjunct in stable patients with indeterminate US + low hCG
- A value <5 ng/mL → can proceed to D&C to look for chorionic villi
Step 5: Other Diagnostic Modalities
D&C (Dilation and Curettage):
- Identifies chorionic villi in endometrial samples → confirms failing IUP and excludes ectopic (in ~70% of cases even with empty uterus on US)
- Can identify villi in 50% of women with empty uterus on US
- Used when: non-rising hCG, indeterminate US, stable patient
- If no villi found → strong suspicion for ectopic → proceed to medical or surgical management
Culdocentesis (largely obsolete):
- Aspiration of cul-de-sac through posterior vaginal fornix
- Non-clotting blood = hemoperitoneum = strongly suggestive of ectopic
- Replaced by TVS; poor sensitivity; false positives from vascular structures; rarely used now
Laparoscopy:
- Gold standard for diagnosis — most accurate
- Appropriate for: unstable patients, peritoneal signs, nondiagnostic US, need for simultaneous treatment
- Can be both diagnostic and therapeutic in the same setting
MRI:
- High sensitivity and specificity
- Theoretical interest only in acute setting — too slow, costly, limited availability
CLASSIFICATION BY HEMODYNAMIC STATUS
Unstable (~20% of cases)
- Hypovolemia, shock, significant hemoperitoneum (free fluid in Morrison's pouch), open cervical os, peritoneal signs
- → Emergency surgery immediately — no time for further diagnostic workup
Stable (~80% of cases)
- Goal: locate the pregnancy and determine viability before deciding management
- Management based on US + hCG pattern + clinical context
MANAGEMENT
A. Unstable Patient — Surgical Emergency
- Two large-bore IV lines → aggressive crystalloid + blood product resuscitation
- Type and crossmatch, CBC, coagulation studies
- Emergency laparoscopy (preferred) or laparotomy if hemodynamically crashing
- Salpingectomy (removal of tube containing ectopic) in most rupture cases
- Salpingostomy (linear incision, ectopic removed, tube preserved) if tube-sparing desired — but higher risk of persistent ectopic (~5–20%); requires serial hCG follow-up
- Rh immune globulin 50–300 µg IM if Rh-negative (within 72 hours)
B. Stable Patient — Medical Management with Methotrexate (MTX)
Methotrexate is a folic acid antagonist — inhibits dihydrofolate reductase → depletes cofactors for DNA/RNA synthesis → destroys rapidly dividing trophoblastic cells → involution of pregnancy
Criteria for MTX Eligibility (all must be met):
- Hemodynamically stable
- Unruptured ectopic (confirmed on US)
- Able to comply with follow-up (serial hCG monitoring weekly)
- No contraindications
Absolute Contraindications to MTX:
| Absolute | Relative |
|---|---|
| Intrauterine pregnancy | Cardiac activity on TVS |
| Immunodeficiency | hCG >5,000 mIU/mL |
| Moderate-severe anemia/leukopenia/thrombocytopenia | Ectopic mass >4 cm on US |
| MTX hypersensitivity | Refusal of blood transfusion |
| Active pulmonary disease | Inability to return for follow-up |
| Active peptic ulcer disease | |
| Significant hepatic or renal dysfunction | |
| Breastfeeding | |
| Hemodynamic instability |
MTX Regimens:
Single-dose (most common):
- 50 mg/m² IM
- Check hCG on day 4 and day 7 post-injection
- Expected: hCG should decrease ≥15% between days 4 and 7
- If <15% decline → repeat dose or proceed to surgery
- Success rate: 88.1% overall; drops to 86% if hCG >5,000 mIU/mL
- Failure rate ~14.3% when hCG >5,000 mIU/mL vs. only 3.7% when <5,000 mIU/mL
Multiple-dose (for higher hCG levels):
- MTX + leucovorin (folinic acid) on alternating days
- Success rate 92.7% — higher than single dose
Common Side Effects of MTX:
- Abdominal pain in up to 75% (3–7 days after treatment) — "separation pain" from tubal abortion / hematoma; usually self-limited; treat with NSAIDs
- Flatulence
- Stomatitis (mouth sores)
- Nausea, vomiting
- Bone marrow suppression (rare at single-dose regimen)
- Photosensitivity — avoid sun exposure during treatment
Distinguishing "Separation Pain" vs. Rupture:
- Both occur 3–7 days after MTX
- Separation pain: mild-moderate, self-limited
- Rupture: severe, with hemodynamic instability, free fluid on US, falling hematocrit
- Evaluation: CBC + abdominal US to rule out hemoperitoneum
- If moderate/severe pain + free fluid + rebound → proceed to surgery
Patient Instructions After MTX Discharge:
- Return immediately for: vaginal bleeding, worsening pain, dizziness, syncope
- No sexual intercourse for 14–21 days (until hCG undetectable) — intercourse can trigger rupture
- Avoid NSAIDs (interfere with MTX clearance — use acetaminophen instead) in some protocols; check institutional guidelines
- Avoid folic acid supplements (antagonizes MTX)
- Serial hCG monitoring until undetectable
- No pregnancy for 3 months after MTX (teratogenic effect)
C. Surgical Management — Laparoscopic Options
| Procedure | Indication | Advantages | Disadvantages |
|---|---|---|---|
| Salpingostomy | Unruptured; desire to preserve tube | Preserves tube; possible future fertility | Persistent ectopic in 5–20%; requires hCG monitoring |
| Salpingectomy | Ruptured; damaged tube; no fertility desire; persistent ectopic | Definitive; no persistent ectopic risk | Removes tube |
| Laparotomy | Hemodynamically unstable; laparoscopy not feasible | Access in emergency | More morbid than laparoscopy |
"Salpingostomy is preferred to salpingectomy if the patient is stable and the procedure is technically feasible." — Rosen's Emergency Medicine
"An increasing number of surgeries are being performed through the laparoscope. The advent of transvaginal ultrasonography has resulted in earlier diagnosis and a trend toward nonoperative management."
SPECIAL TYPES OF ECTOPIC PREGNANCY
Interstitial (Cornual) Ectopic
- Implants within the intramural portion of the tube as it traverses the uterine myometrium
- Rich blood supply → can grow larger before rupturing (may not rupture until 9–16 weeks)
- Higher mortality than standard tubal ectopic — rupture causes massive hemorrhage
- Diagnosis: TVS shows empty uterine cavity + gestational sac lateral to uterine cavity with thin (<5 mm) myometrial mantle surrounding it
- Treatment: MTX (if unruptured, early) or cornual resection/hysterectomy
Cervical Ectopic
- <1% of ectopics; predisposing factors: prior D&C, Asherman syndrome, prior cervical surgery
- Presents with painless heavy vaginal bleeding (mimics placenta previa)
- Diagnosis: gestational sac within the cervical canal on TVS
- Treatment: MTX (preferred if viable); if uncontrolled bleeding → cervical sutures, Foley balloon tamponade, UAE, hysterectomy as last resort
Ovarian Ectopic
- 0.5% of ectopics; difficult to distinguish from corpus luteum cyst clinically
- Criteria (Spiegelberg): tube intact on same side, sac in position of ovary, connected to uterus by ovarian ligament, ovarian tissue in sac wall
Abdominal Ectopic
- ~1%; usually from early tubal rupture/abortion with reimplantation on peritoneum, bowel, omentum, or mesentry
- Can occasionally reach viability (advanced abdominal pregnancy)
- High maternal (and fetal) morbidity; requires surgical management
Cesarean Scar Ectopic
- Implantation at prior uterine incision scar
- Increasingly common with rising cesarean rates
- Risk of massive hemorrhage and uterine rupture
- Diagnosis: empty uterine cavity, empty cervical canal, gestational sac at anterior uterine isthmus within the scar
- Treatment: MTX, UAE, surgical resection, or hysterectomy depending on clinical status
Heterotopic Pregnancy
- Simultaneous IUP + ectopic in the same patient
- Spontaneous rate: ~1/3,000; with IVF: up to 1%
- Risk factors: ART, multiple embryo transfer, PID history, tubal surgery
- Presentation: pain + bleeding with known IUP → do not be falsely reassured by the IUP
- Diagnosed in first 5–8 weeks; only 26% diagnosable by TVS (rest require laparoscopy)
- Treatment: surgical or US-guided injection of KCl into the ectopic pregnancy (to preserve the IUP); overall delivery rate for the IUP after treatment ~70%
- MTX is contraindicated (would harm the IUP)
DIFFERENTIAL DIAGNOSIS
| Condition | Key Distinguishing Features |
|---|---|
| Threatened miscarriage | Viable IUP confirmed on US; cramping + light bleeding |
| Inevitable/incomplete miscarriage | Dilated cervix; heavy bleeding; IUP failing on US |
| Corpus luteum cyst rupture | Positive pregnancy test helps; IUP seen on US; thin-walled cystic mass |
| Appendicitis | Right-sided pain; fever; negative pregnancy test (usually) |
| PID / tubo-ovarian abscess | Fever; cervicitis; bilateral adnexal tenderness; negative hCG (if not pregnant) |
| Ovarian torsion | Sudden severe unilateral pain; adnexal mass; Doppler shows reduced flow |
| Urinary tract pathology | Dysuria, hematuria; normal pelvic US |
| Degenerating fibroid | Uterine tenderness; fibroid on US; negative hCG |
FOLLOW-UP AFTER TREATMENT
After MTX:
- Weekly hCG until undetectable
- No pregnancy for 3 months (MTX teratogenic)
- Monitor for signs of treatment failure (pain, instability) — can rupture even during MTX therapy
- Persistent ectopic (hCG not falling adequately): repeat MTX dose or surgery
After Surgical Treatment:
- hCG to zero post-salpingostomy (to exclude persistent ectopic)
- Not needed after salpingectomy (unless concern for residual tissue)
- Discuss future fertility counseling
- Risk of recurrent ectopic in future pregnancies: up to 22%
RECURRENCE AND FUTURE FERTILITY
| Factor | Risk |
|---|---|
| Subsequent ectopic after one ectopic | Up to 22% |
| Spontaneous IUP after one ectopic | ~60–65% |
| After salpingostomy (tube preserved) | Slightly better fertility outcomes vs. salpingectomy |
| After salpingectomy | May need IVF if contralateral tube also damaged |
KEY CLINICAL PEARLS
- Any woman of reproductive age + pain or bleeding = pregnancy test first, always
- The classic triad is present in a minority — do not wait for it
- Risk factors absent in ~50% of patients — do not use their absence to downgrade concern
- A single hCG level cannot exclude ectopic — even <500 mIU/mL ectopics have ruptured
- Vital signs can be normal despite significant hemoperitoneum — bradycardia can occur paradoxically
- An IUP on US does not exclude ectopic in IVF patients — heterotopic always possible
- Indeterminate US + hCG > discriminatory zone → high suspicion; manage as ectopic until proven otherwise
- MTX: use when stable, unruptured, <4 cm, no cardiac activity, hCG <5,000 ideally
- "Separation pain" 3–7 days after MTX is expected — distinguish from rupture by US + vitals
- After treatment: no pregnancy for 3 months (MTX); watch for recurrence
Sources: Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Tintinalli's Emergency Medicine: A Comprehensive Study Guide; Rosen's Emergency Medicine: Concepts and Clinical Practice; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Textbook of Family Medicine, 9th ed.; Berek & Novak's Gynecology.
Molar pregnancy
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have very comprehensive content. Here is the complete, detailed reference:
Source note: Williams Obstetrics is not in this library. Content is from Berek & Novak's Gynecology (primary — the most comprehensive GTD reference available), Creasy & Resnik's Maternal-Fetal Medicine, Rosen's Emergency Medicine, Robbins & Cotran Pathologic Basis of Disease, and Textbook of Family Medicine 9e.
Molar Pregnancy (Gestational Trophoblastic Disease) — Complete Detailed Reference
OVERVIEW — The GTD Spectrum
Gestational Trophoblastic Disease (GTD) is an umbrella term for a heterogeneous group of interrelated lesions characterized by abnormal proliferation of placental trophoblasts. It ranges from benign (hydatidiform moles) to malignant (gestational trophoblastic neoplasia — GTN).
"GTD is the most successfully treated gynecologic cancer and one of the most curable solid tumors in women." — Creasy & Resnik's Maternal-Fetal Medicine
Full GTD Classification
| Category | Lesion | Behavior |
|---|---|---|
| Benign / Pre-malignant | Complete hydatidiform mole | Benign but malignant potential |
| Partial (incomplete) hydatidiform mole | Benign, low malignant potential | |
| GTN — Malignant | Invasive mole | Locally invasive; rarely metastasizes |
| Choriocarcinoma | Highly malignant; early metastasis | |
| Placental site trophoblastic tumor (PSTT) | Rare; intermediate trophoblasts; chemo-resistant | |
| Epithelioid trophoblastic tumor (ETT) | Rare; similar to PSTT |
"GTNs are among the rare human tumors that can be cured even in the presence of widespread dissemination." — Berek & Novak's Gynecology
INCIDENCE AND EPIDEMIOLOGY
| Region | Incidence |
|---|---|
| United States | 1 in 1,000–2,000 pregnancies |
| Japan | 2 in 1,000 pregnancies (3× higher than US) |
| Taiwan | 1 in 125 pregnancies |
| Southeast Asia | Twice as common as US |
| Complete mole (Ireland study) | 1 in 1,945 pregnancies |
| Partial mole (Ireland study) | 1 in 695 pregnancies |
Why does incidence vary?
- Socioeconomic and nutritional factors — decreasing dietary carotene (Vitamin A precursor) and animal fat associated with increased complete mole rate
- South Korea's declining incidence attributed to Westernized diet and improved living standards
TYPE 1: COMPLETE HYDATIDIFORM MOLE
Pathogenesis / Cytogenetics
| Feature | Detail |
|---|---|
| Karyotype | 46,XX (90%); 46,XY (10%) |
| All chromosomes | Entirely of paternal origin (androgenesis) |
| Mechanism (monospermic — 90%) | Empty ovum (nucleus absent/inactivated) fertilized by one haploid sperm → sperm duplicates its own chromosomes |
| Mechanism (dispermic — 10%) | "Empty" ovum fertilized by two sperm → 46,XX or 46,XY |
| Fetal/embryonic tissue | Absent |
| Mitochondrial DNA | Maternal origin (mitochondria from ovum) |
"Complete moles arise from an ovum fertilized by a haploid sperm, which duplicates its own chromosomes. The ovum nucleus may be absent or inactivated." — Berek & Novak's Gynecology
Gross and Microscopic Pathology
- Gross: delicate, friable mass of thin-walled, translucent, cystic, grape-like vesicles — swollen edematous (hydropic) villi
- Microscopic:
- All villi are enlarged, smooth, oval with central cavitation (cisterns)
- Diffuse trophoblastic hyperplasia (both cyto- and syncytiotrophoblast)
- No scalloping of villi
- No trophoblastic stromal inclusions
- No fetal tissue

Risk Factors Specific to Complete Mole
- Age >40 years: 2–10 fold increased risk
- Age >50 years: 1 in 3 pregnancies is molar
- Adolescents: 7-fold increased risk
- Prior molar pregnancy: significantly increased recurrence
- Prior miscarriage
- Low dietary carotene / animal fat intake
- Extremes of reproductive age (both ends of the spectrum)
TYPE 2: PARTIAL (INCOMPLETE) HYDATIDIFORM MOLE
Pathogenesis / Cytogenetics
| Feature | Detail |
|---|---|
| Karyotype | Triploid (69,XXX or 69,XXY) or occasionally tetraploid (92,XXXY) |
| Mechanism | Normal ovum fertilized by two sperm simultaneously (dispermy) |
| Fetal/embryonic tissue | Present (but growth restricted and often with lethal anomalies) |
| Fetal anomalies | CNS anomalies, syndactyly, skeletal abnormalities |
Microscopic Pathology
- Focal (not diffuse) hydropic villi
- Focal trophoblastic hyperplasia
- Scalloping of chorionic villi present (characteristic)
- Trophoblastic stromal inclusions present
- Fetal/embryonic tissue present (often with anomalies)
COMPLETE vs. PARTIAL MOLE — Comparison Table
| Feature | Complete Mole | Partial (Incomplete) Mole |
|---|---|---|
| Fetal/embryonic tissue | Absent | Present (abnormal) |
| Karyotype | 46,XX (90%); 46,XY | Triploid (69,XXX, 69,XXY) |
| Chromosomal origin | All paternal | 2 paternal + 1 maternal sets |
| Villi swelling | Diffuse | Focal |
| Trophoblastic hyperplasia | Diffuse | Focal |
| Scalloping of villi | Absent | Present |
| Stromal inclusions | Absent | Present |
| Uterine size | Large for dates (>dates in 28%) | Small or equal to dates |
| hCG level | Markedly elevated (>100,000 in many) | Usually lower |
| Theca lutein cysts | ~50% of patients | Rare / absent |
| Preeclampsia | Up to 27% | ~2.5% |
| Hyperemesis | ~8–25% | Rare |
| Hyperthyroidism | ~7% | Rare |
| GTD risk after evacuation | 15–20% (local invasion 15%, metastasis 4%) | 1–5% |
| Choriocarcinoma risk | ~2.5% | Very rare |
| Diagnosis timing | Usually 1st trimester | Usually 2nd trimester (or found on histology) |
| Clinical diagnosis | Usually apparent (classic features) | Often misdiagnosed as incomplete/missed abortion (91.3% in one series) |
CLINICAL FEATURES
Complete Mole — Classic Presentation (Historic vs. Current)
Note: With widespread early TVS use, many complete moles are now diagnosed at 9–10 weeks with fewer classic features.
| Feature | Historic Frequency | Current (Early Diagnosis Era) |
|---|---|---|
| Vaginal bleeding | 97% | 46% (most common presenting symptom) |
| Excessive uterine size (>dates) | ~50% | 28% |
| Hyperemesis | ~25% | ~8% |
| Theca lutein cysts (≥6 cm) | ~50% | Present in ~50% |
| Preeclampsia before 24 weeks | 27% | ~1–2% (but pathognomonic when present) |
| Hyperthyroidism | 7% | Rare |
| Anemia (Hb <10 g/dL) | ~50% | ~5% |
| Respiratory distress | Occurs peri-evacuation | Occurs peri-evacuation |
Vaginal Bleeding
- Most common presenting symptom
- Molar tissues separate from decidua → disrupting maternal vessels
- Large volumes of retained blood may distend endometrial cavity
- May be considerable and prolonged
Excessive Uterine Size
- Present in ~28% currently
- Due to: chorionic tissue bulk + retained blood + trophoblastic overgrowth
- Associated with markedly elevated hCG
Theca Lutein Ovarian Cysts
- Present in ~50% of complete moles
- Result from ovarian hyperstimulation by very high hCG levels
- Can be large (up to 30 cm); may not be palpable (uterus enlarged) — US documents them
- Spontaneously regress within 2–4 months after evacuation
- Complications: torsion, rupture → acute pelvic pain → laparoscopy
- Do NOT need to be removed (they regress)
Preeclampsia Before 24 Weeks — Pathognomonic
Preeclampsia developing before 24 weeks should always prompt consideration of molar pregnancy
- Hypertension, proteinuria, hyperreflexia — classic preeclampsia features
- Eclamptic convulsions rare
- Occurs almost exclusively when uterine size is excessive and hCG markedly elevated
Hyperemesis Gravidarum
- From extremely high hCG levels (hCG has TSH-like and FSH-like activity)
- May cause severe electrolyte disturbances requiring IV fluid replacement
- Severe nausea/vomiting disproportionate to gestational age
Hyperthyroidism
- Historically 7%; rare now with early diagnosis
- hCG has TSH-like activity → stimulates thyroid → elevated free T3 and T4
- Symptoms: tachycardia, warm skin, tremor
- CRITICAL: Anesthesia or surgery can precipitate thyroid storm in untreated hyperthyroid patients
- Before molar evacuation: if hyperthyroid → administer β-blockers first; have treatment for thyroid storm ready
- Thyroid storm: hyperthermia, delirium, convulsions, tachycardia, high-output heart failure, cardiovascular collapse
Respiratory Distress (Trophoblastic Pulmonary Embolism)
- Occurs during or after molar evacuation
- Chest pain, dyspnea, tachypnea, tachycardia, bilateral pulmonary infiltrates on CXR
- From: trophoblastic cell embolization, cardiopulmonary effects of thyroid storm, preeclampsia, massive fluid replacement
- Usually resolves within 72 hours with cardiopulmonary support
- May require mechanical ventilation
Partial Mole — Clinical Presentation
- Usually no dramatic features of complete mole
- Presents like incomplete or missed abortion — diagnosed on histology of curettage specimen
- Main symptom: vaginal bleeding (73%)
- Excessive uterine size: ~4%
- Preeclampsia: ~2.5%
- No theca lutein cysts, no hyperemesis, no hyperthyroidism typically
- Pre-evacuation hCG >100,000 mIU/mL in only 7% of partial moles (vs. common in complete)
- 91% initially diagnosed as incomplete/missed abortion — only confirmed as partial mole on pathologic review
DIAGNOSIS
Ultrasound — Classic Features
Complete mole: "Snowstorm appearance" — echogenic mass filling the uterus with multiple small anechoic (cystic) spaces ("Swiss cheese" or vesicular pattern), no embryo or fetal parts
Partial mole: enlarged placenta with focal cystic lesions; embryo/fetal structures may be visible (but abnormal); Swiss cheese changes less prominent
Note: With early diagnosis (9 weeks), the snowstorm pattern may not yet be fully developed. Many early complete moles appear as a heterogeneous echogenic mass without discrete cysts.
| US Feature | Complete Mole | Partial Mole |
|---|---|---|
| Fetal parts | Absent | Present (abnormal) |
| Placenta | Replaced by vesicular tissue | Enlarged with cystic areas |
| Classic pattern | "Snowstorm" | Focal Swiss cheese changes |
| Theca lutein cysts | Often present bilaterally | Absent |
Quantitative β-hCG
- Markedly elevated — often >100,000 mIU/mL in complete mole
- In partial mole: usually lower; >100,000 mIU/mL in only ~7%
- hCG is the essential tumor marker for diagnosis, treatment monitoring, and surveillance
Histopathology — Definitive Diagnosis
- All products of conception from D&C should be sent for pathologic examination
- Confirms mole type and rules out choriocarcinoma
- Partial moles are frequently only diagnosed on histology (not clinically suspected)
"Phantom hCG" / False-Positive hCG
- Heterophilic antibodies in serum can create false-positive serum hCG results
- Leads to inappropriate treatment for GTN
- Exclusion: run simultaneous urine hCG — serum heterophilic antibodies NOT excreted in urine → urine hCG will be negative in phantom hCG
- Alternative: serial dilution of serum (true hCG shows linear decrease); or use alternative hCG assay platform
MANAGEMENT
Step 1: Pre-Evacuation Workup
- Baseline quantitative serum hCG
- CBC, blood type and screen, coagulation studies
- Thyroid function tests (T3, T4, TSH) — check for hyperthyroidism
- Chest X-ray (rule out pulmonary metastases)
- Renal and liver function tests
- Pelvic ultrasound (document mole + theca lutein cysts)
- Two large-bore IV lines
- If hyperthyroid → consult endocrinology + anesthesia; administer β-blockers before proceeding
Step 2: Uterine Evacuation
Preferred Method: Suction Curettage (regardless of uterine size)
Procedure steps:
- Oxytocin infusion started before anesthesia induction (reduces bleeding risk)
- Cervical dilation — bleeding often increases at this stage (expected); retained blood expelled
- Suction curettage — use 12-mm cannula; uterine size decreases dramatically within minutes; bleeding controlled
- If uterus >14 weeks: place one hand on fundus, massage uterus during evacuation (prevents perforation)
- Sharp curettage — gentle, after suction complete, to remove residual molar tissue
- Oxytocin continued after evacuation to maintain uterine tone
- Rh immune globulin — trophoblast cells express RhD antigen → administer if Rh-negative
- Ultrasound guidance preferred during evacuation
Why NOT medical evacuation (misoprostol alone)?
- Risk of incomplete evacuation (up to 25%)
- Hemorrhage
- Infection
- Trophoblastic embolization → respiratory failure, death
- Higher risk of needing subsequent chemotherapy
Hysterectomy — alternative if:
- Patient desires sterilization
- Ovaries preserved even with theca lutein cysts present (cysts will regress)
- Does NOT prevent metastasis — hCG monitoring still required post-hysterectomy
Step 3: Prophylactic Chemotherapy (Controversial)
| Indication | Recommendation |
|---|---|
| Low-risk complete mole | Generally NOT recommended (only 20% will develop GTN; exposes 80% unnecessarily) |
| High-risk complete mole (hCG >100,000, large uterus, theca lutein cysts >6 cm) | Consider single course actinomycin D — reduces persistent tumor (from 47% to 14% in high-risk) |
| When reliable hCG follow-up is unavailable | Prophylactic chemotherapy recommended |
A single course of actinomycin D at evacuation: local invasion decreased from 47% to 4%; no metastases developed.
POST-EVACUATION SURVEILLANCE — hCG Monitoring
Complete Mole Protocol
| Phase | Frequency | Duration |
|---|---|---|
| Phase 1 | Weekly hCG | Until normal for 3 consecutive weeks |
| Phase 2 | Monthly hCG | Until normal for 6 consecutive months |
| Average time to first normal hCG | ~9 weeks | |
| Risk of GTN once hCG undetectable | Approaches zero |
Partial Mole Protocol
- Weekly hCG until undetectable → then 3 months monitoring (shorter than complete mole)
- Risk of GTN after partial mole is very low (1–5%)
- Surveillance may be safely abbreviated once hCG is undetectable
Diagnosis of Post-Molar GTN (Referral Criteria)
Refer to gynecologic oncologist if:
- hCG plateaus (no change) over 3 weekly measurements
- hCG rises on 2 consecutive weekly measurements
- hCG persists for more than 6 months without becoming undetectable
Contraception During Surveillance
- Highly recommended during entire hCG surveillance period — pregnancy would interfere with hCG monitoring
- Oral contraceptives: safe to use after molar evacuation (prospective trials confirm no increased GTN risk)
- IUD: avoid until hCG is normal (risk of uterine perforation, bleeding, infection with elevated hCG)
- Barrier methods: acceptable
When Can Patient Try to Conceive?
- After complete mole: avoid pregnancy for 12 months (1 year) from hCG remission
- After partial mole: avoid pregnancy for at least 6 months after hCG remission
- After GTN/chemotherapy: wait until 12 months after completion of chemotherapy — subsequent pregnancies have normal outcomes with no increased congenital abnormality risk
HIGH-RISK MARKERS — Who is at Risk for Developing GTN?
At the New England Trophoblastic Disease Center (NETDC), reviewing 858 complete mole patients — two-fifths had at least one of these high-risk signs:
| High-Risk Sign | Criteria |
|---|---|
| Markedly elevated hCG | >100,000 mIU/mL |
| Excessive uterine size | Greater than dates |
| Theca lutein cysts | ≥6 cm diameter |
Outcomes by Risk Group:
| Group | Local Invasion | Metastasis |
|---|---|---|
| High-risk (any one sign) | 31% | 8.8% |
| Low-risk (no high-risk signs) | 3.4% | 0.6% |
GESTATIONAL TROPHOBLASTIC NEOPLASIA (GTN)
When molar tissue persists, invades, or metastasizes after evacuation:
Nonmetastatic (Invasive Mole) — 15% after complete mole evacuation
Symptoms:
- Irregular vaginal bleeding
- Persistent/rising hCG
- Uterine subinvolution or asymmetric enlargement
- Theca lutein cysts persist
- Tumor may perforate myometrium → hemoperitoneum
- Erosion into uterine vessels → vaginal hemorrhage
- Sepsis if necrotic tumor infected → purulent discharge, pelvic pain
Treatment: Single-agent chemotherapy (methotrexate or actinomycin D) → high remission rate
Metastatic GTN — 4% after complete mole; more common after nonmolar pregnancies
GTN usually metastasizes as choriocarcinoma due to early vascular invasion and hematogenous spread.
| Metastatic Site | Frequency | Features |
|---|---|---|
| Lung | Most common | Cough, dyspnea, hemoptysis; pulmonary nodules on CXR |
| Vagina | Second most common | Dark hemorrhagic nodules; risk of massive bleeding |
| Brain | Serious; poor prognosis | Headache, seizures, focal deficits |
| Liver | Serious | RUQ pain, hepatomegaly |
Choriocarcinoma
- Highly invasive, frequently metastatic
- No chorionic villi histologically — sheets of anaplastic syncytiotrophoblast and cytotrophoblast
- Can follow any gestational event: molar pregnancy, spontaneous abortion, ectopic pregnancy, or term delivery
- After nonmolar pregnancies → always choriocarcinoma histologically
- Highly responsive to chemotherapy (unlike PSTT/ETT)
- Curable even with widespread metastases
FIGO Staging
| Stage | Definition |
|---|---|
| I | Disease confined to the uterus |
| II | GTN extends outside the uterus but limited to genital structures |
| III | GTN extends to the lungs ± genital involvement |
| IV | All other metastatic sites (brain, liver, etc.) |
Prognostic Scoring System
WHO/FIGO score based on: age, antecedent pregnancy, interval from index pregnancy, pre-treatment hCG level, largest tumor size, site of metastases, number of metastases, prior failed chemotherapy
- Low-risk (score 0–6): single-agent chemotherapy (MTX or actinomycin D); cure rate ~100%
- High-risk (score ≥7): combination chemotherapy (EMA-CO: etoposide, methotrexate, actinomycin D, cyclophosphamide, vincristine); cure rate ~90–95%
Placental Site Trophoblastic Tumor (PSTT) and Epithelioid Trophoblastic Tumor (ETT)
- Rare; composed of intermediate trophoblasts
- Produce small amounts of hCG and human placental lactogen (hPL)
- Tend to remain confined to uterus initially; metastasize late
- Relatively insensitive to chemotherapy — surgery (hysterectomy) is treatment of choice
- PSTT and ETT are the only GTD forms where hPL measurement (not hCG) is the primary marker
MOLAR PREGNANCY COEXISTING WITH NORMAL FETUS (Twin Molar Pregnancy)
- Occurs in 1 of 20,000–100,000 pregnancies
- One twin = complete mole; other = normal diploid fetus
- Associated complications: fetal death, hemorrhage, preeclampsia, persistent GTN after evacuation
- 60% who continue pregnancy experience spontaneous abortion or fetal demise before 24 weeks
- 40% deliver a live infant (most after 32 weeks)
- Rate of persistent GTN requiring chemotherapy: no different from singleton mole — not increased by continuing pregnancy
- Management: multidisciplinary (MFM + gynecologic oncology)
SUBSEQUENT PREGNANCIES AFTER GTD
| Situation | Outcomes |
|---|---|
| After hydatidiform mole (no GTN) | Normal pregnancy outcomes; no increased congenital abnormalities |
| After GTN treated with chemotherapy | Normal subsequent pregnancies; no increased fetal abnormalities |
| Recurrent molar pregnancy risk | Slightly elevated (1–2% after one mole) |
| Familial recurrent molar pregnancy | Rare; autosomal recessive (NLRP7, KHDC3L gene mutations); biparental diploid moles |
SUMMARY TABLE
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Karyotype | 46,XX / 46,XY (all paternal) | Triploid (69,XXX, 69,XXY) |
| Fetal tissue | Absent | Present (anomalous) |
| Classic US | Snowstorm | Focal Swiss cheese |
| hCG | Markedly elevated | Moderately elevated |
| Classic features | Common | Absent (looks like miscarriage) |
| GTN risk | 15–20% | 1–5% |
| Choriocarcinoma risk | 2.5% | Very rare |
| Contraception after | 12 months | 6 months |
| hCG surveillance | Weekly → monthly × 6 months | Until undetectable + 3 months |
KEY CLINICAL PEARLS
- Preeclampsia before 24 weeks = molar pregnancy until proven otherwise
- Hyperemesis out of proportion to gestational age → check hCG, do ultrasound for mole
- Partial moles are almost always misdiagnosed clinically as miscarriage — only confirmed on histology → send all POC specimens for pathology
- Do NOT use misoprostol alone for molar evacuation — risk of trophoblastic embolism and respiratory failure
- Treat hyperthyroidism before evacuation — anesthesia can trigger thyroid storm
- Theca lutein cysts do NOT need surgical removal — they regress within 2–4 months after hCG normalization
- hCG is the perfect tumor marker — use it for diagnosis, treatment monitoring, and recurrence detection
- Once hCG becomes undetectable after evacuation → risk of GTN approaches zero
- Phantom hCG: if hCG elevated but no pregnancy visible → run urine hCG to exclude false positive
- After GTN treated with chemotherapy → normal future pregnancies are expected — do not deny fertility
Sources: Berek & Novak's Gynecology; Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice; Rosen's Emergency Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Textbook of Family Medicine, 9th ed.
Make question on the above all topics
Here is a comprehensive question bank covering all topics discussed — Labor & Delivery, Ectopic Pregnancy, Molar Pregnancy, Miscarriage, Placental Abruption, Placenta Previa, PAS, Anatomy, and Hypertensive Disorders — in standard MCQ format with explanations.
Obstetrics Question Bank
All Topics — MCQ with Answers and Explanations
SECTION 1: OBSTETRIC ANATOMY & LABOR
Q1. A primigravida is in active labor. The fetal head is at the level of the ischial spines. What station is this?
- A) Station −2
- B) Station +1
- C) Station 0
- D) Station −1
✅ Answer: C — Station 0
The ischial spines are the reference point for station 0. Above the spines = negative station; below = positive.
Q2. Which of the following correctly describes the stages of labor?
- A) First stage: full dilation to delivery of baby
- B) Second stage: onset of contractions to full cervical dilation
- C) Third stage: delivery of baby to delivery of placenta
- D) Fourth stage: from onset of contractions to full dilation
✅ Answer: C
- 1st stage: onset of contractions → full dilation (10 cm)
- 2nd stage: full dilation → delivery of baby
- 3rd stage: delivery of baby → delivery of placenta
Q3. A nulliparous woman has been in the latent phase of labor for 22 hours. Which of the following is TRUE?
- A) Immediate cesarean section is indicated
- B) This is within normal limits for a nullipara
- C) The latent phase is considered prolonged; conservative management is appropriate
- D) Amniotomy should be performed immediately
✅ Answer: C
Normal latent phase limit is <20 hours (nullipara) and <14 hours (multipara). At 22 hours it is prolonged. Management is conservative — therapeutic rest (morphine), observation, ± oxytocin. This alone is NOT an indication for cesarean delivery. Amniotomy is avoided in latent phase (increases infection risk).
Q4. According to the Consortium on Safe Labor (Zhang et al.), the active phase of labor is reliably defined beginning at:
- A) 3 cm cervical dilation
- B) 4 cm cervical dilation
- C) 6 cm cervical dilation
- D) 8 cm cervical dilation
✅ Answer: C — 6 cm
Contemporary evidence (Zhang et al.) redefined active phase as starting at 6 cm, not 4 cm. Active-phase arrest should not be diagnosed before 6 cm.
Q5. Which pelvic type is most favorable for normal vaginal delivery?
- A) Android
- B) Anthropoid
- C) Platypelloid
- D) Gynecoid
✅ Answer: D — Gynecoid
Gynecoid (round inlet) occurs in ~50% of women and is most favorable. Android is associated with dystocia; platypelloid with transverse arrest; anthropoid with occiput posterior.
Q6. During the 3rd stage of labor, which of the following signs does NOT indicate placental separation?
- A) Gush of blood
- B) Cord lengthening
- C) Uterus becomes globular and firm
- D) Fetal heart rate returns to baseline
✅ Answer: D
Signs of placental separation: uterus becoming globular and firm, gush of blood from vagina, cord lengthening. FHR changes are fetal, not related to placental separation.
Q7. Misoprostol is used for cervical ripening. Which of the following is an ABSOLUTE contraindication to its use in the third trimester?
- A) Postdates pregnancy
- B) Prior low transverse cesarean section
- C) Multiparity
- D) PROM at term
✅ Answer: B — Prior uterine surgery (prior cesarean)
Misoprostol in the 3rd trimester in women with prior cesarean or major uterine surgery is associated with uterine rupture and is contraindicated.
Q8. A woman's BMI is 42 kg/m². Compared to a normal-weight nullipara, her first stage of labor is expected to be:
- A) The same duration
- B) More than 2 hours longer
- C) Shorter due to increased uterine tone
- D) 30 minutes longer
✅ Answer: B
Kominiarek et al. (Consortium on Safe Labor): BMI >40 kg/m² is associated with >2 hours longer first stage in nulliparous women.
SECTION 2: ECTOPIC PREGNANCY
Q9. Ectopic pregnancy is the leading cause of maternal death in which trimester?
- A) First trimester
- B) Second trimester
- C) Third trimester
- D) Equal across all trimesters
✅ Answer: A — First trimester
Ectopic pregnancy is the #1 cause of maternal death in the first trimester and the 3rd leading cause overall (4–10% of all maternal deaths).
Q10. A 28-year-old woman with amenorrhea for 6 weeks presents with pelvic pain and vaginal spotting. Urine hCG is positive. TVS shows an empty uterus. Serum hCG is 800 mIU/mL. What is the most appropriate next step?
- A) Diagnose ectopic pregnancy and administer methotrexate immediately
- B) Perform emergency laparoscopy
- C) Repeat hCG in 48 hours and repeat TVS when hCG rises above discriminatory zone
- D) Perform D&C immediately
✅ Answer: C
hCG is below the discriminatory zone (1,500–2,000 mIU/mL). An empty uterus below this level is indeterminate — could be very early IUP, failed IUP, or ectopic. Serial hCG in 48 hours is appropriate; ectopic cannot be diagnosed definitively yet from this data alone.
Q11. The discriminatory zone for transvaginal ultrasound is:
- A) 500–800 mIU/mL
- B) 1,500–2,000 mIU/mL
- C) 5,000–6,000 mIU/mL
- D) 10,000–15,000 mIU/mL
✅ Answer: B
At hCG ≥1,500–2,000 mIU/mL (TVS), an IUP should be visible. At this level with an empty uterus, ectopic pregnancy should be strongly suspected.
Q12. A patient's serial hCG rises 40% over 48 hours. What does this suggest?
- A) Normal viable intrauterine pregnancy
- B) Abnormal pregnancy — ectopic or failing IUP
- C) Normal variation within range
- D) Rapidly growing molar pregnancy
✅ Answer: B
Normal IUP hCG rises ≥66% in 48 hours. A rise of only 40% (below 66%) is abnormal — suggesting ectopic pregnancy or failing intrauterine pregnancy.
Q13. A serum progesterone level of 28 ng/mL in a patient with suspected ectopic pregnancy most likely indicates:
- A) Ectopic pregnancy
- B) Failing IUP
- C) Normal viable IUP
- D) Molar pregnancy
✅ Answer: C — Normal viable IUP
Progesterone >25 ng/mL → likely normal IUP (<2% are ectopic). Progesterone <15 ng/mL → seen in 81% of ectopics; <5 ng/mL → effectively excludes viable IUP.
Q14. Which of the following is an ABSOLUTE contraindication to methotrexate for ectopic pregnancy?
- A) hCG level of 3,000 mIU/mL
- B) Ectopic mass of 3.2 cm
- C) Breastfeeding
- D) No cardiac activity detected
✅ Answer: C — Breastfeeding
Absolute contraindications to MTX include: IUP, immunodeficiency, significant anemia/leukopenia/thrombocytopenia, MTX sensitivity, active pulmonary disease, active PUD, significant hepatic/renal dysfunction, breastfeeding, hemodynamic instability.
Q15. A patient received MTX for ectopic pregnancy 5 days ago. She now presents with moderate lower abdominal pain but is hemodynamically stable. hCG drawn today is decreasing appropriately. What is the most likely explanation?
- A) Treatment failure with impending rupture
- B) "Separation pain" — expected effect of MTX
- C) Allergic reaction to MTX
- D) Ovarian torsion
✅ Answer: B — Separation pain
Lower abdominal pain occurring 3–7 days after MTX is common ("separation pain") — from tubal abortion or hematoma formation. If patient is stable and hCG is decreasing → observe; NSAIDs for pain relief.
Q16. Which ectopic pregnancy location carries the highest mortality risk due to its rich blood supply and delayed rupture?
- A) Ampullary
- B) Fimbrial
- C) Isthmic
- D) Interstitial (cornual)
✅ Answer: D — Interstitial (cornual)
Interstitial ectopic lies within the myometrium (intramural tube), surrounded by myometrium. Rupture can occur at 9–16 weeks and causes massive hemorrhage due to the rich myometrial blood supply.
Q17. Which of the following findings on pelvic ultrasound is DIAGNOSTIC (not just suggestive) of ectopic pregnancy?
- A) Adnexal mass without intrauterine pregnancy
- B) Moderate free fluid in cul-de-sac
- C) Empty uterus with hCG above discriminatory zone
- D) Cardiac activity detected in the fallopian tube
✅ Answer: D
Ectopic cardiac activity = diagnostic. Options A and B are suggestive. Option C is indeterminate (highly suspicious but not diagnostic alone).
Q18. Heterotopic pregnancy (IUP + ectopic simultaneously) has an incidence of up to how much with IVF?
- A) 1 in 30,000
- B) 1 in 4,000
- C) 1 in 100
- D) 1 in 500
✅ Answer: C — up to 1 in 100 (1%) with IVF
Spontaneous rate: ~1/3,000 (historically 1/30,000). With IVF: up to 1%. Always consider heterotopic in ART patients even when IUP is confirmed on US.
SECTION 3: MOLAR PREGNANCY & GTD
Q19. A complete hydatidiform mole has which karyotype?
- A) 69,XXY (triploid)
- B) 46,XX (all maternal)
- C) 46,XX (all paternal — androgenetic)
- D) 45,X (monosomy)
✅ Answer: C — 46,XX all paternal (androgenetic)
Complete moles: 46,XX (90%) or 46,XY (10%), all chromosomes of paternal origin. Formed by fertilization of an empty ovum by one sperm (duplicates) or two sperm.
Q20. A partial mole has which karyotype?
- A) 46,XX all paternal
- B) 69,XXX or 69,XXY (triploid)
- C) 45,X (monosomy)
- D) 46,XY normal
✅ Answer: B — Triploid (69,XXX or 69,XXY)
Partial moles result from fertilization of a normal ovum by two sperm → triploid karyotype.
Q21. A 19-year-old presents at 16 weeks with vaginal bleeding. Ultrasound shows uterine size larger than expected for dates, no identifiable fetal heartbeat, and a "snowstorm" echogenic pattern filling the uterus. BP is 160/105 mmHg. What is the most likely diagnosis?
- A) Placenta previa
- B) Complete hydatidiform mole
- C) Placental abruption
- D) Threatened miscarriage
✅ Answer: B — Complete hydatidiform mole
Snowstorm US + uterine size > dates + preeclampsia before 24 weeks = pathognomonic for complete molar pregnancy. Preeclampsia before 24 weeks almost always means molar pregnancy.
Q22. Which of the following is the MOST important complication to monitor for after evacuation of a complete hydatidiform mole?
- A) Uterine rupture
- B) Cervical stenosis
- C) Persistent/rising serum hCG indicating GTN
- D) Ovarian failure from theca lutein cysts
✅ Answer: C — Persistent/rising hCG indicating GTN
After complete mole evacuation: 15–20% develop GTN (local invasion or metastasis). Weekly hCG monitoring is essential. Any plateau, rise, or persistence beyond 6 months → GTN → oncology referral.
Q23. What is the risk of choriocarcinoma specifically after a complete hydatidiform mole?
- A) 15–20%
- B) 2.5%
- C) 10%
- D) 0.5%
✅ Answer: B — 2.5%
Complete mole: local invasion (invasive mole) in 15%, metastasis in 4%, choriocarcinoma specifically ~2.5%.
Q24. A patient who had a complete molar pregnancy asks when she can attempt pregnancy. After achieving hCG remission, she should wait:
- A) 3 months
- B) 6 months
- C) 12 months (1 year)
- D) 2 years
✅ Answer: C — 12 months
After complete mole → avoid pregnancy for 1 year after hCG remission to allow adequate serial hCG monitoring without confusion from pregnancy hCG.
Q25. Which of the following is a HIGH-RISK marker for developing post-molar GTN?
- A) Uterine size equal to dates
- B) hCG of 50,000 mIU/mL
- C) hCG >100,000 mIU/mL + uterine size > dates + theca lutein cysts ≥6 cm
- D) Age under 30
✅ Answer: C
Three high-risk signs: hCG >100,000 mIU/mL, excessive uterine size, theca lutein cysts ≥6 cm. Patients with any one of these: local invasion 31%, metastases 8.8%.
Q26. Why is misoprostol-only uterine evacuation NOT preferred for molar pregnancy?
- A) Insufficient cervical ripening
- B) Risk of incomplete evacuation, hemorrhage, infection, and trophoblastic pulmonary embolism
- C) It is too expensive
- D) It does not work before 12 weeks
✅ Answer: B
Medical evacuation risks: incomplete evacuation (up to 25%), hemorrhage, infection, trophoblastic embolization → respiratory failure and death. Suction curettage is preferred.
Q27. A patient with complete molar pregnancy has a serum hCG of 200,000 mIU/mL and is tachycardic with warm skin and tremor before evacuation. What must be done BEFORE proceeding to the operating room?
- A) Administer misoprostol for cervical ripening
- B) Administer β-adrenergic blocking agents to prevent thyroid storm
- C) Give IV methotrexate
- D) Place cervical cerclage
✅ Answer: B — β-blockers before evacuation
Clinically evident hyperthyroidism (from hCG's TSH-like activity) → anesthesia/surgery can precipitate thyroid storm (hyperthermia, delirium, tachycardia, cardiovascular collapse). Must treat with β-blockers before proceeding.
SECTION 4: MISCARRIAGE (SPONTANEOUS ABORTION)
Q28. A patient at 8 weeks presents with light vaginal bleeding. TVS shows a gestational sac with a fetal pole showing cardiac activity. Cervix is closed. What is the diagnosis?
- A) Inevitable abortion
- B) Threatened abortion
- C) Missed abortion
- D) Incomplete abortion
✅ Answer: B — Threatened abortion
Threatened: bleeding + closed cervix + viable IUP on US. ~50% will continue to term.
Q29. Which of the following is the most common cause of first-trimester spontaneous abortion?
- A) Uterine septum
- B) Antiphospholipid syndrome
- C) Chromosomal abnormalities
- D) Luteal phase defect
✅ Answer: C — Chromosomal abnormalities
~50–60% of first-trimester losses have chromosomal abnormalities. Trisomies are most common; trisomy 16 is the most frequent.
Q30. An embryo with a crown-rump length of 8 mm on TVS with no cardiac activity. What is the diagnosis?
- A) Threatened miscarriage
- B) Nonviable (embryonic demise / missed abortion)
- C) Normal — cardiac activity not expected until 10 weeks
- D) Partial molar pregnancy
✅ Answer: B — Nonviable
Absent cardiac activity when CRL ≥7 mm on TVS = nonviable pregnancy (embryonic demise).
Q31. Which type of miscarriage is the most treatable cause of recurrent pregnancy loss?
- A) Chromosomal aneuploidy
- B) Antiphospholipid syndrome (APS)
- C) Uterine septum
- D) Advanced maternal age
✅ Answer: B — Antiphospholipid syndrome
APS is the most treatable cause of recurrent miscarriage — treated with aspirin ± heparin during pregnancy with good outcomes.
Q32. A patient presents with vaginal bleeding, dilated cervix, and products of conception palpable at the os. She is hemodynamically stable. What is the diagnosis?
- A) Missed abortion
- B) Incomplete abortion
- C) Inevitable abortion
- D) Threatened abortion
✅ Answer: C — Inevitable abortion
Inevitable: bleeding + dilated cervix + POC not yet passed. Once POC partially expelled with open cervix = incomplete.
Q33. What is the dose of misoprostol for medical management of missed or incomplete abortion?
- A) 25 µg orally
- B) 200 µg orally
- C) 800 µg vaginally
- D) 400 µg sublingually only
✅ Answer: C — 800 µg vaginally
Standard dose for missed/incomplete/inevitable abortion: 800 µg vaginally. (Note: 25 µg vaginally is for labor induction at term.)
SECTION 5: PLACENTAL ABRUPTION
Q34. What is the hallmark clinical feature of placental abruption?
- A) Painless bright red bleeding
- B) Sudden fetal tachycardia with no bleeding
- C) Painful dark vaginal bleeding
- D) Rupture of membranes with bloody fluid
✅ Answer: C — Painful dark vaginal bleeding
Abruption hallmark = painful (uterine tenderness) + dark blood. Contrasts with previa (painless, bright red).
Q35. Approximately what percentage of placental abruptions present with NO external (vaginal) bleeding?
- A) 1–2%
- B) 5%
- C) 10–20% (concealed hemorrhage)
- D) 50%
✅ Answer: C — 10–20%
Up to 10–20% of abruptions are concealed — all hemorrhage is retroplacental with no external bleeding, yet massive internal blood loss may be occurring.
Q36. The MOST important risk factor for placental abruption (highest relative risk increase) is:
- A) Maternal hypertension
- B) Cocaine use
- C) Prior placental abruption
- D) Cigarette smoking
✅ Answer: C — Prior placental abruption
Previous abruption → up to 20-fold increased risk; with 2 prior abruptions → 25% recurrence risk. Chronic hypertension → 5× risk, superimposed preeclampsia → 8×.
Q37. Which laboratory test is the MOST SENSITIVE for detecting DIC in placental abruption?
- A) Platelet count
- B) Prothrombin time
- C) Fibrin degradation products (FDP)
- D) Hemoglobin level
✅ Answer: C — Fibrin degradation products
FDP are "almost always elevated" in abruption-related DIC and are the most sensitive lab test. Fibrinogen is the most important serial monitor.
Q38. A patient at 28 weeks has moderate abruption. The mother is stable, fetal monitoring is reassuring, and there is no coagulopathy. The most appropriate management is:
- A) Immediate cesarean delivery
- B) Expectant management with betamethasone, close monitoring
- C) Induction of labor with oxytocin
- D) Tocolysis with magnesium and discharge home
✅ Answer: B
At 20–34 weeks with stable mother and fetus → expectant management is appropriate. Betamethasone given for fetal lung maturity. Patient monitored closely — she remains at risk for evolving abruption.
Q39. A patient is in a motor vehicle accident at 30 weeks. She has no pain or bleeding. When can she safely be discharged?
- A) Immediately after examination
- B) After 2 hours of monitoring
- C) After 6 hours of continuous CTG monitoring if reassuring
- D) After 24 hours regardless of symptoms
✅ Answer: C — 6 hours of monitoring
Asymptomatic after trauma → monitor CTG for minimum 6 hours; if reassuring → discharge. If bleeding or contractions → observe at least 24 hours (abruption may present up to 24 hours post-trauma).
Q40. What is Couvelaire uterus?
- A) Placenta completely covering the cervical os
- B) Uterus infiltrated with blood penetrating through the myometrium to the peritoneum
- C) Uterine rupture from prior cesarean scar
- D) Abnormal placental attachment to the myometrium
✅ Answer: B
Couvelaire uterus (uteroplacental apoplexy): retroplacental blood penetrates the full uterine wall thickness into the peritoneal cavity. Myometrium becomes bruised and atonic → risk of PPH.
Q41. Normal fibrinogen level in pregnancy is:
- A) 150–250 mg/dL
- B) 200–300 mg/dL
- C) 400–650 mg/dL
- D) 100–150 mg/dL
✅ Answer: C — 400–650 mg/dL
Normal fibrinogen in pregnancy is elevated (400–650 mg/dL). Values <300 mg/dL indicate significant coagulopathy. In severe abruption: fibrinogen <150 mg/dL.
SECTION 6: PLACENTA PREVIA
Q42. A patient at 24 weeks presents with painless bright red vaginal bleeding. The emergency physician wants to perform a digital vaginal examination to assess the cervix. What should you do?
- A) Allow the examination — it is safe
- B) Perform a speculum examination first to identify source of bleeding
- C) Immediately perform digital exam to assess dilation
- D) Stop — do NOT perform digital examination until placenta previa is excluded by ultrasound
✅ Answer: D — Absolutely no digital examination
Digital examination in placenta previa can precipitate catastrophic, life-threatening hemorrhage. US must exclude previa first.
Q43. At 18 weeks gestation, routine anatomy scan shows the placenta completely overlying the internal cervical os. What should the patient be told?
- A) She will definitely need a cesarean delivery
- B) She has placenta previa and needs immediate hospitalization
- C) 90% of 2nd trimester previas resolve by term — follow-up US at 32 weeks
- D) She needs cervical cerclage placement immediately
✅ Answer: C
At 16 weeks, placenta occupies 25–50% of uterine surface. 90% of complete previas found in 2nd trimester resolve by term due to trophotropism and LUS elongation. Follow-up at 32 weeks, then 36 weeks.
Q44. Why does the bladder need to be EMPTY before performing TVS for suspected placenta previa?
- A) Full bladder prevents adequate TVS imaging
- B) Full bladder pushes uterine walls together, creating a false-positive previa diagnosis
- C) Full bladder prevents the probe from being inserted
- D) Full bladder increases the risk of hemorrhage
✅ Answer: B
A full bladder compresses the lower uterine segment, pushing the anterior and posterior walls together → artificially makes placenta appear to cover the os (false-positive previa).
Q45. Placenta previa is confirmed at 36 weeks. The patient is stable with no active bleeding. What is the appropriate delivery plan?
- A) Allow labor to begin spontaneously
- B) Cesarean delivery now — do not delay
- C) Elective cesarean at or just after 36 weeks gestation
- D) Await spontaneous labor at 40 weeks
✅ Answer: C
Elective cesarean at 36–37 weeks for confirmed previa — risk of sudden, potentially fatal hemorrhage outweighs any fetal advantage of waiting beyond 36 weeks. Amniocentesis for lung maturity not needed.
Q46. The lower uterine segment (LUS) does NOT contract as effectively as the upper uterus after placental delivery. What complication does this cause in placenta previa?
- A) Uterine rupture
- B) Postpartum hemorrhage from LUS atony
- C) Cervical laceration
- D) Placenta accreta
✅ Answer: B — PPH from LUS atony
The LUS (where previa implants) has poor contractile ability → placental bed does not close properly after delivery → PPH. Anticipate with uterotonics (oxytocin, Methergine, carboprost, B-Lynch suture, Bakri balloon).
Q47. Which of the following about vasa previa is TRUE?
- A) It is associated with fundal placental implantation
- B) Fetal survival is 97% with antenatal diagnosis vs. 44% without
- C) Management is expectant until term
- D) The vessels are protected by Wharton's jelly
✅ Answer: B
With antenatal diagnosis → planned cesarean → 97% neonatal survival. Without diagnosis → membrane rupture tears unprotected fetal vessels → exsanguination in minutes → only 44% survival. Vessels in vasa previa are NOT supported by Wharton's jelly (that's the danger).
SECTION 7: PLACENTA ACCRETA SPECTRUM (PAS)
Q48. A woman with her 4th cesarean delivery has an anterior placenta previa. What is her approximate risk of placenta accreta?
- A) 3%
- B) 11%
- C) 40%
- D) 61%
✅ Answer: D — 61%
With placenta previa and 4th cesarean (≥3 prior C/S) → risk of accreta = 61–67%. This is the critical risk table to memorize.
Q49. Which layer's absence allows trophoblasts to invade the myometrium in PAS?
- A) Wharton's jelly
- B) Nitabuch fibrinoid layer (decidua basalis)
- C) Chorion laeve
- D) Amnion
✅ Answer: B — Nitabuch fibrinoid layer
Normally the Nitabuch layer in the decidua basalis acts as a barrier to trophoblast invasion. In PAS, this layer is absent or deficient (from prior uterine scar) → trophoblasts invade freely.
Q50. Which ultrasound finding is most characteristic of placenta accreta?
- A) Placenta completely covering the os
- B) Loss of retroplacental hypoechoic zone + placental lacunae ("Swiss cheese" appearance)
- C) Posterior placenta with normal clear zone
- D) Theca lutein cysts
✅ Answer: B
Key US findings: loss of the normal retroplacental hypoechoic "clear zone" + irregular hypoechoic lacunae (Swiss cheese/snowstorm) within the placenta + bridging vessels + <1mm myometrial thickness.
Q51. What is the recommended gestational age for planned delivery of confirmed PAS?
- A) 28–30 weeks
- B) 34–35 weeks after corticosteroids
- C) 38–40 weeks
- D) 32 weeks
✅ Answer: B — 34–35 weeks
Planned delivery at 34–35 weeks (after betamethasone for lung maturity). Rationale: before labor begins; planned reduces hemorrhage risk dramatically vs. emergency delivery. No amniocentesis for lung maturity needed.
Q52. Which of the following is the DEFINITIVE treatment for PAS?
- A) Manual placental removal at cesarean
- B) Misoprostol + oxytocin to facilitate placental separation
- C) Planned cesarean hysterectomy with placenta left in situ
- D) Uterine artery embolization alone
✅ Answer: C
Placenta left in situ → cesarean hysterectomy. Attempting manual removal causes catastrophic hemorrhage as placenta fragments. UAE is an adjunct, not definitive treatment.
Q53. Methotrexate is used for conservative management of PAS. Which of the following is TRUE?
- A) MTX is highly effective for PAS and should be used routinely
- B) MTX is unequivocally NOT recommended — no proven efficacy and one death reported from complications
- C) MTX should be given prophylactically after every cesarean
- D) MTX replaces the need for serial hCG monitoring
✅ Answer: B
Berek & Novak / Creasy & Resnik: "Methotrexate is unequivocally not advised for conservative management of accreta" — no proven benefit and a death has been reported from MTX complications in this setting.
SECTION 8: HYPERTENSIVE DISORDERS OF PREGNANCY
Q54. Preeclampsia is defined as:
- A) BP ≥140/90 after 20 weeks with no proteinuria
- B) BP ≥140/90 after 20 weeks + proteinuria >300 mg/24 hr (or PCR ≥0.3)
- C) BP ≥160/110 at any time in pregnancy
- D) Chronic HTN diagnosed before pregnancy
✅ Answer: B
Preeclampsia = BP ≥140/90 on two occasions ≥4 hours apart, after 20 weeks, AND proteinuria >300 mg/24 hr (or PCR ≥0.3, or dipstick ≥2+). Note: edema is no longer a criterion.
Q55. Which of the following is a feature of preeclampsia WITH SEVERE FEATURES?
- A) BP of 138/88 mmHg
- B) Proteinuria of 250 mg/24 hours
- C) Platelet count of 85,000/µL
- D) Creatinine of 0.9 mg/dL
✅ Answer: C — Thrombocytopenia (<100,000/µL)
Severe features include: SBP ≥160 or DBP ≥110, thrombocytopenia (<100,000/µL), renal insufficiency (Cr >1.1 or doubling), impaired liver function (transaminases ×2), pulmonary edema, new-onset headache, visual disturbances, oliguria (<500 mL/24h).
Q56. A patient with preeclampsia with severe features at 37 weeks. What is the appropriate management?
- A) Expectant management until 40 weeks
- B) Deliver within 24 hours + IV magnesium sulfate
- C) Start antihypertensives and monitor weekly
- D) Immediate cesarean only
✅ Answer: B
Severe preeclampsia at any gestation requires delivery within 24 hours + IV MgSO₄ for seizure prophylaxis. Route of delivery based on obstetric indications (not always cesarean).
Q57. What is the magnesium sulfate loading dose for preeclampsia seizure prophylaxis?
- A) 2 g IV over 30 minutes
- B) 4–6 g IV over 15–20 minutes, then 2 g/hr maintenance
- C) 10 g IM
- D) 1 g/hr from the start
✅ Answer: B
MgSO₄ protocol: loading dose 4–6 g IV over 15–20 min, then maintenance 1–3 g/hr (therapeutic level 5–8 mg/dL). Continue for 24 hours postpartum.
Q58. The FIRST sign of magnesium sulfate toxicity is:
- A) Respiratory depression
- B) Cardiac arrest
- C) Loss of deep tendon reflexes (DTRs)
- D) Urine output decreasing
✅ Answer: C — Loss of deep tendon reflexes
Mg toxicity signs in order: loss of DTRs (~7–10 mg/dL) → respiratory depression (~15 mg/dL) → cardiac arrest (~20 mg/dL). Monitor DTRs, RR, and urine output.
Q59. What is the antidote for magnesium sulfate toxicity?
- A) Naloxone 0.4 mg IV
- B) Calcium gluconate 1 g IV
- C) Furosemide 40 mg IV
- D) Flumazenil
✅ Answer: B — Calcium gluconate 1 g IV
Calcium gluconate reverses MgSO₄ toxicity. Must always be at the bedside when MgSO₄ is infusing.
Q60. HELLP syndrome is diagnosed by which combination of findings?
- A) Hypertension + edema + leukocytosis
- B) Hemolysis + elevated liver enzymes + low platelets
- C) Hypotension + elevated LFTs + high platelets
- D) Hematuria + elevated creatinine + low BP
✅ Answer: B
HELLP = Hemolysis + Elevated Liver enzymes + Low Platelets. Occurs in 5–10% of preeclamptic patients. Often presents with RUQ/epigastric pain — can occur WITHOUT severe HTN or proteinuria.
Q61. Eclampsia is defined as:
- A) Hypertension >160/110 in pregnancy
- B) Preeclampsia + new-onset grand mal seizures not attributable to other causes
- C) HELLP syndrome with severe hypertension
- D) Hypertensive emergency in the 1st trimester
✅ Answer: B
Eclampsia = preeclampsia + grand mal (tonic-clonic) seizures not explained by other conditions. Can occur antepartum (most common), intrapartum, or up to 7 days postpartum. MgSO₄ is the drug of choice.
Q62. Which antihypertensive medications are CONTRAINDICATED in pregnancy?
- A) Labetalol and methyldopa
- B) Nifedipine and hydralazine
- C) ACE inhibitors and ARBs
- D) Beta-blockers and calcium channel blockers
✅ Answer: C — ACE inhibitors and ARBs
ACE inhibitors and ARBs are absolutely contraindicated — fetotoxic (renal tubular dysgenesis, oligohydramnios, pulmonary hypoplasia, fetal death). Safe options: methyldopa, labetalol, nifedipine, hydralazine.
Q63. A pregnant patient has BP 168/112 mmHg. According to protocol, which IV medication should be given for acute severe hypertension?
- A) Furosemide IV
- B) IV labetalol or IV hydralazine
- C) IV enalapril
- D) Oral amlodipine
✅ Answer: B — IV labetalol or IV hydralazine
For acute severe HTN in pregnancy (DBP persistently >110 mmHg): IV labetalol or IV hydralazine; oral nifedipine is also acceptable. Target: DBP <105 mmHg (not aggressively lower — risk of placental ischemia).
Q64. The treatment of choice for chronic hypertension in pregnancy is:
- A) Lisinopril
- B) Valsartan
- C) α-methyldopa (Aldomet) or labetalol
- D) Atenolol
✅ Answer: C
First-line for chronic HTN in pregnancy: α-methyldopa (Aldomet) — central-acting α-adrenergic; or labetalol — α and β blocker. Both have long safety records. ACE inhibitors/ARBs are contraindicated; atenolol associated with IUGR.
SECTION 9: MIXED / INTEGRATED QUESTIONS
Q65. A woman at 30 weeks presents with painless bright red vaginal bleeding. Uterus is soft and non-tender. Fetal heart rate is normal. The FIRST action should be:
- A) Perform digital cervical examination
- B) Obtain IV access, continuous CTG, and perform transabdominal US — DO NOT perform digital exam
- C) Immediate cesarean delivery
- D) Perform amniotomy
✅ Answer: B
Painless bright red bleeding → suspect placenta previa → no digital exam. Stabilize, CTG, US to confirm. Digital exam only when previa excluded.
Q66. Which of the following conditions is NOT associated with preeclampsia before 24 weeks?
- A) Complete molar pregnancy
- B) Multiple gestation
- C) Placenta accreta
- D) Antiphospholipid syndrome
✅ Answer: C — Placenta accreta
Preeclampsia before 24 weeks is associated with: complete molar pregnancy (most classically), multiple gestation, antiphospholipid syndrome, hydrops fetalis, and other causes of exaggerated placentation. PAS itself does not typically cause early preeclampsia.
Q67. The MOST common cause of peripartum hysterectomy is:
- A) Uterine rupture
- B) Placenta previa alone
- C) Placenta accreta spectrum
- D) Postpartum hemorrhage from uterine atony
✅ Answer: C — Placenta accreta spectrum
PAS is the most common indication for emergency peripartum hysterectomy in the modern obstetric era.
Q68. Which of the following pairs is CORRECTLY matched?
- A) Abruption → painless bright red bleeding
- B) Previa → painful dark bleeding + rigid uterus
- C) Abruption → painful dark bleeding + hypertonic uterus
- D) Vasa previa → maternal hemorrhage without fetal distress
✅ Answer: C
- Abruption: painful, dark blood, hypertonic/tender uterus
- Previa: painless, bright red, soft uterus
- Vasa previa: fetal hemorrhage (fetal blood vessels) → fetal distress + bleeding when membranes rupture
Q69. What is the "snowstorm" appearance on ultrasound associated with?
- A) Placenta accreta
- B) Complete hydatidiform mole
- C) Placental abruption
- D) Dichorionic twin pregnancy
✅ Answer: B — Complete hydatidiform mole
Snowstorm = echogenic mass with multiple small anechoic (cystic) spaces, no fetal parts = classic complete mole appearance.
Q70. Rh immune globulin (300 µg) should be administered in which of the following obstetric scenarios?
- A) Rh-negative patient with placenta previa and heavy bleeding who has NOT yet received her 28-week dose
- B) Rh-positive patient with placental abruption
- C) Rh-negative patient who received their 28-week prophylaxis and now has threatened miscarriage
- D) All pregnant patients regardless of Rh status
✅ Answer: A
Rh immune globulin should be given to Rh-negative, non-immunized women who have not yet received their 28-week dose and are now bleeding (previa, abruption, ectopic, miscarriage, trauma). Given within 72 hours of the event.
SCORING GUIDE
| Score | Level |
|---|---|
| 63–70 | Excellent — Mastery level |
| 50–62 | Good — Minor review needed |
| 35–49 | Fair — Systematic topic review needed |
| <35 | Needs comprehensive review |
Questions based on: Creasy & Resnik's Maternal-Fetal Medicine; Berek & Novak's Gynecology; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Textbook of Family Medicine 9e; Robbins & Cotran Pathologic Basis of Disease.
Earliest cardinal movement of labour is and why
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have all the content needed directly from the textbooks. Here is the complete, detailed answer:
The Earliest Cardinal Movement of Labor — ENGAGEMENT
The Cardinal Movements — Full Sequence
The cardinal movements (mechanisms of labor) describe the series of positional changes the fetal head makes to navigate the maternal pelvis. In order:
| Order | Movement |
|---|---|
| 1. Engagement ← Earliest | Descent of the biparietal diameter (BPD) below the pelvic inlet |
| 2. Descent | Continuous progressive downward movement |
| 3. Flexion | Head flexes, chin to chest |
| 4. Internal rotation | Head rotates to OA position |
| 5. Extension | Head extends around pubic symphysis → delivery |
| 6. External rotation (Restitution) | Head rotates back to transverse after delivery |
| 7. Expulsion | Delivery of shoulders and body |
ENGAGEMENT — Why It Is the Earliest and What It Means
Definition
"Engagement is defined by descent of the biparietal diameter of the fetus to a level below the maternal pelvic inlet." — Pfenninger and Fowler's Procedures for Primary Care
Engagement = the widest transverse diameter of the fetal head (biparietal diameter, BPD ~9.5 cm) has passed through and descended below the plane of the pelvic inlet.
Clinical Recognition
- Clinically suggested when the lowest portion of the occiput (not caput succedaneum) is at or below the level of the ischial spines = Station 0
- On abdominal palpation: the head is no longer ballottable / freely mobile; it is "fixed" in the pelvis — only 2/5 or less of the head is palpable abdominally
- The fundal height drops ("lightening") — the mother notices she can breathe more easily but has increased pelvic pressure
Why Engagement Occurs FIRST — The Anatomic Reason
The sequence of cardinal movements is dictated by the shape of the maternal pelvis. The fetal head must adapt to the different diameters it encounters at each level:
At the pelvic inlet:
- The transverse diameter is the widest dimension of the inlet
- The anteroposterior (AP) / obstetric conjugate is the narrowest dimension of the inlet (~10–11 cm)
- Therefore, the fetal head must enter the inlet in the transverse (or oblique) diameter — biparietal diameter aligning with the widest transverse dimension
- The biparietal diameter (BPD ≈9.5 cm) must fit through the obstetric conjugate (≥10 cm)
"In most cases, the anteroposterior diameter of the pelvic inlet is the smallest dimension. Thus, the smallest diameter of the fetal head (biparietal diameter) must align with the anteroposterior diameter of the pelvic inlet." — Pfenninger and Fowler's Procedures for Primary Care
This is why engagement must happen before any other movement can begin — until the head clears the inlet, descent, flexion, and rotation cannot proceed.
Simply put:
- No engagement → no labor progress
- Engagement confirms that the pelvic inlet is adequate to allow fetal descent
- It is the gatekeeper — the head must first pass the narrowest dimension at the inlet before all subsequent movements occur
When Does Engagement Occur?
| Parity | Timing |
|---|---|
| Nulliparas (first-time mothers) | Often occurs 2–4 weeks before onset of labor ("lightening") |
| Multiparas | Often does NOT occur until active labor begins (pelvis already proven; soft tissue more lax) |
"Often occurs before the onset of labor, especially in nulliparas." — Pfenninger and Fowler's Procedures for Primary Care
This is clinically important:
- In a nullipara at 38 weeks with a non-engaged head → consider pelvic inadequacy (android pelvis, cephalopelvic disproportion)
- In a multipara → non-engagement before labor is normal and not concerning
What Happens to the Head at Engagement — The Position
At engagement, the fetal head enters in one of the oblique diameters of the inlet:
- Left occipitotransverse (LOT) — most common (~40%)
- Left occipitoanterior (LOA) — second most common
- Right occipitotransverse (ROT), Right occipitoanterior (ROA) — less common
- Occipitoposterior (OP) — ~5–10% — less favorable, often results in longer, more painful labor
At engagement, the head is usually in a neutral or slightly flexed position. Full flexion comes with the next movement.
Clinical Significance of Non-Engagement
| Situation | Significance |
|---|---|
| Non-engagement at term in nullipara | Warrants evaluation for CPD (cephalopelvic disproportion), pelvic shape (android pelvis), fetal macrosomia, or abnormal fetal position |
| Verification difficulty | If fetal head is molded (bones overlapping) or in OP position, station may be overestimated clinically |
| "Floating head" at term | Requires ultrasound to rule out placenta previa before digital examination |
Why the Sequence Proceeds in This Order — Summary
Each movement is forced by the shape of the pelvis at that level:
| Level | Widest Diameter | Narrowest Diameter | Fetal Head Response |
|---|---|---|---|
| Inlet | Transverse | AP (obstetric conjugate) | Engagement in transverse/oblique |
| Mid-pelvis | AP | Transverse (bispinous) | Internal rotation to bring occiput anterior |
| Outlet | AP (intertuberous) | — | Extension around pubic symphysis |
| After outlet | — | — | External rotation — head realigns with shoulders |
"As the fetal head continues to descend, the biparietal diameter of the fetus rotates to align with the lateral diameter (intertuberous diameter) of the maternal pelvic outlet." — Pfenninger and Fowler's Procedures for Primary Care
Engagement must come first because:
- It is the entry of the presenting part into the pelvis — before this, the fetus is entirely above the pelvis
- Without clearing the inlet, no subsequent movement is anatomically possible
- It confirms pelvic adequacy at the inlet level — a critical obstetric gate
Summary Answer
| Question | Answer |
|---|---|
| Earliest cardinal movement | Engagement |
| Why earliest? | The fetal BPD must first cross the pelvic inlet (the narrowest anteroposterior diameter) before any other descent or positional change can occur — it is anatomically the first gate the fetus must pass |
| Clinical sign | Head at or below ischial spines (Station 0); lightening; head no longer freely ballottable |
| When in nulliparas | 2–4 weeks before labor |
| When in multiparas | Usually at onset of active labor |
| Position at engagement | Usually left occipitotransverse (LOT) — BPD in transverse diameter of inlet |
Sources: Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.; Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice.
This is a shared conversation. Sign in to Orris to start your own chat.