Femroacetubular impingement
Reading File
Finding Sources
Finding Sources
Searching Images
femoroacetabular impingement FAI cam pincer hip
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Femoroacetabular Impingement (FAI):
Femoroacetabular Impingement (FAI)
Definition: Abnormal mechanical contact between the proximal femur and acetabulum that causes chondral damage and symptoms, often progressing to labral tears and osteoarthritis if untreated.
— Miller's Review of Orthopaedics, 9th Ed.
Types
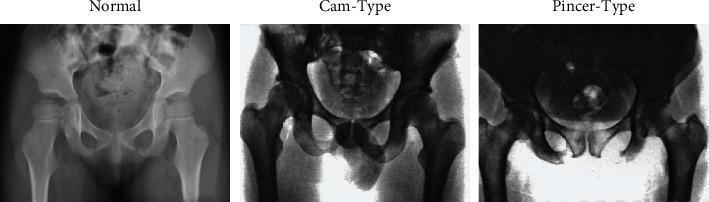
1. Cam Impingement (Femoral-side problem)
- A bony prominence at the femoral head-neck junction reduces the normal concave offset (reduced head-neck ratio)
- Caused by aspherical femoral head, slipped capital femoral epiphysis deformity, or pistol-grip deformity
- α-angle is used to quantify head-neck offset — normally ≤40°; elevated in cam FAI
- Produces shearing delamination of acetabular cartilage, especially at the anterosuperior quadrant
- More common in young males
2. Pincer Impingement (Acetabular-side problem)
- Caused by acetabular overcoverage — the rim extends too far over the femoral head
- Mechanisms: protrusio acetabuli, coxa profunda, or acetabular retroversion (crossover sign on X-ray)
- Results in intrasubstance labral tears (typically anterosuperior)
- A contrecoup cartilage lesion may occur posteroinferiorly ("levering" effect)
- More common in middle-aged females
3. Combined (Mixed) Type
- Most common presentation — features of both cam and pincer morphology
Clinical Presentation
- Groin or anterior hip pain, worsened by hip flexion activities and prolonged sitting
- Grinding or popping sensation
- Decreased internal rotation (out of proportion to other ROM losses)
- Impingement test (FADIR): Passive flexion to 90° + adduction + internal rotation → reproduces groin pain (almost always positive)
- More passive external rotation than internal rotation on exam
Imaging
| Modality | Findings |
|---|---|
| AP pelvis X-ray | Pistol-grip deformity (cam), crossover sign (pincer retroversion), coxa profunda/protrusio |
| 45° Dunn lateral | Preferred lateral view for most hip arthroscopy surgeons |
| False profile view | Anterior coverage, subspine deformities, joint space narrowing |
| CT scan | Detailed femur-acetabulum mismatch; 3D morphology |
| MR arthrogram | Best for labral tears and cartilaginous injury |
Caveat: >90% of asymptomatic adolescents have at least one radiographic FAI parameter, and 50% have two — imaging must be interpreted in clinical context.
Pathological Consequences
- Labral tears (pincer mechanism)
- Acetabular cartilage delamination (cam mechanism)
- Progressive osteoarthritis if untreated
Treatment
Conservative
- Activity modification, physiotherapy, NSAIDs
- Diagnostic/therapeutic intra-articular injections
Surgical
- Hip arthroscopy (most common): femoral head-neck osteoplasty (cam resection), acetabular rim trimming, labral repair
- Labral repair is preferred over débridement (superior outcomes)
- Median return to sport: ~6 months
- Surgical hip dislocation (Ganz trochanteric osteotomy): for severe deformities requiring full exposure
- Periacetabular osteotomy (PAO) or femoral osteotomy for complex morphological correction
Poor Prognostic Factors
- Tönnis grade 2+ arthritic changes
- Joint space <2 mm → increased risk of conversion to total hip arthroplasty (THA)
Sources: Miller's Review of Orthopaedics 9th Ed. | Schwartz's Principles of Surgery 11th Ed. | Grainger & Allison's Diagnostic Radiology | Imaging Anatomy Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.